Abordarea diagnostică şi terapeutică a placentei invazive
Diagnostic and therapeutical approach of the invasive placenta
Abstract
Adherent placenta incidence has increased in the last 60 years from 1/30000 pregnancies to 1/700 pregnancies. The increased index of the caesarean section supports this pathology. Uncontrollable bleeding due to the invasive placenta is one of the main indications of per partum hysterectomy and a major cause of disseminated intravascular coagulopathy, adult respiratory distress syndrome, kidney failure and maternal mortality. Although ultrasound diagnosis has a sensitivity considered to be 90% and a specificity of 97% with a positive real rate appreciated at 11 and a negative real rate of 0.16, magnetic resonance imaging is widely available and has a high diagnostic accuracy. In current practice prevails an inadvertently and an unreasonably high report between prenatal and the intraoperative diagnosis. Discussing the cases from the last 2 years of experience in a multidisciplinary emergency hospital, we present a broad review of the literature with the purpose of giving a coherent and standardized approach of the patients with risk factors. As well, the current methods for optimal therapeutic approach will be presented.Keywords
adherent placentauterine embolizationRezumat
Incidenţa placentei aderente a crescut în ultimii 60 de ani de la 1/30000 de sarcini la 1/700 de sarcini, creşterea indicelui de cezariană favorizând această patologie. Hemoragia incontrolabilă datorată placentatiei invazive reprezintă una dintre principalele indicaţii ale histerectomiei peripartum şi o cauză majoră de coagulopatie intravasculară diseminată, detresă respiratorie a adultului, insuficienţă renală şi mortalitate maternă. Deşi diagnosticul ecografic are o sensibilitate considerată a fi de 90% şi o specificitate de 97%, cu o rată de real pozitiv apreciată la 11 şi o rată de real negativ de 0,16, deşi rezonanţa magnetică este larg disponibilă şi are acurateţe diagnostică înaltă, practica demonstrează un raport de inadvertenţă nejusticat de mare între diagnosticul prenatal şi cel intraoperator. Discutând experienţa cazurilor ultimilor 2 ani într-un spital pluridisciplinar de urgenţă, prezentăm o largă revizie a literaturii de specialitate în scopul formulării unei abordari coerente şi standardizate a pacientelor cu factori de risc, precum şi a metodelor actuale optime de abordare terapeutică.Cuvinte Cheie
placentă aderentăembolizare uterinăIntroducere
Formarea şi dezvoltarea placentei reprezintă un proces de complexitate înaltă. Rolul fundamental al placentei în dezvoltarea fetală şi pentru evoluţia normală a sarcinii face ca orice modificare patologică morfologică sau funcţională să reprezinte o problemă de importanţă majoră. Funcţia definitorie a placentei este cea de transfer: oxigen, nutrienţi, anticorpi, hormoni şi o largă varietate de substanţe ajung din circulaţia maternă prin intermediul placentei în circulaţia fetală(1).
Termenul de placentă invazivă reflectă aderenţa excesivă a placentei la peretele uterin sau invadarea profundă a peretelui uterin de către aceasta. Incidenţa acestei patologii a crescut alarmant în ultimii 60 de ani. Morbiditatea şi mortalitatea maternă legate de această condiţie sunt considerabile. Placenta aderentă este citată ca fiind cea mai frecventă cauză de histerectomie de necesitate în cadrul operaţiei cezariene(2). Hemoragia incontrolabilă este complicaţia majoră ce face ca diagnosticul prenatal al placentei invazive să fie unul esenţial, iar managementul naşterii în cazul diagnosticului pozitiv să fie unul specific, atent planificat.
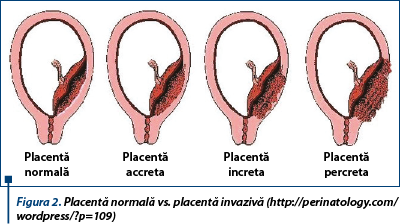
În funcţie de severitatea condiţionată de gradul de invazie, placenta invazivă poate fi clasificată în:
-
placenta acreta: definită de aderenţa excesivă a placentei la miometru, dar fără invadarea acestuia;
-
placenta increta: aderenţa excesivă a placentei prin invadarea miometrului uterin;
-
placenta percreta: invadarea întregii grosimi a pretelui uterin de către placentă, care poate să se extinda dincolo de seroasa uterină, ataşându-se organelor periuterine.
