Calitatea vieţii la pacientele cu endometrioză şi rezecţie colorectală laparoscopică
Quality of life in patients with deep endometriosis and laparoscopic colorectal resection
Abstract
Objective. The aim of this paper is to evaluate the effectiveness of laparoscopic colorectal resection in cases of deep endometriosis, as well as the impact on the quality of life, on gynecological and digestive symptoms. Materials and method. Following the preoperative evaluation (MRI, transvaginal ultrasound, endorectal ultrasound, hydro-colon CT), 42 cases with deep endometriosis were included in the studied group. All patients included in the study completed a questionnaire on preoperative endometriosis symptoms and quality of life (SF-36 Questionnaire). The status and quality of life were assessed. Gynecological and digestive symptoms, as well as the rate of perioperative complications were also assessed. Laparoscopic surgeries were performed by the same operating team (E.B., C.C.B., R.M., A.I., L.R.). Results. The average age of the patients was 34 years old. The conversion rate to laparotomy was zero. Following surgery, there was a significant improvement regarding dysmenorrhea, dyspareunia, chronic pelvic pain, defecation pain, and lower abdominal pain. In cases with deep endometriosis and colorectal resection, an improvement in the score for the quality of life, assessed by the SF-36 Questionnaire, was observed. One patient (2.38%) refused the colorectal resection for objective reasons. The rate of perioperative complications was 4.76%, including an inadvertent cystotomy (2.38%) and a reintervention (2.38%) at five days postoperatively – protective ileostomy. The rate of hemoperitoneum, rectovaginal fistula, uroperitoneum and pelvic abscess was zero. Conclusions. Laparoscopic segmental colorectal resection for endometriosis significantly improves the quality of life and the gynecological and digestive symptoms. However, women should be informed about the risk of complications, including rectovaginal fistula. The need to adhere to a guideline on the therapeutic conduct in cases of deep endometriosis and the standardization of treatment allow to obtain satisfactory results in terms of improving the quality of life in patients with colorectal resection. Preoperative investigations allow the planning of surgery and the formation of a multidisciplinary team for the correct management and the complete excision of endometriotic lesions.Keywords
minimally invasive surgerylaparoscopydeep endometriosissuperficial endometriosisrectosigmoid resectionmechanical end-to-end anastomosisRezumat
Obiectiv. Scopul acestei lucrări este de a evalua eficacitatea rezecţiei colorectale laparoscopice în cazurile de endometrioză profundă, precum şi impactul asupra calităţii vieţii şi asupra simptomatologiei ginecologice şi digestive. Materiale şi metodă. În urma evaluării preoperatorii (RMN, ecografie transvaginală, ecografie endorectală, hidro-colono-CT), în lotul studiat au fost incluse 42 de paciente cu endometrioză profundă. Toate pacientele incluse în studiu au completat un chestionar privind simptomele preoperatorii ale endometriozei şi calitatea vieţii (chestionarul SF-36). Au fost evaluate statusul şi calitatea vieţii. De asemenea, au fost evaluate simptomele ginecologice şi digestive, precum şi rata de complicaţii perioperatorii. Intervenţiile chirurgicale laparoscopice au fost efectuate de aceeaşi echipă operatorie (E.B., C.C.B., R.M., A.I., L.R.). Rezultate. Vârsta medie a pacientelor a fost de 34 de ani. Rata de conversie la laparotomie a fost nulă. În urma intervenţiei chirurgicale s-a observat o ameliorare semnificativă a dismenoreei, dispareuniei, a durerilor pelviene cronice, a durerilor la defecaţie şi a durerilor în etajul abdominal inferior. În cazurile cu endometrioză profundă şi rezecţie colorectală, s-a observat o îmbunătăţire a scorului pentru calitatea vieţii, evaluată prin chestionarul SF-36. O pacientă (2,38%) a refuzat rezecţia colorectală, din motive obiective. Rata de complicaţii perioperatorii a fost de 4,76%, incluzând o cistotomie inadvertentă (2,38%) şi o reintervenţie (2,38%) la cinci zile postoperatoriu – ileostomă de protecţie. Rata de hemoperitoneu, fistulă rectovaginală, uroperitoneu şi de abces pelvian a fost nulă. Concluzii. Rezecţia colorectală segmentară laparoscopică pentru endometrioză îmbunătăţeşte semnificativ calitatea vieţii şi simptomele ginecologice şi digestive. Cu toate acestea, femeile trebuie să fie informate cu privire la riscul unor complicaţii, inclusiv fistula rectovaginală. Necesitatea aderării la un ghid privind conduita terapeutică în cazurile de endometrioză profundă şi standardizarea tratamentului permit obţinerea unor rezultate satisfăcătoare în ceea ce priveşte ameliorarea calităţii vieţii la pacientele cu rezecţie colorectală. Investigaţiile preoperatorii permit planificarea intervenţiei chirurgicale şi formarea unei echipe multidisciplinare, pentru managementul corect şi excizia completă a leziunilor endometriozice.Cuvinte Cheie
