Correlation between vitamin D deficiency and fibrocystic mastopathy
Corelaţia dintre deficitul de vitamina D şi mastopatia fibrochistică
Abstract
Fibrocystic dystrophy is one of the most frequent and common non-neoplastic pathologies whose symptomatology is represented by the appearance of painful nodules in the breast. Fibrocystic lesions have several etiological factors, the most important being considered the hormonal imbalance between estrogen and progesterone, manifested by excess estrogen that causes proliferations at the connective tissue level (fibrosis). The diagnosis of this pathology is based on symptoms and with the help of breast ultrasound, which can also be used in the puncture and drainage of large cysts. The treatment of fibrocystic breast disease is a medical one, by administering combined oral contraceptives, having a success rate of 70-90%. Breast ultrasound is an important technique for evaluating breast anatomy in benign and malignant pathologies. Fibrocystic mastopathy is most often associated with dense breasts with well-developed breast tissue. Epidemiological studies suggest that the level of vitamin D (25-hydroxycholecalciferol) below 20 ng/mL is associated with an increased risk of breast, colon and prostate cancer. In young people, vitamin D deficiency is associated with benign pathology (mammary cysts, fibroadenoma). This article presents a study in which 50 women, aged between 30 and 50 years old, were included, for a period of three years, all of them being diagnosed by ultrasound with fibrocystic mastopathy and all presenting vitamin D deficiency (below 20 ng/mL 25-hydroxyvitamin D) at the time of the examination.Keywords
vitamin Dfibrocystic mastopathybreast ultrasoundRezumat
Distrofia fibrochistică este una dintre cele mai frecvente şi comune patologii non-neoplazice, a cărei simptomatologie este reprezentată de apariţia unor noduli dureroşi la nivelul sânului. Leziunile fibrochistice au ca etiologie mai mulţi factori, cel mai important fiind considerat dezechilibrul hormonal dintre estrogen şi progesteron, manifestat prin exces estrogenic, care determină proliferări la nivelul ţesutului conjunctiv (fibroză). Diagnosticul acestei patologii se face pe baza simptomatologiei şi cu ajutorul ecografiei mamare, care poate fi utilizată şi în puncţia şi drenarea chisturilor mari. Tratamentul bolii fibrochistice mamare este medicamentos, prin administrare de contraceptive orale combinate, cu o rată de succes de 70-90%. Ecografia mamară reprezină o tehnică importantă pentru evaluarea anatomiei sânului, a patologiei benigne şi maligne. Mastopatia fibrochistică este asociată de cele mai multe ori cu sânul dens, cu ţesut mamar bine dezvoltat. Studiile epidemiologice sugerează că nivelul de vitamină D (25-hidroxicolecalciferol) sub 20 ng/mLeste asociat cu un risc crescut de cancere de sân, colon sau prostată, iar la persoanele tinere deficitul de vitamina D se asociază cu patologia benignă (chisturi mamare sau fibroadenom). Acest articol prezintă un studiu în care au fost incluse 50 de femei, pe durata a trei ani, cu vârste cuprinse între 30 şi 50 de ani, toate fiind diagnosticate ecografic cu mastopatie fibrochistică şi toate, la momentul examinării, prezentând deficienţă de vitamina D (sub 20 ng/mL 25-hidroxivitamină D).
Cuvinte Cheie
vitamina Dmastopatie fibrochisticăecografie mamarăIntroduction
Fibrocystic dystrophy is one of the most frequent and common non-neoplastic pathologies whose symptomatology is represented by the appearance of painful nodules in the breast. Fibrocystic lesions have as their etiology several factors, the most important being considered the hormonal imbalance between estrogen and progesterone, manifested by excess estrogen that causes proliferations at the connective tissue level (fibrosis)(1).
The most affected age category is between 20 and 40 years old, with the maximum prevalence before menopause(2). Most of the patients present menometrorrhagia, are nulliparous, with a history of spontaneous abortions in the past, early menarche and late menopause(3). The main symptoms of fibrocystic mastopathy are mastodynia and increased breast sensitivity which can be associated with dysmenorrhea, menometrorrhagia and frequently ovarian cysts (40-60%). The diagnosis of this pathology is based on symptoms and with the help of breast ultrasound, which can also be used in the puncture and drainage of large cysts. The treatment of fibrocystic breast disease is medical, by administering combined oral contraceptives, with a success rate of 70-90%(4).
Vitamin D was identified by Edward Mellanby, as a fat-soluble substance with antirachitic properties, classically associated with its physiological role of regulating calcium and phosphate in bone metabolism. People can get vitamin D from two main sources: from food and from exposure to the sun. Few foods contain vitamin D in significant amounts, among them being fish, eggs and mushrooms. However, the majority (90% to 95%) of the vitamin D requirement is produced by the skin when exposed to sunlight (ultraviolet B radiation)(5). The biologically active form of vitamin D – 1a,25-dihydroxyvitamin D3 or 1a,25(OH)2D3 – is synthesized in the kidneys by the mitochondrial enzyme CYP27B1(6).