Incidenţă
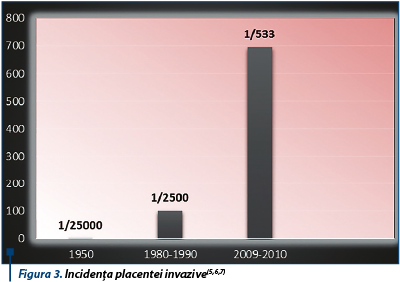
Frecvenţa placentei acreta domină, formele increta şi percreta fiind mai rare. Conform unui studiu ce a analizat 138 cazuri de placentă invazivă confirmată histologic(2,3), incidenţa placentei acreta este net superioară (79%) celor increta (14%) şi percreta (7%). Rata placentei invazive a crescut semnificativ în ultimii 60 de ani, unul din principalii factori fiind prevalenţa crescută a naşterilor prin operaţie cezariană(4). Dacă în anul 1950 incidenţa placentei invazive era raportată ca fiind 1/25000(5), în anul 1980 această patologie a avut o rată de prevalenţă de 1/2500(6). Date recente descriu o incidenţă de 1/533 pentru SUA(7) şi 1/588 pentru Canada(8). Luând în considerare continua tendinţă de creştere a incidenţei acestei patologii, este estimat faptul că până în anul 2020 SUA va avea o rată de incidenţă a operaţiilor cezariene de 56%, consecinţa fiind un plus de 4504 cazuri de placentă invazivă şi 130 de cazuri de deces matern anual(9).
Patogeneză şi factori de risc
Mecanismul etiopatogenic al placentei invazive nu este pe deplin cunoscut, o serie de ipoteze fiind însă propuse pe parcursul timpului(10). Decidua segmentului uterin superior compromisă primar, remodelarea vasculară maternă anormală, invazia trofoblastică excesivă sau o combinaţie a proceselor descrise sunt câteva din ipotezele propuse. Un studiu al lui Tantbirojn P şi colab.(11) în care s-au analizat 49 de cazuri de histerectomie peripartum, dintre care 38 de cazuri cu placentă invazivă confirmată, a concluzionat că patogeneza placentei invazive este multidimensională şi implică invazie trofoblastică crescută, dar incompletă, în context de absenţă deciduală. Factorul de risc dominant care favorizează dezvoltarea invazivă a placentei este uterul cicatriceal, numărul crescut al ceazarienelor segmento-trasnsversale în antecedente amplificând exponenţial riscul de apariţie a placentei invazive. Placenta previa la o pacientă cu operaţie cezariană în antecedente ridică suspiciunea diagnosticului de placentă invazivă, implicând un management prudent adecvat. Printre ceilalţi factori de risc se numără: vârsta maternă avansată, multiparitatea, chiuretaje uterine în antecedente, intervenţii chirurgicale pentru sindrom Asherman, embolizare sau miomectomie(12). Incidenţa placentei invazive este predominantă la sexul fetal feminin(13).

Aspecte clinice
Placenta invazivă este frecvent asimptomatică pe parcursul sarcinii. Depistarea ultrasonografică a acestei condiţii este obligatorie realizării unei pregătiri operatorii adecvate. Manifestarea clinică marcantă este hemoragia fudroaiantă, ameninţătoare de viaţă, ce survine de obicei în momentul naşterii şi este datorată imposibilităţii decolării placentei prin manevre uzuale. Transfuzia sanguină cu o medie de 10 unităţi de sânge şi produse sanguine este frecvent necesară, ligatura sau fistula ureterală, ruptura uterină spontană, patologia infecţioasă şi decesul matern marcând adesea evoluţia acesei anomalii de placentaţie. Conform studiilor, consecinţele placentei invazive asupra fătului pot fi naşterea prematură, restricţia de creştere intrauterină şi nu rareori decesul perinatal(14).
