Evaluarea ecografică a cavităţii orale fetale - studiu retrospectiv
Ultrasound assessment of the fetal oral cavity - our experience
Abstract
Introduction. The oral cavity can be assessed by ultrasound from 11 weeks onwards, in a more and more detailed manner as pregnancy progresses.Method. Our study followed 100 first trimester cases (11-13,6 weeks) and 100 second-trimester cases, following two different protocols.
Results and discussions. The used protocols targeted mainly the diagnosis of facial clefts, but also other abnormalities of the oral cavity were reported. The results showed that protocols designed were efficient and easy to follow. This paper also presents three pathological cases that were encountered during this study: two facial clefts with moderate and severe involvement of the posterior palate and one case of Pierre-Robin syndrome diagnosed with the help of our standardized protocol by detecting an abnormal profile and an abnormal position of the tongue. Conclusion. The protocols we developed seem to work in a standard scan without creating difficulties in the normal workflow. All sonographers participating in the study, from PhD students to experienced examiners, found the protocols useful and felt they increased the confidence in the diagnosis of oro-facial pathology or even in confirming the normal aspect.
Keywords
oral cavityfacial cleftsRezumat
Introducere. Cavitatea orală poate fi evaluată ecografic începând cu 11 săptămâni, într-o manieră din ce în ce mai detaliată, pe măsură ce sarcina progresează.Metodă. Studiul nostru a urmărit 100 de cazuri de primul trimestru (11-13,6 săptămâni) și 100 de cazuri de trimestru doi, urmând două protocoale diferite.
Rezultate și discuții. Protocoalele folosite au vizat, în principal, diagnosticul de cheiloschizis și cheilopalatoschizis, dar au fost raportate și alte anomalii ale cavității orale. Rezultatele au arătat că protocoalele concepute au fost eficiente și ușor de urmărit. Această lucrare prezintă, de asemenea, trei cazuri patologice care au fost întâlnite în timpul acestui studiu: două defecte de buză şi palat, cu implicarea moderată și severă a palatului posterior, și un caz de sindrom Pierre-Robin, diagnosticat cu ajutorul protocolului nostru standard, prin detectarea unui profil anormal și a unei poziții anormale a limbii.
Concluzie. Protocoalele pe care le-am dezvoltat par să funcționeze integrate într-o examinare standard, fără a crea dificultăți în fluxul normal de lucru. Toți examinatorii care au participat la studiu, de la doctoranzi la examinatori experimentați, le-au găsit folositoare și au simțit că sporesc încrederea în diagnosticul patologiei oro-faciale sau chiar în confirmarea aspectului normal.
Cuvinte Cheie
cavitate oralădefecte facialeIntroduction
Although the oral cavity is almost fully developed at the 11-13,6 weeks scan, limited resolution stands in the way of a full assessment at this gestational age. All studies regarding the first trimester oral cavity pathology are targeted to facial clefts with some insight of the extent of maxillary involvement. However, we believe that when certain markers are identified, the use of a transvaginal probe with a high resolution will make more details available, allowing an earlier diagnosis of more complex pathology. In the second trimester, more details regarding the oral cavity are accessible and information about tongue and soft palate are available, despite many times the hard part of the posterior palate remains hidden in the shadow of the alveolar ridge. Even though we are in the age of 3D, 4D and even 5D ultrasound, we believe that the answer for diagnosing pathology of the oral cavity on a routine basis lies in standardized 2D protocols.
Method
Our study targeted the assessment of the oral cavity at two different gestational ages, by two teams. Team A (AC Comanescu, EM Barbu si A Popa) targeted pregnancies between 11 and 13,6 weeks. Team B (OC Sirbu, MC Comanescu si M Hirnau) targeted pregnancies between 20 and 24 weeks. The protocols were as follows:
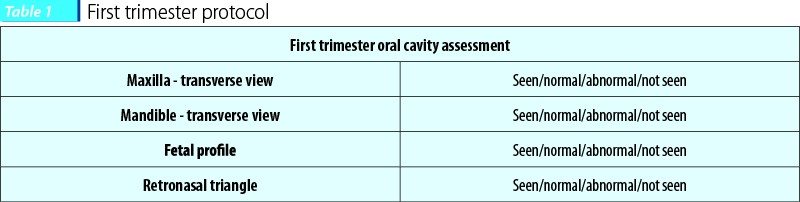
For first trimester scans, the targets had to be classified in seen (a section of the target can be obtained), normal (the sonographer is sure that it is a normal structure), abnormal (the sonographer is sure that it is an abnormal structure), not seen (a standard section could not be obtained).
