Giant isthmic fibromatous nodule developing within the cervix – clinical case
Nodul fibromatos gigant istmic cu dezvoltare la nivelul colului uterin – caz clinic
Abstract
Isthmic-cervical leiomyomas can grow very large and cause extreme discomfort. The surgical removal of these leiomyomas is a technical challenge, with an increased risk of operative and postoperative complications. This paper presents the case of a patient with a gynecopathy who presented herself to our clinic, having been diagnosed with a giant isthmic-cervical fibromatous nodule which was developing within the cervix and required extended surgery – i.e., the radical dissection of the pelvis, to ensure the success of the total en bloc hysterectomy. The radical pelvic dissection at the time of the total en bloc hysterectomy is necessary in most cases of large isthmic-cervical fibroids, to minimize the risk of intraoperative and postoperative complications. These isthmic-cervical fibroids have a very difficult surgical approach. Ideally, the medical team should be pluridisciplinary, and the gynecologist should do the surgery together with a general surgeon and a urologist. To conclude, the surgical treatment of giant isthmic-cervical fibroids should be personalized and individualized.Keywords
isthmusisthmiccervicalleiomyomasurgical approachRezumat
Leiomioamele cervicoistmice pot atinge dimensiuni mari şi pot provoca un disconfort extrem. Îndepărtarea chirurgicală a acestor leiomioame este o provocare tehnică, cu un risc crescut de complicaţii operatorii şi postoperatorii. Lucrarea prezintă cazul unei paciente cu o ginecopatie, care s-a prezentat în clinica noastră, fiind diagnosticată cu un nodul fibromatos gigant istmic cu dezvoltare la nivelul colului uterin şi care a necesitat intervenţie chirurgicală extinsă, respectiv disecţia radicală a pelvisului, pentru a se asigura succesul histerectomiei totale en bloc. Disecţia pelviană radicală în momentul histerectomiei totale en bloc este necesară în majoritatea cazurilor de fibroame cervicoistmice mari pentru a minimiza riscul de complicaţii intraoperatorii şi postoperatorii. Aceste fibroame cervicoistmice au un abord chirurgical foarte dificil. De aceea, ideal este ca echipa de medici să fie pluridisciplinară, iar medicul specialist ginecolog să efectueze intervenţia chirurgicală împreună cu medicul specialist de chirurgie generală şi medicul specialist urolog. În concluzie, tratamentul chirurgical al fibroamelor gigante cu localizare cervicoistmică trebuie să fie personalizat şi individualizat.Cuvinte Cheie
istmistmiccervicalleiomiomabord chirurgicalIntroduction
The fibromatous nodule (uterine fibroid) is a benign tumor that develops from tissue similar to the uterine muscle, being aided by an increased level of estrogens. It is the most frequent noncancerous tumor that develops from the muscular wall of the uterus, and it affects more than half of women; the maximum incidence of uterine fibroids is in perimenopause(1).
Fibroids are hormone-dependent tumors which appear in the reproductive period and tend to regress after menopause sets in(1).
Also known as a myoma, a fibromyoma or a leiomyoma, the uterine fibroid is made up of smooth muscle fibers, conjunctive tissue and blood vessels.
The incriminating risk factors for the appearance of uterine fibroids are: hyperestrogenism, excess weight, genetic factors, early menarche and late menopause.
The uterine fibroid consists in single or multiple round tumors, firm in consistence, small or very large in size (giant tumors), which occupy most of the abdomen, without clinical manifestations, asymptomatic (silent fibroid) or with loud clinical manifestations. There are several types of uterine fibroids(2):
- Corporeal fibroids – these are the most frequent uterine fibroids and are located within the uterine body. Depending on the area where they develop, there are three types of corporeal fibroids – intramural (when they develop within the uterine wall), submucosal (when they develop towards the uterine cavity), and subserosal (when they develop outside the uterus).
- Intraligamentary fibroids – these are fibroids which develop entirely outside the uterus.
- Cervical and isthmic-cervical fibroids – these are very rare in the medical practice; they are rather voluminous and occupy variably the abdominal cavity which they increase in volume mostly suprasymphyseal and subumbilically; they produce compressive complications in the adjacent organs with clinical manifestations such as pollakiuria, dysuria, urinary incontinence, bloating, chronic constipation, dyspareunia, pelvic or abdominal pressure, pelvic or pelvic-abdominal pain.