Imagistică
Pentru diagnosticarea placentei invazive, cele două metode care şi-au dovedit eficienţa sunt examenul ecografic şi rezonanţa magnetică nucleară (RMN). Prin ultrasonografie abdominală şi transvaginală se poate aprecia poziţia şi profunzimea invaziei uterine a placentei. În primul trimestru de sarcină, schiţa placentară jos situată sau în proximitatea cicatricei miometriale post-operaţie cezariană ridică suspiciunea de placentă invazivă şi necesită o monitorizare adecvată. Y.J. Chen şi colab. descriu diagnosticul placentei accreta, ecografic, la 9 săptămâni de gestaţie(15).
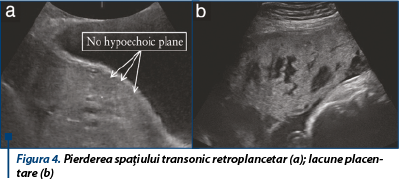
European Working Group on Abnormally Invasive Placenta este o societate non-profit compusă din 29 de ginecologi, obstetricieni, patologi, anestezişti şi cercetători din 11 ţări europene. Scopul acestei societăţi este dezvoltarea tehnicilor de diagnostic şi tratament al placentei invazive. Pentru facilitarea diagnosticului imagistic, această societate propune un consens al criteriilor ecografice, rezultat prin analiza a 23 de studii referitoare la diagnosticul antenatal ecografic al placentei invazive(16). În cadrul unui articol publicat în luna martie 2016 de către Ultrasound in Obsterics and Gynecology, grupul de lucru propune criterii ecografice standardizate, clare, pentru diagnosticarea placentei invazive, ilustrând în imagini ecografice fiecare dintre aceşti parametri(16):
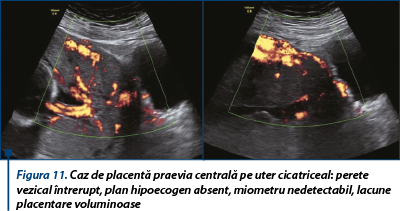
1. pierderea omogenităţii placentare, cu multiple spaţii transonice, lacune adiacente miometrului periplacentar;
2. pierderea sau iregularitatea spaţiului transonic retroplancetar;
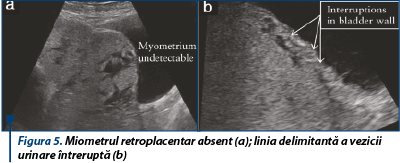
3. miometrul retroplacentar subţire <1 mm;
4. absenţa liniei delimitante a vezicii urinare;
5. masă exofitică ce depăşeşte seroasa uterină şi invadează vezica urinară;
6. protruzia placentei în spaţiul vezical.

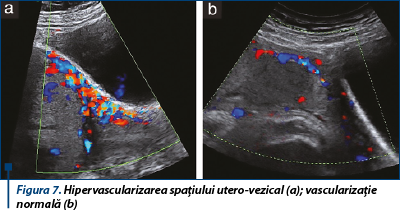
Doppler-ul color este foarte util diagnosticului pozitiv prenatal al placentei invazive, îmbunătăţind elementele sugestive decelate prin ultrasonografie convenţională 2D. Aspecte specifice relevate de utilizarea Dopller-ului color, power sau HD flow sunt lacunele placentare difuze sau intraparenchimtoase, lacurile vasculare cu flux turbulent, hipervascularizarea interfeţei seroasă - vezică urinară, complexe venoase proeminente subplacentare(17).
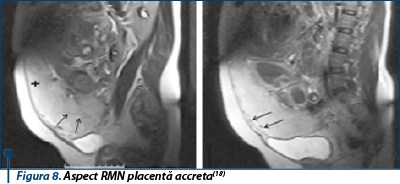
Explorarea RMN este mai eficientă în caz de placentă invazivă posterioară şi în aprecierea invazivităţii miometriale şi paramiometriale, inclusiv a organelor parauterine. Indicaţia RMN-ului este reprezentată de suspiciunea ecografică a diagnosticului de placentă invazivă, fără posibilitatea afirmării certe a acestuia exclusiv pe criterii ecografice. Acurateţea diagnostică a investigaţiei RMN este estimată fi aproape de 90%. Aspectele RMN sugestive, frecvent întâlnite, sunt spaţiul translucent intraplacentar şi discontinuitatea spaţiului perete vezical - seroasă uterină(18).