Targets were chosen based on their described efficiency in diagnosing facial clefts in the first trimester in current literature.
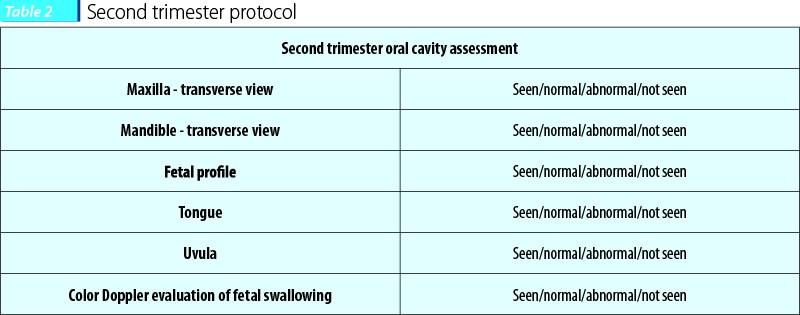
For second trimester scans, we chose the following sections based on preexisting routine guidelines and personal experience from previous cases.
The purpose of the study was to evaluate the ease of use of these markers/standard sections and their efficiency in pathological cases. All images obtained were evaluated by a member of the team not involved in the examinations, but aware of the targets of the study (NC). All images were obtained on a Voluson 730 Pro ultrasound machine (GE Healthcare, Kretz Ultrasound, Zipf, Austria) using a 4-8 MHz transabdominal ultrasound probe and/or a transvaginal 5-9 MHz probe. The study was developed in the Department of Obstetrics and Gynecology, Prenatal Diagnostic Unit, University of Medicine and Pharmacy of Craiova.
Results and discussions
First, we would like to make a short discussion regarding our choices for first and second trimester protocol. Developed initially for diagnosing the absent nasal bone, Sepulveda’s retronasal triangle is one of the most common sections used for diagnosing facial clefts in the first trimester(1). The maxillary gap sign, described by Chaoui on the standard fetal profile section in the first trimester, is extremely accessible since this image is the standard for the combined screening, being the same image we routinely use for nuchal translucency and nasal bone assessment(2). Maxillary assessment is done for obvious reasons. Mandible assessment can reveal an abnormal shape that may lead to further investigations.

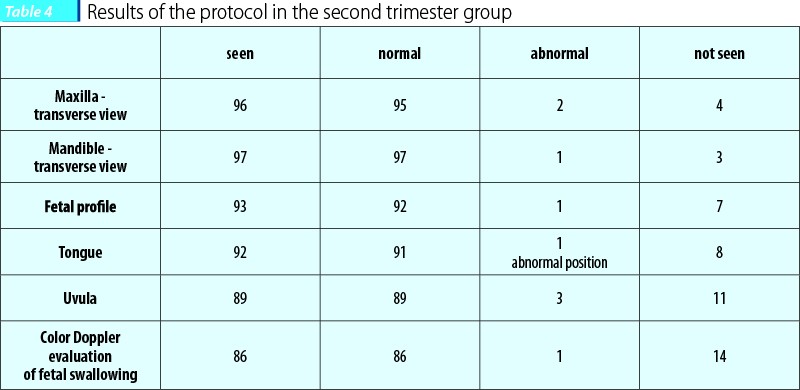
At 22 weeks we can make a more complete evaluation including the position of the tongue and the presence of the uvula. On a study on 667 patients with a gestation age between 20 and 25 weeks, L. Wilhelm and coworkers showed that a normal uvula and soft palate is visible at about 90% of cases and that an abnormal image is associated with a pathology of the posterior palate(3). Fetal swallowing can be evaluated in standard 2D or using Color Doppler - HD-flow has been shown to be efficient in the evaluation of the oral cavity during fetal swallowing(4). The fetal profile has been found helpful in the diagnosis of micro and retrognasia; also, the measurement of the MNM (maxilla-nasion-mandible angle) has been helpful in the diagnosis of the fetal profile pathology by enabling an objective assessment of the anteroposterior relationship of the jaws and helping us supporting the diagnosing of retrognathia, maxillary alveolar ridge interruption and flat profile(5).