In the case of isthmic-cervical fibroids, the ureters can be compressed, generating the dilation of the urinary tract or hydronephrosis, with the risk of causing urinary infections. When these fibroids are voluminous and generate compressive phenomena at the level of the urinary bladder, the ureters, the rectum and the iliac vessels, there may appear proximity disorders, such as intestinal motility disorders, mictional difficulties, compressive complaints at the level of the pelvic vessels, causing venous thromboses on the pelvic members. The greater a fibroid is, the higher the chance of it becoming symptomatic. These isthmic-cervical fibroids also have a very difficult surgical approach. Ideally, the team should be pluridisciplinary, and the gynecologist should perform the surgery together with the general surgeon and the urologist(2).
Such a giant isthmic-cervical fibroid, with compressive complications at the level of the adjacent organs, was operated on at the “Elena Doamna” Clinical Hospital of Obstetrics and Gynecology, Iaşi, Romania, by a pluridisciplinary team (a gynecologist, a general surgeon, a urologist, and an intensive care physician).
Materials and method
This clinical case refers to a patient with a gynecopathy, aged 45 years old, living in Iaşi, Romania, who came to the maternity hospital with intense pelvic pain which radiated to the lumbar region, the iliac fossae and the lower limbs, the pelvic pain radiating more towards the right iliac fossa and the right thigh, with repetitive menometrorrhagia for about six months (declarative), compressive phenomena at the level of the urinary bladder (mictional difficulties), compressive phenomena at the level of the rectum (intestinal motility disorders), fatigability, asthenia, panic attacks, dyspareunia, and the growth in volume of the abdomen subumbilically.
Among the family medical history antecedents and the personal physiological and pathological ones, we have to mention that the onset of the menarche was at the age of 12 years old, with regular menstrual cycles (28/6), the patient had three vaginal births with no complications, three abortions upon request, and glaucoma; she had been diagnosed by a psychiatrist with depressive-anxiety syndrome with panic attacks (medicated), stable effort-induced angina pectoris, chronic overwork syndrome (medicated), modified basal glycemia, and appendectomy.
The general clinical examination revealed an anxious person, mildly neurotic and irritable, a person who requested upon admission to hospital (because of the intense pelvic pain that radiated to the lumbar region and the lower members) the radical surgery.
We must mention the fact that the patient did not work, did not drink alcohol (declarative), but she smoked, on average, 20 cigarettes/day (declaratively).
Upon admission, the patient was under the following treatment: Xanax® 0.25 mg (2 cp./day), Nebilet® 5 mg (1-2 cp./day), Preductal® 35 mg (2 cp./day), Sortis® 20 mg (1 cp./day), Prestarium® 5 mg (1 cp./in the evening).
The abdominal inspection revealed the existence of the abdominal incision post-appendectomy, a well-represented panniculus adiposus and a consistently enlarged abdomen, especially subumbilically, suprasymphyseal and towards the flanks.
The local examination (VVE and DVE) revealed a vaginal mucosa with a normal aspect, whitish leucorrhea in medium quantity, ascended cervix, deviated laterally, occupied by the formation, but the external orifice of the cervix could not be revealed (not even with the help of the vaginal speculum), the external orifice of the cervix being enclosed in the formation (modified anatomically by the tumor), which is why the Pap smear could not be performed preoperatively.
Also, during the local examination (DVE combined with the abdominal palpation), a large voluminous tumor (120/130 mm) stood out. It was hard, regular, with very low mobility (almost immobile), developed at the level of the cervix, isthmic-lateral right, which put great pressure at the level of the lesser pelvis, being located very low, a slightly larger uterus, hard, with a regular contour, non-palpable adnexa and a pouch of Douglas occupied by the formation (we must mention the fact that the palpation was done with great difficulty since the patient did not collaborate to a full extent with the medical personnel due to the pain she had during the examination).
The large volume formation developed at the level of the cervix isthmic-cervically, putting pressure on the lesser pelvis, which explained the pain mentioned by the patient (in the right iliac fossa, radiating in the right thigh), and the compression produced by the tumor on the neighboring structures brought about the urinary and intestinal motility issues.
In the absence of the external orifice of the cervix, we supposed (preoperatively) that the formation developed at the level of the cervix, encasing the external orifice of the cervix, but having as starting point either at the level of the uterine isthmus (rare cases in the medical practice), something that was confirmed intraoperatively, or at the level of the uterine body, which is where most fibroids are located.