Atitudine terapeutică
Diagnosticul antenatal al placentei invazive este definitoriu evitării complicaţiilor grave anterior menţionate. Managementul pacientelor cu placentă invazivă este variabil, neexistând în prezent un protocol standardizat.
Suspiciunea prenatală a placentei invazive impune o serie de proceduri obligatorii: corectarea anemiei, în cazul prezenţei acesteia, administrarea de corticosteroizi între 24 şi 34 de săptămâni de gestaţie şi imunizarea pacientelor cu Rh negativ. Robert Resnik şi colab. recomandă administrarea de betametazonă şi practicarea intervenţiei la 34 de săptămâni de gestaţie, la 48 de ore după administrarea profilaxiei, riscurile prelungirii sarcinii dincolo de această limită fiind considerate nejustificate(18). Terminarea naşterii este recomandabil a fi realizată prin operaţie cezariană planificată, de către o echipă multidisciplinară cu experienţă şi aptitudini chirurgicale avansate, în condiţiile pregătirii disponibilităţii de sânge şi produse de sânge izogrup izoRh. Preoperator, este necesară obţinerea consimţământului informat al pacientei cu privire la riscurile care pot surveni şi pregătirea a cel puţin două căi venoase de calibru mediu/mare.
Trei modalităţi de abordare terapeutică şi-au demonstrat eficacitatea de-a lungul timpului:
1. Cateterizarea cu balon şi embolizarea arterială.
Scopul utilizării cateterelor cu balon este controlul hemoragiei post-partum. Părerile sunt împărţite între studii care au raportat hemoragii semnificativ reduse, necesitatea mai mică de transfuzie sanguină şi durata mai mică a intervenţiei chirurgicale şi studii care nu au raportat beneficii ale utilizării cateterismului(20). Cateterizarea necesită asepsie riguroasă locală. În fiecare arteră iliacă internă este inserat în porţiunea imediat distală de origine câte un balon de 8 mm diametru, fixat la piele. Inflaţia balonului se efectuează manual, cu presiune mică, pentru a evita leziunea arterei iliace interne, după extracţia fătului prin histerotomie fundică, următorul pas fiind decolarea placentei şi sutura patului placentar. Deflaţia balonului se efectuează după histerotomie.
În cadrul Departamentului de Imagistică Intervenţională al Spitalului Universitar de Urgenţă Bucureşti avem o amplă experienţă în managementul hemoragiilor post-partum prin atonie uterină, al sarcinilor ectopice, în special cele cu localizare cervicală, şi al sângerărilor din stadiile depăşite chirurgical ale cancerelor cervicale sau de corp uterin, prin tehnica embolizării arterelor uterine. Avantajele tehnicii sunt reprezentate de abordul minim invaziv, non-chirurgical şi conservator. Procedeul constă în cateterizarea supraselectivă a arterelor uterine şi embolizarea cu particule de PVA sau/şi Tachocomb, rezultând devascularizarea temporară sau permanentă a structurilor irigate de acestea şi hemostaza locală intravasculară.
2. Operaţie cezariană cu histerectomie
Această intervenţie este recomandată pentru a minimiza morbiditatea placentei invazive cu preţul sacrificării fertilităţii. Decizia histerectomiei este optim a se planifica preoperator, totuşi Carolyn F. Weiniger şi colab.(22), într-un studiu publicat în martie anul curent, afirmă faptul că 15% dintre pacientele suspectate ca având placentă invazivă, intraoperator au avut o bună decolare a placentei, fiind evitată histerectomia, astfel optând pentru decizia intraoperatorie a necesităţii histerectomiei.