Vitamin D is a steroid hormone that exerts most of its biological activities by binding to a specific and high-affinity receptor (vitamin D receptor; VDR). VDR belongs to the superfamily of nuclear receptors for steroid hormones and regulates gene expression by acting as a transcription factor(7). Vitamin D can also induce VDR-independent effects; the anti-proliferative effects of vitamin D in MCF-7 cells are not solely dependent on the presence of VDR(8).
It has been shown that vitamin D plays an important role in the development and function of the mammary gland, the VDR receptor being also present in normal breast tissue, through immunohistochemical tests(9). The main enzymes involved in the metabolism of vitamin D in the normal breast are CYP27B1 and CYP24A1(10), and an imbalance of those can cause the appearance of benign pathology or neoplasia.
Regarding the representation of differences in the expression of vitamin D receptor, CYP27B1 and CYP24A1 during breast carcinogenesis, vitamin D receptor and CYP27B1 expression decreases with breast carcinogenesis, while CYP24A1 expression is increased (the level of brown coloring represents the intensity of gene expression)(11) – Figure 1.

In benign breast pathology, the aforementioned three proteins (VDR, CYP27B1 and CYP24A1) are in decreased amount compared to normal breast.
Epidemiological studies suggest that the level of vitamin D (25-hydroxycholecalciferol) below 20 ng/mL is associated with an increased risk of breast, colon and prostate cancer(12). In young people, vitamin D deficiency is associated with benign pathology (mammary cysts, fibroadenoma)(13).
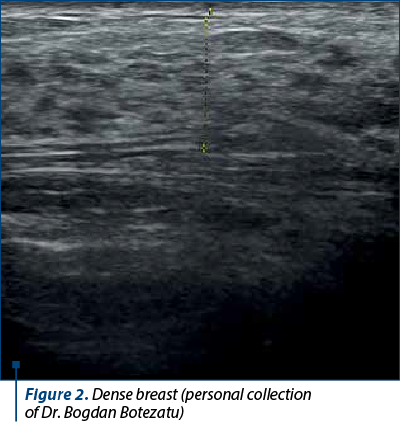
Breast ultrasound is an important technique for evaluating breast anatomy, benign and malignant pathology. Fibrocystic mastopathy is most often associated with dense breasts with well-developed breast tissue (Figures 2 and 3).

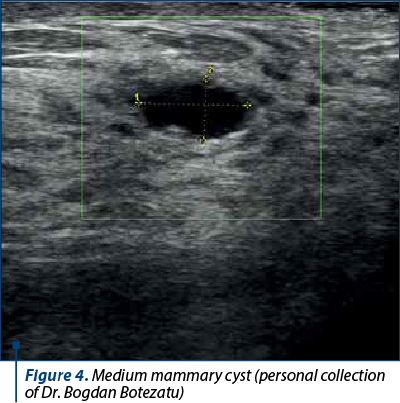
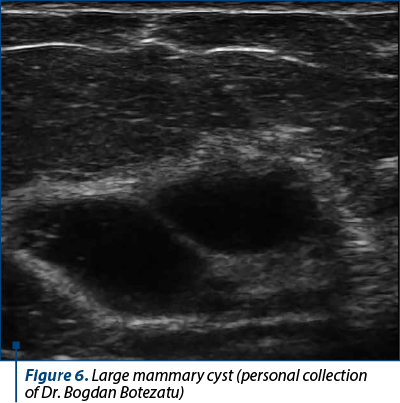
Fibrocystic mastopathy is highlighted sonographically by multiple anechoic images, well delimited with posterior acoustic accentuation, usually of medium or small size, present in both breasts; the anatomical structure of the breast is preserved and there is no accentuation of the vascularization (Figures 4, 5 and 6).

Materials and method
The study included 50 women, for a period of three years, aged between 30 and 50 years old, all of them being diagnosed by ultrasound with fibrocystic mastopathy and all presenting vitamin D deficiency (below 20 ng/mL of 25-hydroxyvitamin D)(14) at the time of the examination.
After the administration of vitamin D3 (2000 UI) for at least six months and the correction of the vitamin deficiency (above 30 ng/ml of 25-hydroxyvitamin D), the bilateral breast ultrasound was performed again.
At the time of the ultrasound examination, all the cystic images in the four quadrants of the breast were described, measured and numbered.
Results
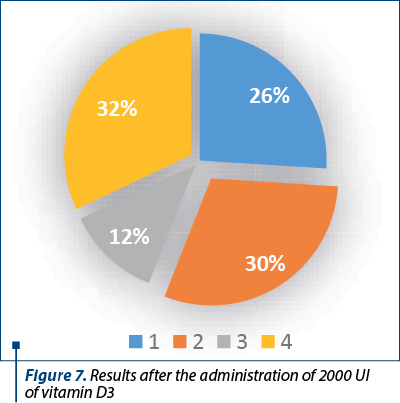
Thirteen patients (26%) presented an important reduction in the number of breast cystic formations, by more than 50% than in the previous examination, 15 patients (30%) presented a moderate reduction (between 25% and 50% than the previous examination), and six patients (12%) presented a slight decrease, between 10% and 20% compared to the previous examination. Sixteen patients (32%) did not show significant changes, or the number of cystic formations increased.