chirurgie minim invazivălaparoscopieendometrioză profundăendometrioză superficialărezecţie rectosigmoidianăanastomoză termino-terminală mecanicăIntroduction
Deep infiltrating endometriosis of the bowel represents a major challenge for the gynecologists, general surgeons and patients. The incidence regarding deep infiltrating endometriosis affecting the bowel is estimated at 5-12% of the patients with deep endometriosis(1). Endometriosis has a high impact on the life of the patient, leading to chronic non-menstrual pelvic pain, dysmenorrhea, dyspareunia and infertility. Deep infiltrating endometriosis affecting the intestinal tract generates digestive symptoms, such as diarrhea, constipation, painful defecation, rectal bleeding or even occlusion(2).
Deep endometriosis is defined as the presence of endometrial tissue infiltrating more than 5 mm of the peritoneum. Deep endometriosis of the bowel represents the endometriosis that affects the muscular layer(3,4). The endometriosis can spread from the small bowel to the anus, but the most frequent sites are the rectum and sigmoid colon (74%), cecum and appendix(5).
Once the diagnosis of bowel endometriosis has been made, the management plan must be established and the colorectal resection procedure – with its advantages and disadvantages – must be discussed with the patient. Once the surgery is established, a complete resection of all endometriotic lesions must be performed(6). There has to be a specialized multidisciplinary team in charge of these cases, in order to reduce the negative outcomes while maintaining good results(7).
Alike any other surgical procedure, the surgical treatment of deep infiltrating endometriosis of the bowel has also some downsides besides the expected favourable outcome. Postprocedural complications depend on different surgical approaches, and the number of complications can sum up when more than one technique is performed. Both major and minor surgical complications have been reported after the surgical excision of deep endometriosis. The complications that need to be mentioned are: pelvic abscess, cutaneous abscesses, peritonitis, stenosis of colorectal anastomosis, anastomotic leakage(8), rectovaginal fistula(9-11), haemorrhage(12), laparoconversion(13), bladder atony and bowel dysfunction(14). However, some studies suggested that the risk of unfavourable outcomes is higher when segmental colorectal resection is performed, but we also have to reckon with the patient’s overall health condition(15).
The aim of this paper is to present the direct observation of the authors and to evaluate the effectiveness of laparoscopic colorectal resection in cases of deep endometriosis, as well as the impact on life’s quality, gynecological symptoms and digestive symptoms.
Materials and method
We conducted a prospective study, from January 2019 to December 2019, in the Department of Obstetrics and Gynecology of the Monza Hospital, Bucharest, and the “Prof. Dr. Panait Sîrbu” Clinical Hospital of Obstetrics and Gynecology. We enrolled patients with deep infiltrating endometriosis symptoms. Following the preoperative evaluation (magnetic resonance imaging [MRI], transvaginal ultrasound, endorectal ultrasound, hydro-colo computed tomography), forty-two cases with deep endometriosis were included in the studied group. From this group, we choose the patients with bowel endometriosis, and the study will focus on them.
All patients included in this study completed a questionnaire regarding preoperative endometriosis symptoms and the quality of life (SF-36 Questionnaire) and six-month postoperative symptoms, in order to evaluate the impact of symptoms on life before and after the colorectal resection. All patients gave their informed consent. The purpose of the questionnaire is twofold: to provide a complete clinical picture of the symptoms, and to objectify the improvement of the quality of life. The questionnaire consists of multiple variables that quantify various dimensions of health, that can be associated into two measures, the physical and mental scores. Patients also filled in data regarding the presence of dysmenorrhea, dyspareunia and of chronic non-menstrual pelvic pain. Status and quality of life were assessed. Quality of life assessment in patients with deep endometriosis is an integral part of both preoperative and postoperative assessment, in order to objectify the benefit of surgery. Gynecological and digestive symptoms, as well as the rate of perioperative complications were also assessed.