Incizia recomandată este cea verticală, pubo-subombilicală, cu o atentă inspecţie a pelvisului şi organelor parauterine. Decizia locului practicării histerotomiei este corelată cu datele ecografice/de RMN privind poziţia placentei. Uterul este recomandabil a se inciza la distanţă de inserţia placentară, lăsând o porţiune de miometru indemn între incizie şi placentă, cea mai frecventă situaţie în cazul placentei praevia invazive pe uter cicatriceal fiind practicarea inciziei fundice a uterului. După ce fătul este extras şi cordonul ombilical secţionat, incizia este suturată complet în strat unic sau circumferenţial pentru a limita hemoragia, histerectomia practicându-se în timpul operator ulterior.
Tehnica ligaturii arterei hipogastrice reprezintă o altă alternativă descrisă, dar adesea evitată, fiind consumatoare de timp, operator-dependentă şi eficientă în doar 60% din cazuri în scăderea hemoragiei fără histerectomie(23).
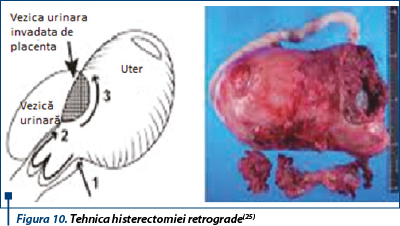
În cazul placentei increta cu invazia vezicii urinare, poate fi necesară cistectomia parţială(24). Shinya Matsuzaki şi colab.(25) descriu un caz de placentă percreta cu invadarea peretelui vezical, la care după extragerea fătului prin incizie mediană a peretelui abdominal şi incizie fundică uterină, autorii practică histerectomia retrogradă ce constă în deschiderea peretelui vaginal posterior, urmată de ligatura arterelor uterine şi a vaselor parametriale, cu plasarea preoperatorie a unui stent ureteral; deschiderea circumferenţiară a peretelui vaginal precede decolarea şi rezecţia peretelui anterior uterin şi a placentei din corpul uterin, histerectomia retrogradă fiind efectuată în timpul doi.
3. Managementul conservator al placentei invazive
Conservarea uterului poate fi luată în considerare atunci când pacienta insistă în vederea prezervării fertilităţii sau atunci când riscul histerectomiei depăşeşte riscul abandonării placentei in situ(26). Consilierea cu privire la riscurile managementului conservator vizează hemoragiile, infecţiile, histerectomia de necesitate şi recurenţa patologiei în sarcinile viitoare. După extragerea fătului şi ligatura cordonului la nivelul inserţiei sale placentare, placenta este lăsată in situ, după histerotomie aplicându-se numeroase metode de hemostază: medicaţie uterotonică, embolizarea arterelor uterine sau ligatura acestora, suturi de compresie. Numeroase studii descriu administrarea de metotrexat, fără a se dovedi însă eficienţa sa în aceste cazuri. Rezecţia histeroscopică a resturilor placentare a fost, de asemenea, descrisă ca fiind eficientă pentru tratamentul hemoragiilor şi durerilor pelviene survenite ulterior(27). Riscul ridicat de dezvoltare a sinechiilor uterine şi rata de recurenţă limitează această metodă.
Postoperatoriu
O urmărire atentă postoperatorie a pacientelor cu placentă invazivă este imperios necesară. Administrarea masivă de lichide poate avea drept complicaţie edemul pulmonar. Hemoragia incontrolabilă datorată placentaţiei invazive reprezintă o cauză majoră de coagulopatie intravasculară diseminată, detresă respiratorie a adultului, insuficienţă renală şi mortalitate maternă. Hemoragia postoperatorie este frecvent descrisă, caz în care embolizarea angiografică poate fi luată în considerare.

În cazul în care nu s-a practicat histerectomia în timpul operaţiei cezariene, este obligatorie consilierea pacientei cu privire la sarcinile următoare şi riscurile acestora.
Pe parcursul a doi ani, în cadrul Spitalului Universitar de Urgenţă Bucureşti, cu o rată anuală a naşterilor de 3700, au fost suspicionate pe criterii ecografice 135 de cazuri de placentă invazivă, 14 dintre aceste cazuri fiind intraoperator confirmate. Unul dintre aceste cazuri, cu placentă poziţionată pe peretele uterin posterior, a prezentat un diagnostic RMN fals pozitiv. O treime dintre cazurile de placentă invazivă au fost diagnosticate intraoperator, fără criterii ecografice de placentă invazivă descrise anterior, exceptând diagnosticul ecografic de placentă praevia. Într-un singur caz a fost nevoie de reintervenţie chirurgicală, iar rezultatul a constat în decesul matern.