Each team examined 100 cases that presented or were referred to the Prenatal Diagnosis Unit from their assigned gestational age. Team A (first trimester) had no pathological cases. Team B (second trimester) had three pathological cases, two facial clefts and one isolated posterior palate defect that was diagnosed based on fetal profile and tongue assessment.
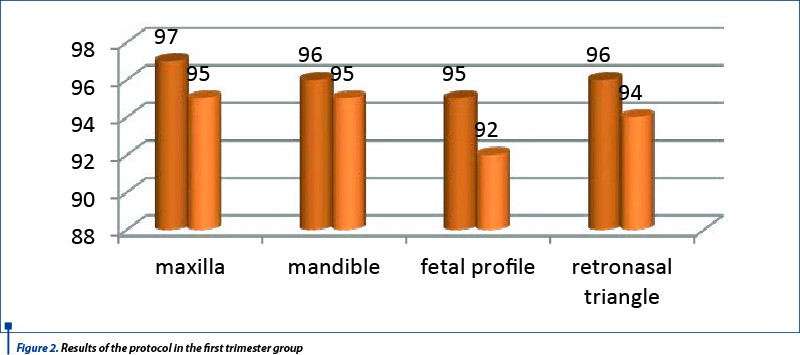
Team A results showed that the protocol established was easy to follow, with more than 90% efficiency in obtaining he sections.
All sections were considered fairly easy to be obtained. Transvaginal and transabdominal probes were both used. There was a greater comfort in confirming normality when transvaginal images were obtained. Though not a target of this protocol, all examiners felt confident that more details, like the tongue and posterior palate and pharynx, could be assessed at 11-13,6 weeks using transvaginal ultrasound.

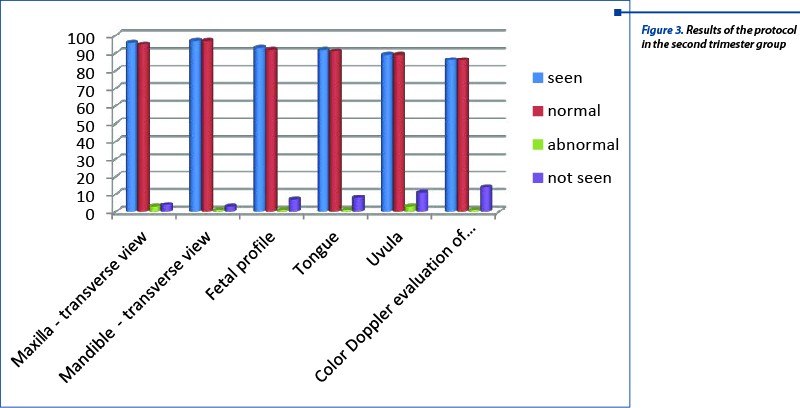
Team B results are shown in Figure 3 and Table 4, and reveal a good reliability of the protocol and high efficiency in the diagnosis of the three pathological cases.
The three pathological cases were as mentioned above: two facial clefts and one posterior palate defect (part of a Pierre-Robin syndrome). We evaluated how our protocol performed in pathological cases. Another important aspect is that two of the patients had no anomaly scan done during the first trimester and one had a combined test done at 11 weeks with a minimal evaluation of the fetal anatomy. We believe that using our first trimester protocol, at least two of these cases could have been diagnosed before 14 weeks.