The operative strategy was discussed in the multidisciplinary team which consisted of gynecology specialists and general surgeons. The management plan was also discussed with the patient. The 28 procedures were performed as a segmental laparoscopic bowel resection with end-to-end anastomosis. All of the visible endometriosis was excised, including infiltrating nodules of the sacrouterine ligaments, parametrial nodules and peritoneum lesions. In those cases with ovarian endometriomas, unilateral or bilateral laparoscopic cystectomy was performed. For the transection of the rectosigmoid below the endometriotic lesion a linear stapler was used, after which the bowel was exteriorized through an extension of the umbilical incision. The end-to-end anastomosis was completed using a circular stapler (33 mm). Laparoscopic surgeries were performed by the same operating team (E.B., C.C.B., R.M., A.I., L.R.).
To assess the comparisons between preoperative and postoperative scores, the Student t test and Pearson correlation were performed for continuous data. For all comparisons, a p<0.05 was considered to define statistical significance. All data were analyzed in SPSS 23.0.
Results
Twenty-eight patients (67%) received laparoscopic segmental rectosigmoid resection with mechanical end-to-end anastomosis. Thirteen patients (31%) with deep endometriosis benefited from laparoscopic excision of deep endometriosis nodules and one (2%) patient with bowel endometriosis refused the rectosigmoid resection – Figure 1. The histopathologic exam confirmed in all cases that the bowel nodules were endometriotic.
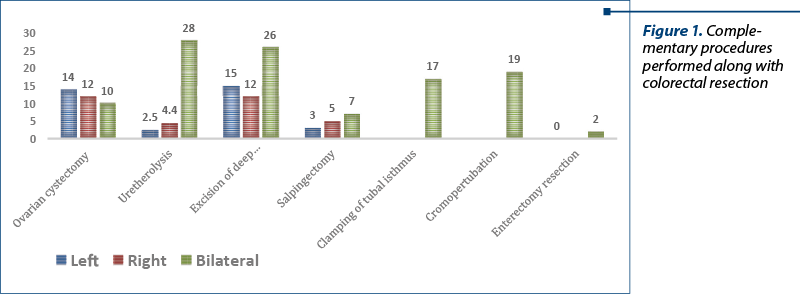
From now on, we will focus on the 28 patients who underwent laparoscopic segmental rectosigmoid resection with mechanical end-to-end anastomosis. In Figure 2, we illustrate the complementary procedures that were performed beside colorectal resection.
The mean age of the 28 patients included in the study was 34.1 years old. The demographic characteristics of the patients is presented in Table 1.
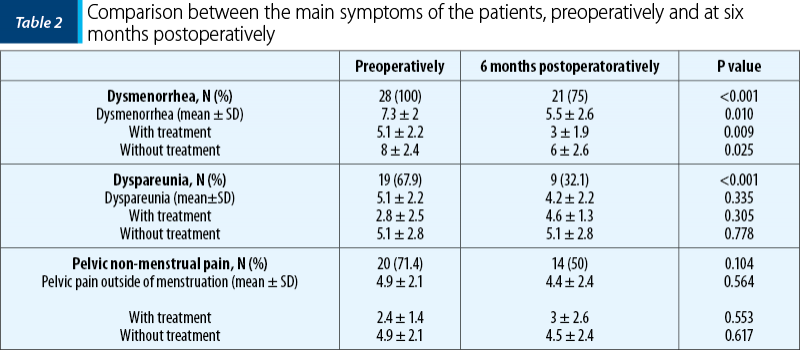
All patients presented preoperatively with dysmenorrhea (100%) and 19 (67.9%) with dyspareunia. Regarding the pelvic non-menstrual pain, 20 patients (71.4%) presented the aforementioned symptom. Six months after surgery, at the follow-up, the number of patients who presented with the symptoms described before was lower compared to preoperative numbers. Following surgery, there was a significant improvement (p<0.05) in dysmenorrhea, dyspareunia and chronic non-menstrual pelvic pain, as it can be observed in Table 2.