Histerectomia de necesitate a fost practicată în 9 cazuri (64,2%), iar alte 5 cazuri au fost supuse embolizării arteriale, metodă aplicată cu succes.
Concluzii
Incidenţa placentei invazive este crescută în special din cauza creşterii ratei de naşteri prin operaţie cezariană. Mortalitatea şi morbiditatea maternă sunt reduse dacă naşterea are loc într-un centru specializat şi este realizată de o echipă multidisciplinară. Diagnosticul antenatal al placentei prin ultrasonografie, îndeosebi cu funcţie Doppler şi prin RMN, este definitoriu pentru planificarea managementului ulterior.
Divergenţele actuale de opinie privesc decizia preoperatorie a histerectomiei practicate în cadrul operaţiei cezariane sau amânarea deciziei până în momentul explorării intraoperatorii.
Deşi sunt descrise multiple tehnici de abordare a placentei invazive, nu s-a formulat până în prezent un protocol standardizat optim de management al acestor cazuri.
Bibliografie
1. Burton GJ, Hempstock J, Jauniaux E. Nutrition of the human fetus during the first trimester - a review. Placenta 2001; 22 Suppl A:S70.
2. Shellhaas CS, Gilbert S, Landon MB, Varner MW, Leveno KJ, Hauth JC, Spong CY, Caritis SN, Wapner RJ, Sorokin Y, Miodovnik M, O’Sullivan MJ, Sibai BM, Langer O, Gabbe SG; Eunice Kennedy Shriver National Institutes of Health and Human Development Maternal-Fetal Medicine Units Network. The frequency and complication rates of hysterectomy accompanying cesarean delivery. Obstet Gynecol 2009; 114: 224–229.
3. Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol 1997; 177:210.
4. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year analysis. Am J Obstet Gynecol 2005; 192:1458.
5. Miller DA, Chollet JA, Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol 1997; 177:210–214.
6. Committee on Obstetric Practice. ACOG committee opinion number 529: Placenta accreta. Obstet Gynecol 2012; 120: 207–211.
7. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year analysis. Am J Obstet Gynecol 2005; 192: 1458–1461.
8. Balayla J, Bondarenko HD. Placenta accreta and the risk of adverse maternal and neonatal outcomes. J Perinat Med 2013; 41: 141–149.
9. Eller AG, Bennett MA, Sharshiner M, Masheter C, Soisson AP, Dodson M, Silver RM Maternal morbidity in cases of placenta accreta managed by a multidisciplinary care team compared with standard obstetric care. Obstet Gynecol 2011; 117: 331–337.
10. Read JA, Cotton DB, Miller FC. Placenta accreta: changing clinical aspects and outcome. Obstet Gynecol 1980; 56:31.
11. Tantbirojn P, Crum CP, Parast MM. Pathophysiology of placenta creta: the role of decidua and extravillous trophoblast. Placenta 2008; 29:639.
12. Mehrabadi A, Hutcheon JA, Liu S, et al. Contribution of placenta accreta to the incidence of postpartum hemorrhage and severe postpartum hemorrhage. Obstet Gynecol 2015; 125:814.
13. S. Wu, M. Kocherginsky, J.U. Hibbard Abnormal placentation: twenty-year analysis Am J Obstet Gynecol, 192 (2005), pp. 1458–1461.
14. Khong TY, Healy DL, McCloud PI. Pregnancies complicated by abnormally adherent placenta and sex ratio at birth. BMJ 1991 Mar 16; 302 (6777); 625-6.
15. Y.J. Chen, P.H. Wang, W.M. Liu, C.R. Lai Placenta accreta diagnosed at 9 weeks’ gestation Ultrasound Obstet Gynecol, 19 (2002), pp. 620–622.