The lab tests run in the hospital highlighted the presence of iron deficiency anemia (Hgb=8 g/dl, Hct=30%, serum ferritin=95 ng/mL), higher ESR (35 mm after 1 hour and 70 mm after 2 hours), an increased C-reactive protein qualitative test and glycemia of 120 mg/dl, the rest of the blood and urinary tests being within normal limits.
The cytobacteriological smear together with the vaginal culture and antibiogram have identified the presence of vaginal candidiasis, for which the patient received preoperatively specialized treatment (orally and vaginal preparations); the cytodiagnostic smear could not be done due to the absence of a visible external orifice of the cervix in the vagina.
To establish a clear diagnosis before the surgery we were going to undertake, we indicated an endovaginal ultrasound and an abdominopelvic CT scan.
The endovaginal ultrasound highlighted a slightly enlarged uterine body (as palpated during the DVE) and the cervical canal entirely occupied by a hyperechogenic, nonhomogeneous, large formation (123/100/111 mm), left ovary of 37/26/36 mm situated in an elevated position with a 26 mm follicle; the right ovary was not visualized due to the formation that was extended more towards the right, the pouch of Douglas being occupied completely by the formation.
The diagnostic established at the endovaginal ultrasound (corroborated with the data obtained during the clinical examination) was that of isthmic fibroid developed entirely within the cervix.
This is an extremely rare case in medical practice (there are few cases cited in the specialized literature), and it requires a very thorough preoperative preparation, a well trained and experienced gynecology surgeon, and a pluridisciplinary team (gynecologist, general surgeon, urologist, and intensive care physician).
Due to the complexity of the case (a large formation developed within the cervix) together with the compressive phenomena at the level of the urinary bladder and the compressive phenomena at the level of the rectum, but also to establish a very precise diagnosis before the radical surgery and, most importantly, to reveal the connections of the tumor with the ureters, the urinary bladder and the rectum, an abdominopelvic CT scan with contrast was asked for.
The data obtained from the abdominopelvic CT scan with contrast (IOPAMIRO) were as follows:
- Liver partially comprised in the scanned volume, presenting at the level of segment VI a cyst with a diameter of 4 mm.
- The highly elevated left ovary presented a thin-walled cyst with a diameter of 23 mm and a thin wall.
- The right ovary had no modifications visible on the CT.
- The uterus had at an isthmic level and prolonging into the cervix, which it occupied entirely, a prominent formation, highly delineated with contrast medium uptake, nonhomogeneous, without calcifications, with an approximate size of 119/107/131 mm (AP/T/CC); numerous neoformation vessels at the intralesional level, having as a source both adnexa; the actual uterine cavity occupied by liquid with a thickness below 5 mm.
- The right ovarian vein was dilated by 10 mm (by compression).
- The urinary bladder with reduced content was imprinted by the visualized formation (by compression).
- No free intraperitoneal liquid or iliac adenopathy was found.
- An umbilical hernia with a collar of 5 mm, with properitoneal adipose content.
The diagnostic established after the abdominopelvic CT with contrast was: isthmic-cervical fibromatous nodule, simple liver cyst, left ovary cyst.
The diagnostic given by the abdominopelvic CT (isthmic-cervical fibromatous nodule) was corroborated with the endovaginal ultrasound diagnostic (isthmic fibroid developed entirely within the cervix) and the clinical examination done in the hospital, our case being extremely rare in the medical practice and requiring personalized surgical management.
The diagnostic upon admission was that of hemorrhagic fibroid uterus with chronic pelvic pain syndrome which worsened progressively in the last few years, as the condition progressed; glaucoma, anxiety-depressive syndrome with panic attacks (medicated), stable effort-induced angina pectoris, chronic overwork syndrome (medicated), modified basal glycemia, appendectomy, and type 2 obesity.
The diagnostic given after 72 hours (after specialized examinations) was that of giant isthmic fibroid developed entirely within the cervix, an extremely difficult and complex surgical case, due to involving the ureters, urinary bladder, rectum, iliac vessels and uterine arteries, which made us request the forming of a pluridisciplinary team (gynecology surgeon, general surgeon, urology surgeon, and intensive care physician); glaucoma, anxiety-depressive syndrome with panic attacks (medicated), stable effort-induced angina pectoris, chronic overwork syndrome (medicated), modified basal glycemia, appendectomy, and type 2 obesity.