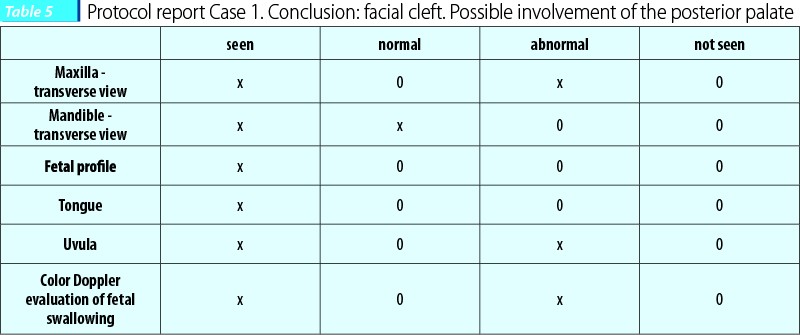
Case 1. A patient presented at 23 weeks in the Prenatal Diagnosis Unit. She had no first trimester anomaly scan. She had however done an NIPT (non-invasive prenatal testing), that showed no chromosomal anomalies related to chromosomes 13, 18 and 21. The fetus presented an abnormal maxillary transverse view. Initial images seemed to reveal only an involvement of the anterior palate, but further images revealed the involvement of the posterior palate.
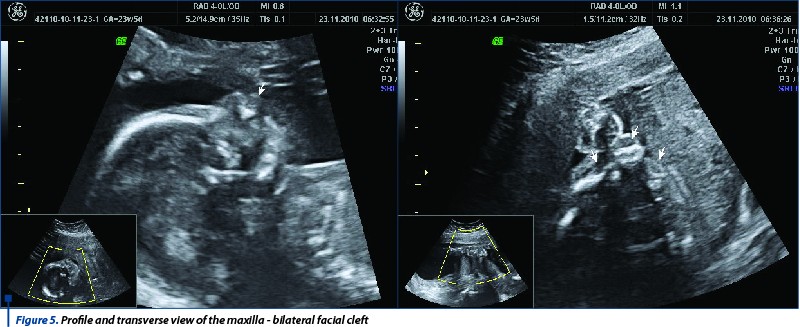
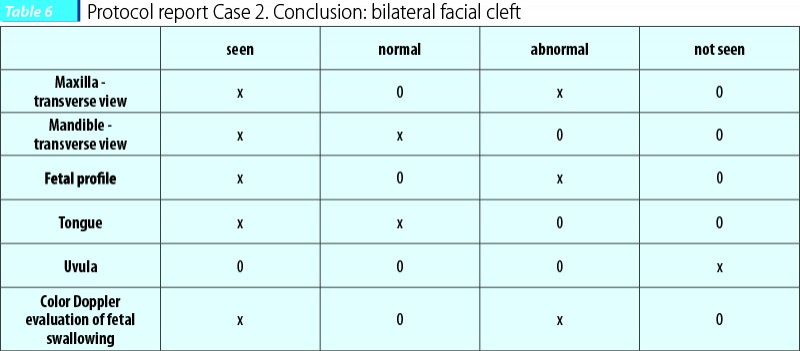
Case 2. The patient presented at 20 weeks for an ultrasound evaluation. She had one previous ultrasound at 8 weeks and no screening for chromosomal anomalies. The scan of the fetal face started with the profile which was considered abnormal. The maxillary transverse view that followed was capital for the diagnosis - bilateral cleft. Some structures (the uvula) could not be assessed but HD-flow monitoring of the fetal swallowing showed an abnormal pattern.
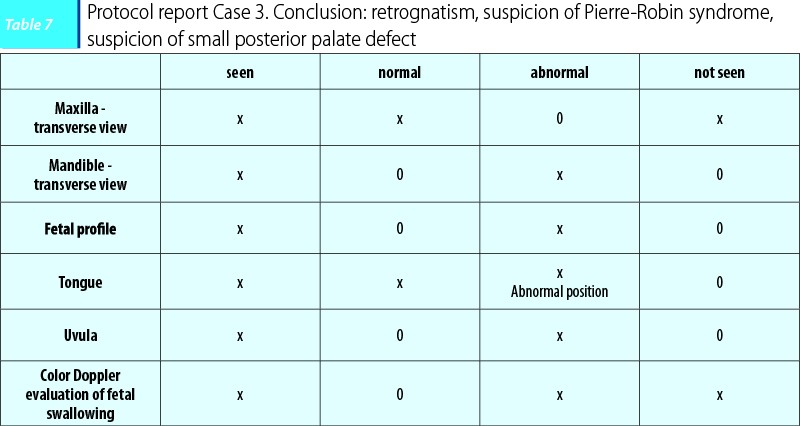
Case 3. A patient arrived for the 22-week anomaly scan. She had a normal combined test performed at 11+3 weeks. When fetal profile was analyzed, retrognasia was noticed. Further study revealed a malposition of the tongue, positioned posteriorly in the pharynx, unable to reach the lips throughout the examination. Mandible looked abnormal in shape and moderately smaller in size. HD-flow monitoring during fetal swallowing revealed an abnormal pattern that suggested the presence of a posterior palate defect.