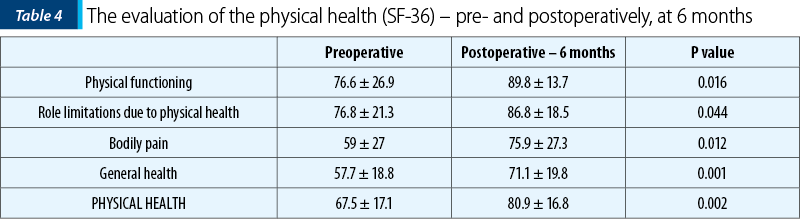
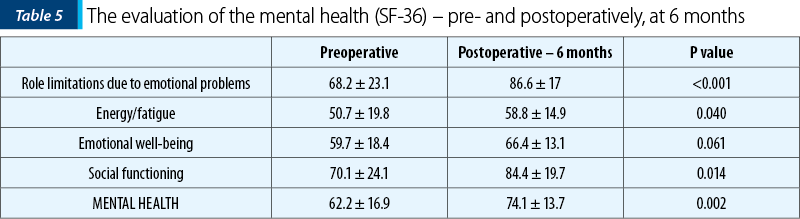
The quality of life, evaluated with SF-36 Questionnaire, is summarized in two elements: physical health and mental health, each with four aspects. Dysmenorrhea and dyspareunia affect the quality of life, as we notice from Table 3.
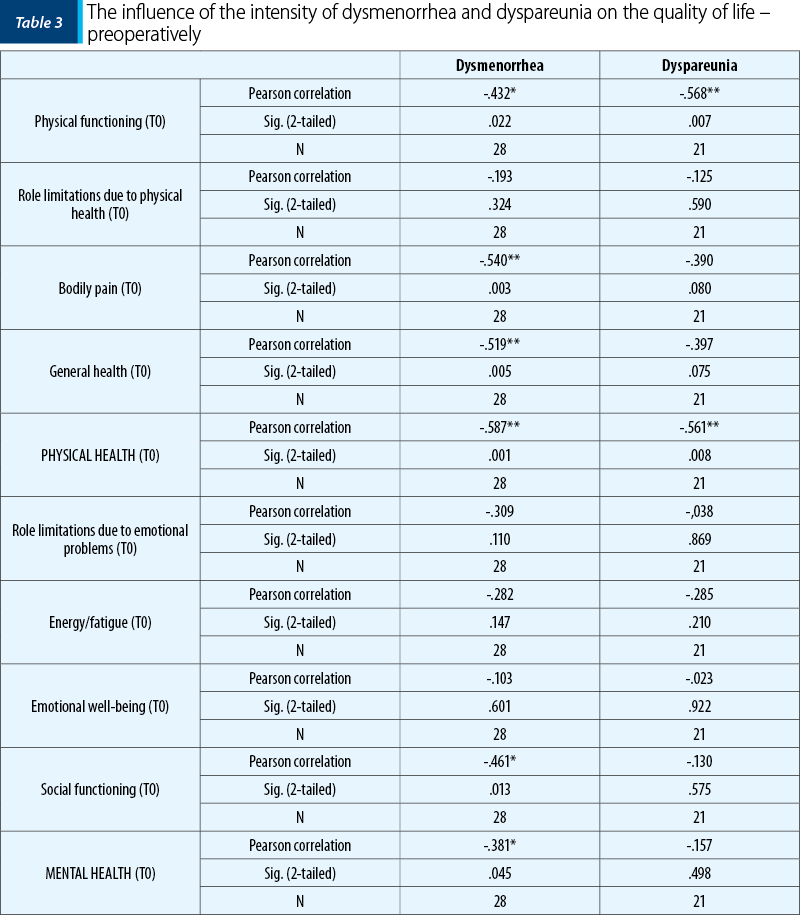
We found out that, preoperatively, there is an inverse statistic correlation between the intensity of both dysmenorrhea and dyspareunia and some variables regarding life’s quality. This statistically negative correlation proves that, the higher the intensity of dysmenorrhea, the lower the physical functioning, the bodily pain, the general health, the social functioning, the physical health and the mental health. Also, the higher the intensity of dyspareunia, the lower the level of physical functioning and physical health.
As we can notice in Table 4 and Table 5, a significant improvement was observed in all eight aspects and both elements (p<0.05) of the quality of life after the bowel resection.