The surgery that we were going to perform was very difficult, because of the very low location of the tumor, which was very large, difficult to access intraoperatively, almost immobile, and had completely enclosed the external orifice of the cervix, modifying the anatomical planes.
The very low location of the tumor (within the cervical canal) made it compress the neighboring structures, firstly generating pain, which was localized laterally, to the right, at the level of the pelvis, towards the right iliac fossa and the right lower limb, then compressing the rectum, generating constipation and compressing the urinary bladder, causing urinary disorders.
The team of doctors who performed the surgery was pluridisciplinary (gynecology surgeon, general surgeon, urology surgeon, and intensive care physician), due to the important connections of the tumor both with the ureters and the uterine vessels, iliac vessels, urinary bladder and rectum.
It was a very difficult surgery. In all cases of giant isthmic-cervical fibroids, it is recommended to perform a total abdominal hysterectomy en bloc with the radical dissection of the pelvis, the surgical management of large isthmic-cervical fibroids needing to be personalized and individualized preoperatively to ensure the success of the surgery.
We performed the surgery with a classical approach, with general anesthesia, doing a subumbilical midline incision that we prolonged distally bypassing the umbilicus, to obtain a larger operating field (operating protocol of 9 March 2023)
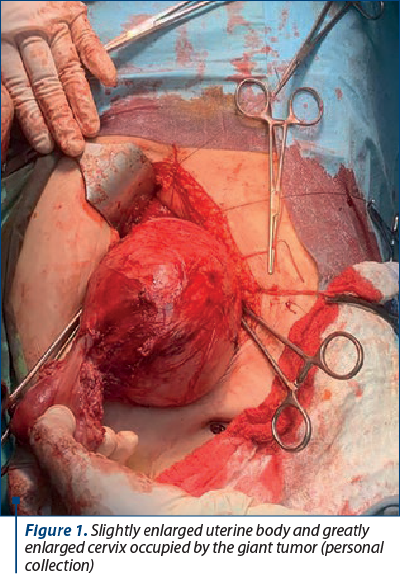
Operating protocol – subumbilical midline incision prolonged distally; upon opening the peritoneal cavity, multiple adhesions, parietal peritoneal, between the greater omentum and the peritoneum, vesicouterine, were noticed; the adhesiolysis was done with great difficulty; the uterine body was slightly larger, the right adnexa had a normal aspect, the left ovary had a small cyst and the cervix was greatly enlarged, containing a tumor of approximately 15 cm in diameter, inhabiting the interior of the cervix, up to the upper third of the vagina – Figure 1.
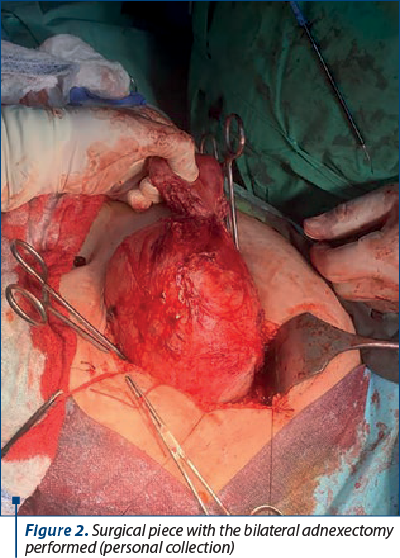
We performed a bilateral adnexectomy to create more surgical space; the uterine body was skeletonized (Figure 2).
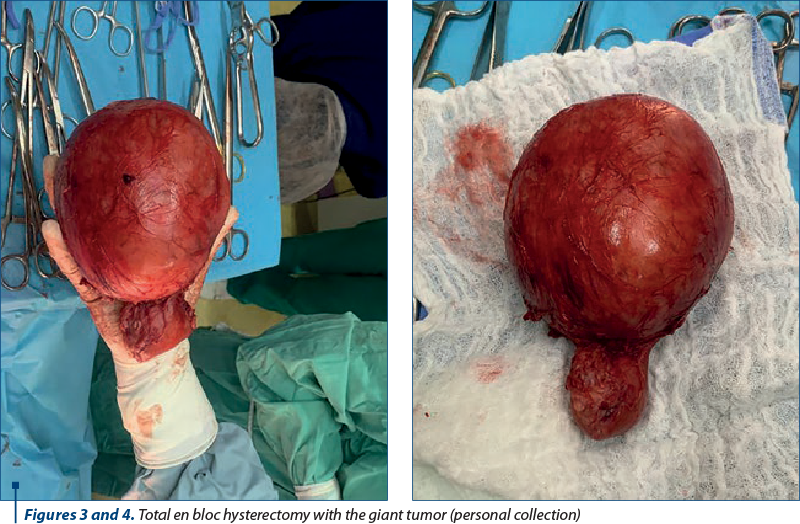
Peritoneal detachment; dissection of the retroperitoneal space; development of the rectovaginal, pararectal, vesicovaginal and paravesical spaces; total en bloc hysterectomy with the giant tumor; the pieces that were taken were sent to the pathology department – Figures 3 and 4.