Conclusions
The protocols that we developed seem to work in a standard scan without creating difficulties in the normal workflow. All sonographers participating in the study, from PhD students to experienced examiners, found them useful and felt they increased the confidence in the diagnosis of oro-facial pathology or even in confirming the normal aspect.
Bibliografie
1. Sepulveda W, Wong AE, Martinez-Ten P, Perez-Pedregosa J. Retronasal triangle: a sonographic landmark for the screening of cleft palate in the first trimester. Ultrasound Obstet Gynecol, 2010; 35:7–13.
2. Chaoui R, Orosz G, Heling KS, Sarut-Lopez A, Nicolaides KH. Maxillary gap at 11–13 weeks' gestation: marker of cleft lip and palate. Ultrasound Obstet Gynecol, 2015; 46: 665–9.
3. Wilhelm L, Borgers H. The ‘equals sign’: a novel marker in the diagnosis of fetal isolated cleft palate. Ultrasound Obstet Gynecol, 2010; 36:439–44.
4. Comănescu A, Cernea N, Tănase F, Tica O, Barbu M, Comănescu C. EP10.06: HD-flow use in the study of the posterior palate defects: pilot study. Ultrasound Obstet Gynecol, 2017; 51:297.
5. de Jong-Pleij EAP, Ribbert LSM, Manten GTR, Tromp E, Bilardo CM. Maxilla-nasion-mandible angle: a new method to assess profile anomalies in pregnancy. Ultrasound Obstet Gynecol, 2011; 37:562–9.

Consecinţele sarcinii la adolescente
Mihai Mitran, Daniela Stan
Sarcinile neplanificate sunt întotdeauna pline de provocări, dar pot fi chiar extrem de dificile, mai ales în cazul în care părinții sunt adolescenți. Când vine vorba de o sarcină la vârsta adolescenței, există anumite probleme de sănătate, financiare și emoționale, de care trebuie să se țină seama....
Factorul de creștere insulin-like (IGF1), sarcina și retinopatia de prematuritate (ROP)
Adriana Dan, Valeriu Horhoianu
Retinopatia de prematuritate (ROP) este o complicație tardivă oculară care survine la nou-născuții cu vârste de gestație și greutăți mici; ea constă în anomalii de dezvoltare a vascularizației retiniene cauzate de inte...
Restaurarea coronară directă cu pivot din fibră de sticlă în sarcină - prezentare de caz
Irina-Maria Gheorghiu, Paula Perlea, Claudiu-Gabriel Ciolan, Loredana Mitran, Ioana Suciu, Mihai Mitran
În cadrul tratamentelor dentare care sunt necesare în cursul perioadei de sarcină, situațiile clinice în care pacienta prezintă o distrucție coronară masivă de etiologie variată ocupă o pondere import...
Managementul gravidei cu hepatită virală B cronică - review de literatură şi prezentarea experienţei Spitalului Clinic de Obstetrică-Ginecologie „Prof. Dr. Panait Sîrbu”, Bucureşti
Octavia Velicu, Roberta Ciobanu, Ioan Diaconu, Elvira Brătilă, Mihai Mitran
Managementul hepatitei virale B cronice în timpul sarcinii rămâne o provocare și implică numeroase aspecte de îngrijire materno-...
Defectul septal ventricular fetal - tipuri și evoluţie naturală
Alexandra Bruja, Mihai Mitran, Elvira Brătilă
Defectul septal ventricular (DSV) este una dintre cel mai frecvent întâlnite malformaţii cardiace congenitale. Se poate prezenta sub forma unei anomalii cardiace congenitale izolate sau poate fi parte componentă în cadru...