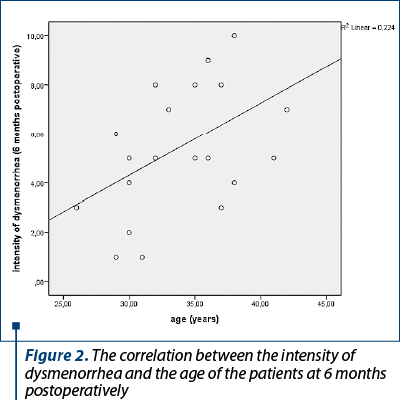
Patients’ age correlated statistically significantly with the intensity of postoperative dysmenorrhea at 6 months (p=0.030). The Visual Analogue Scale was used in order to assess the intensity of dysmenorrhea. The older the patients, the higher the intensity of dysmenorrhea (Figure 2).
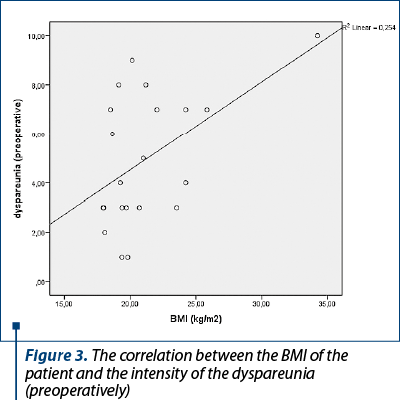
The Body Mass Index (BMI) of the patients had a positive statistical correlation with the intensity of the preoperative dyspareunia (p=0.020). The higher the BMI, the higher the intensity of the preoperative dyspareunia (Figure 3).
The rate of perioperative complications was 4.76%, including an inadvertent cystotomy (2.38%) and a reintervention (2.38%) at five days postoperatively –protective ileostomy. Two patients (4.76%) benefited from double resection – rectosigmoid segmental resection and segmented enterectomy with manual anastomosis. The protective ileostoma was due to the enteral anastomosis (short distance from the ileocecal valve). The rate of hemoperitoneum, rectovaginal fistula, uroperitoneum and pelvic abscess was zero.
Discussion
The present study brings preoperative and postoperative information on pelvic pain and quality of life in a group of women who underwent rectosigmoid resection for deep infiltrating endometriosis. Our study shows that laparoscopic colorectal resection has a statistically significant positive effect on pain symptoms and life’s quality in these patients. For all elements of the mental and physical health, a highly significant improvement was observed. All of the comparisons presented had highly significant p values, minimizing the risk of multiple comparison problems.
Even though large studies regarding deep infiltrating endometriosis surgeries with colorectal segmental resection are needed, several studies, retrospective, with limited number of patients, were published and revealed similar findings with the ones of our study. Bailey et al. reported that 86% of the patients who underwent colorectal resection had symptoms improvement at 6 months postoperatively. In a study of 50 patients, Kavallaris et al. noted that 72% of the women, at 32 months postlaparoscopic segmental bowel resection, were symptom-free or nearly symptom-free. An improvement regarding dysmenorrhea and dyspareunia was noticed by Thomassin et al. in a study in which 27 patients were followed-up after bowel resection(16-18).
Some authors believe that segmental rectosigmoid resection should be avoided due to short- and long-term complications. Our rate of postoperative complications was low and we didn’t report any fistula or leakage, despite large studies, like the one published in France, which reported a rate of these complications at 4.7% after laparoscopic segmental resection of bowel endometriosis(19).
Conclusions
Bowel involvement with endometriosis is a new frontier for the gynecologists, general surgeons and patients. We have shown that laparoscopic segmental colorectal resection for endometriosis significantly improves gynecological symptoms – dysmenorrhea, dyspareunia and non-menstrual pelvic pain. The aforementioned improvements had a positive effect on life’s quality for these patients. Rectosigmoid resection is a feasible and safe technique for treating bowel endometriosis.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Coronado C, et al. Surgical treatment of symptomatic colorectal endometriosis. Fertil Steril. 1990;53(3):411–6.
-
Roman H, et al. Surgical management of deep infiltrating endometriosis of the rectum: Pleading for a symptom-guided approach. Hum Reprod. 2011;26(2):274–81.
-
Koninckx PR, Martin DC. Deep endometriosis: A consequence of infiltration or retraction or possibly adenomyosis externa? Fertil Steril. 1992;58(5):924–8.
-
Bazot M, Daraï E. Diagnosis of deep endometriosis: clinical examination, ultrasonography, magnetic resonance imaging, and other techniques. Fertil Steril. 2017;108(6):886–94.
-
Chamié LP, et al. Atypical sites of deeply infiltrative endometriosis: Clinical characteristics and imaging findings. Radiographics. 2018;38(1):309–28.