Conclusions
1. Fifty-six percent of the patients showed a statistically significant reduction in the number of breast cystic formations, this revealing that a correction of vitamin D deficiency has beneficial effects on patients (Figure 7).
2. The sizes of the cysts decreased significantly in the patients who responded to the treatment and even in four patients in the non-responsive group.
3. The fact that 44% of patients were nonresponsive or had a poor response shows that other factors, besides vitamin D deficiency, are involved in fibrocystic breast dystrophy.
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Norwood SL. Fibrocystic breast disease. An update and review. J Obstet Gynecol Neonatal Nurs. 1990:19(2):116-21.
-
Stachs A, Stubert J, Reimer T, Hartmann S. Benign breast disease in women. Dtsch Arztebl Int. 2019;116(33-34):565-74.
-
Arulkumaran S. Essentials of gynecology. LWW Wolters Kluwer. 2005;698.
-
Malherbe K, Khan M, Fatima S. Fibrocystic Breast Disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 8, 2023.
-
Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80(6 Suppl):1678S-88S.
-
Haussler MR, Whitfield GK, Haussler CA, Hsieh JC, Thompson PD, Selznick SH, Dominguez CE, Jurutka PW. The nuclear vitamin D receptor: biological and molecular regulatory properties revealed. J Bone Miner Res. 1998;13(3):325-49.
-
Evans RM. The steroid and thyroid hormone receptor superfamily. Science. 1988;240:889-89.
-
Costa JL, Eijk PP, van de Wiel MA, ten Berge D, Schmitt F, Narvaez CJ, Welsh J, Ylstra B. Anti-proliferative action of vitamin D in MCF7 is still active after siRNA-VDR knock-down. BMC Genomics. 2009;10:499.
-
Berger U, Wilson P, McClelland RA, Colston K, Haussler MR, Pike JW, Coombes RC. Immunocytochemical detection of 1,25-dihydroxyvitamin D receptors in normal human tissues. J Clin Endocrinol Metab. 1988;67(3):607-13.
-
Townsend K, Banwell CM, Guy M, Colston KW, Mansi JL, Stewart PM, Campbell MJ, Hewison M. Autocrine metabolism of vitamin D in normal and malignant breast tissue. Clin Cancer Res. 2005;11(9):3579-86.
-
Lopes N, Paredes J, Costa JL, Ylstra B, Schmitt F. Vitamin D and the mammary gland: a review on its role in normal development and breast cancer. Breast Cancer Res. 2012;14(3):211.
-
Spina CS, Tangpricha V, Uskokovic M, Adorinic L, Maehr H, Holick MF. Vitamin D and cancer. Anticancer Res. 2006;26(4A):2515-24.
-
Alipour S, Hadji M, Hosseini L, et al. Levels of serum 25-hydroxyvitamin D in benign and malignant breast masses. Asian Pac J Cancer Prev. 2014;15(1):129-32.
-
Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clin Proc. 2010;85(8):752-7.

December 2023 – February 2024 Calendar
December 2023 – February 2024 Calendar...
Synchronous endometrial and ovarian carcinoma, endometrioid type – a pathologist’s insight. Case report
Maria Olinca, Anca Potecă, Elvira Brătilă, Mihai Mitran
Synchronous endometrial and ovarian carcinomas (SEOC) represent a relatively rare yet clinically significant occurrence where malignant tumors arise concurrently in the endometrium and ovaries. ...
The utility of prophylactic salpingectomy – case report
Dan Cozmei, Oana Ursică, Sorin Vameşu, Constantin Viorel Cristurean, Vlad-Iustin Tica
Pelvic high-grade serous carcinoma – including ovarian carcinoma, tubal carcinoma and primary peritoneal carcinoma – has an important clinical significance because of the rapid progression and extension of the disease a...
The utility of prophylactic salpingectomy – case report
Dan Cozmei, Oana Ursică, Sorin Vameşu, Constantin Viorel Cristurean, Vlad-Iustin Tica
Pelvic high-grade serous carcinoma – including ovarian carcinoma, tubal carcinoma and primary peritoneal carcinoma – has an important clinical significance because of the rapid progression and extension of the disease a...
Cervical ectopic pregnancy – case report
Fernanda-Ecaterina Augustin, Ionuţ Vâlcea, Mihaela Amza, Romina-Marina Sima, Liana Pleș, Ileana-Maria Conea
The definition of an ectopic pregnancy (EP) is that of a pregnancy where implantation occurs outside the endometrial cavity. Roughly 95% of EPs take place in the fallopian tube. Unusual locations include the cervix, a ru...