16. S. L. Collins, A Ashcroft, T. Braun et al. Proposal for standardized ultrasound descriptors of abnormally invasive placenta (AIP). Ultrasound in Obstetrics & Gynecology 47 (2016), pp. 271-275. http://onlinelibrary.wiley.com/doi/10.1002/uog.14952/full#uog14952-fig-0001
17. Chou MM, Ho ES, Lee YH. Prenatal diagnosis of placenta previa accreta by transabdominal color Doppler ultrasound. Ultrasound Obstet Gynecol 2000; 15:28.
18. Binoj Varghese, Navdeep Singh et al. Magnetic resonance imaging of placenta accreta. Abd Radiology 23 (2013) pp. 379-385.
19. Robert Resnik et al. Management of the morbidly adherent placenta (placenta accreta, increta, and percreta), http://www.uptodate.com/contents/management-of-the-morbidly-adherent-placenta-placenta-accreta-increta-and-percreta?source=search_result&search=invasive+placenta&selectedTitle=1~150#H1320723
20. Dubois J, Garel L, Grignon A, et al. Placenta percreta: balloon occlusion and embolization of the internal iliac arteries to reduce intraoperative blood losses. Am J Obstet Gynecol 1997; 176:723.
21. Dandu Ravi Varma et al. Management of type IV placenta previa by bilateral internaliliac artery balloon placement. Journal of Mahatma Gandhi Institute of Medical Sciences,20(2015;pp 170-172.
22. Carolyn F. Weiniger, Yehuda Ginosar et al. Suspected placenta accreta and cesarean hysterectomy: observational cohort utilizing an intraoperative decision strategy. European Journal of Obstetrics & Gynecology and Reproductive Biology 198 (2016); pp 56-61.
23. Clark SL, Phelan JP, Yeh SY, et al. Hypogastric artery ligation for obstetric hemorrhage. Obstet Gynecol 1985; 66:353.
24 Washecka R, Behling A. Urologic complications of placenta percreta invading the urinary bladder: a case report and review of the literature. Hawaii Med J 2002; 61:66.
25. Shinya Matsuzaki, Kiyoshi Yoshino, Keiichi Kumasawa, Noriko Satou, Kazuya Mimura, Takeshi Kanagawa, Yutaka Ueda & Tadashi Kimura.Placenta percreta managed by transverse uterine fundal incision with retrograde cesarean hysterectomy: a novel surgical approach. Clinical Case Reports 2014; 2(6): 260–264.
26. Fox KA, Shamshirsaz AA, Carusi D, et al. Conservative management of morbidly adherent placenta: expert review. Am J Obstet Gynecol 2015; 213:755.
27. Legendre G, Zoulovits FJ, Kinn J, et al. Conservative management of placenta accreta: hysteroscopic resection of retained tissues. J Minim Invasive Gynecol 2014; 21:910.

Evenimente organizate de MedicHub în luna IUNIE 2026
Florentina Ionescu
Luna iunie a acestui an vine cu mai multe evenimente marca MedicHub pe care nu trebuie să le ratați.
...
Subdiagnosticarea bolilor respiratorii cronice, o problemă majoră în România
Cristina Ghioca
În România sunt necesare investiții în prevenirea, screeningul și tratamentul bolilor respiratorii cronice, au atras atenția participanții la o masă rotundă privind managementul bolilor respiratorii.
...
SUUB demarează un proiect în parteneriat cu Politehnica
Florentina Ionescu
Scopul concret al proiectului este de a introduce pe piața internă și europeană un dispozitiv medical portabil, inteligent, denumit INDOVIEWER.
...
Evenimente organizate de MedicHub în luna IUNIE 2026
Florentina Ionescu
Luna iunie a acestui an vine cu mai multe evenimente marca MedicHub pe care nu trebuie să le ratați.
...
Subdiagnosticarea bolilor respiratorii cronice, o problemă majoră în România
Cristina Ghioca
În România sunt necesare investiții în prevenirea, screeningul și tratamentul bolilor respiratorii cronice, au atras atenția participanții la o masă rotundă privind managementul bolilor respiratorii.
...
SUUB demarează un proiect în parteneriat cu Politehnica
Florentina Ionescu
Scopul concret al proiectului este de a introduce pe piața internă și europeană un dispozitiv medical portabil, inteligent, denumit INDOVIEWER.
...