-
Carmona F, et al. Does the learning curve of conservative laparoscopic surgery in women with rectovaginal endometriosis impair the recurrence rate? Fertil Steril. 2009;92(3):868–75.
-
Tuech JJ, Roman H. Worrying about postoperative functional outcomes in young women with colorectal endometriosis: That’s it! Dis Colon Rectum. 2018;61(2):149–50.
-
Balla A, et al. Outcomes after rectosigmoid resection for endometriosis: a systematic literature review. Int J Colorectal Dis. 2018;33(7):835–47.
-
Duepree HJ, et al. Laparoscopic resection of deep pelvic endometriosis with rectosigmoid involvement. J Am Coll Surg. 2002;7515(02):754–8.
-
Keckstein J, Wiesinger H. Deep endometriosis, including intestinal involvement – the interdisciplinary approach. Minim Invasive Ther Allied Technol. 2005;14(3):160–6.
-
Ruffo G, Scopelliti EF. Laparoscopic colorectal resection for deep infiltrating endometriosis: analysis of 436 cases. Surg Endosc. 2010;24(1):63–7.
-
Darai E, et al. Laparoscopic segmental colorectal resection for endometriosis: limits and complications. Surg Endosc. 2007;21(9):1572–7.
-
Dubernard G, et al. Quality of life after laparoscopic colorectal resection for endometriosis. Hum Reprod. 2006;21(5):1243–7.
-
Milone M, et al. Colorectal resection in deep pelvic endometriosis: Surgical technique and post-operative complications. World J Gastroenterol. 2015;21(47):13345–51.
-
Abo C, et al. Postoperative complications after bowel endometriosis surgery by shaving, disc excision, or segmental resection: a three-arm comparative analysis of 364 consecutive cases. Fertil Steril. 2018;109(1):172-178.e1.
-
Kavallaris A, et al. Histopathological extent of rectal invasion by rectovaginal endometriosis. Hum Reprod. 2003;18(6):1323-7.
-
Bailey HR, Ott MT, Hartendorp P. Aggressive surgical management for advanced colorectal endometriosis. Dis Colon Rectum. 1994;37(8):747–53.
-
Thomassin I, et al. Symptoms before and after surgical removal of colorectal endometriosis that are assessed by magnetic resonance imaging and rectal endoscopic sonography. Am J Obstet Gynecol. 2004;190(5):1264–71.
-
Roman H, FRIENDS group (French coloRectal Infiltrating ENDometriosis Study group). A national snapshot of the surgical management of deep infiltrating endometriosis of the rectum and colon in France in 2015: A multicenter series of 1135 cases. J Gynecol Obstet Hum Reprod. 2017;46(2):159-65.

May-September 2021 Calendar
May-September 2021 Calendar...
Actualităţi în investigarea prenatală a fătului folosind RMN-ul fetal
Erick George Neştianu, Cristina Brădeanu-Guramba, Radu Vlădăreanu, Simona Vlădăreanu
Rezonanţa magnetică nucleară (RMN) fetală reprezintă o unealtă modernă, care vine în ajutorul stabilirii diagnosticului în sarcinile la risc. Acesta reprezintă o examinare complementară ecografiei, demonstrându-şi a...
IRM – avantaje şi limite în diagnosticul şi tratamentul endometriozei
Cristina Vladu, Andreea Boiangiu, Elvira Brătilă, Radu Vlădăreanu
Endometrioza este o boală ginecologică multifocală comună, care se manifestă în timpul anilor de reproducere, cauzând adesea dureri pelviene cronice şi infertilitate. Poate apărea ca noduli şi aderenţe fibrotice periton...
IRM – avantaje şi limite în diagnosticul şi tratamentul endometriozei
Cristina Vladu, Andreea Boiangiu, Elvira Brătilă, Radu Vlădăreanu
Endometrioza este o boală ginecologică multifocală comună, care se manifestă în timpul anilor de reproducere, cauzând adesea dureri pelviene cronice şi infertilitate. Poate apărea ca noduli şi aderenţe fibrotice periton...
Imagistica şi maparea chirurgicală în endometrioză
Cristina Vladu, Andreea Boiangiu, Elvira Brătilă, Radu Vlădăreanu
Endometrioza este o boală cronică estrogen-dependentă, cu potenţial inflamator, caracterizată prin prezenţa ţesutului ectopic endometrial în afara uterului, cu caracter polimorf şi multifocal, la aceeaşi pacientă pu...