We checked the integrity of the ureters; the ureters were visible bilaterally and integral; we performed the lavage of the abdominal cavity with a betadine solution; we sutured the remaining vaginal stump with continuous absorbable suture no. 1; we checked the hemostasis – the hemostasis was efficient; we placed a drain in the pouch of Douglas through which the patient drained in the first 24 hours after the surgery approximately 80 ml of serosanguineous fluid; visceral peritonization; restoration of the wall in anatomical plans; separate suture threads on the skin; sterile dressing; complete count of the soft material.
Postoperatively, the evolution of the patient was favorable. She followed a five-day antithrombotic, antalgic and antibiotic treatment. The patient was discharged from hospital on the fifth day, and on the nineth day we suppressed the separate suture threads.
Afterwards, the evolution of the patient was favorable, the checkups at one, three and six months after the surgery being within normal parameters.
We do not have information about the health of the patient 12 months after the surgery, because she did not present at her appointment.
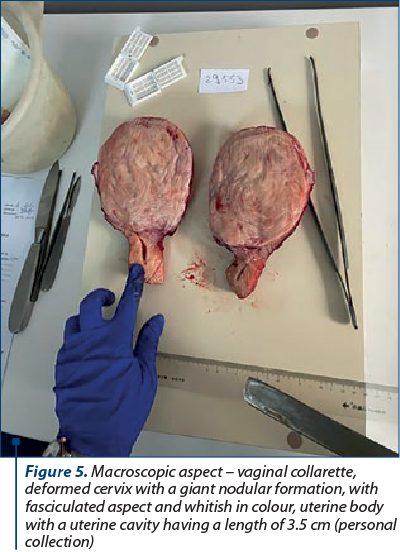
The histopathological examination revealed, from a macroscopic point of view, a total hysterectomy piece with bilateral adnexectomy made up of (Figure 5):
- Vaginal collarette approximately 3.5 cm in length.
- Deformed cervix of 11/11.5/9.5 cm with a smooth shiny exocervix and an endocervix permeable for the probe. The section revealed a nodular formation of 11/11.5/9 cm, with a fasciculated aspect, whitish in color and with a firm-elastic consistency.
- Uterine body of 6/4/4.5 cm with an intact smooth serosa, and a uterine cavity with a length of 3.5 cm.
- Left adnexa – salpinx with a length of 3.5 cm, with a maximum diameter of 0.6 cm. Ovary of 3.5/1/0.8 cm which had a subcapsular cystic formation of 0.7 cm in diameter with smooth internal walls and containing serous citrine fluid.
- Right adnexa – salpinx with a length of 4.5 cm, with a maximum diameter of 0.6 cm. Ovary measuring 3.5/2/1 cm.
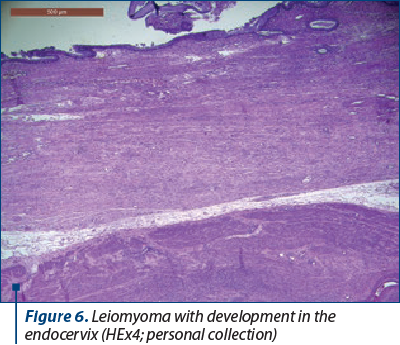
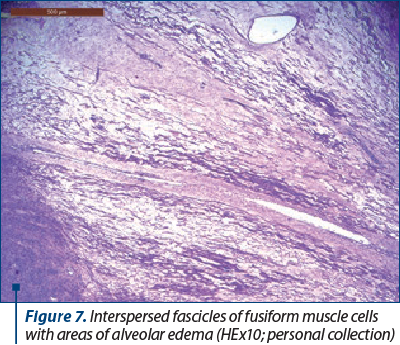
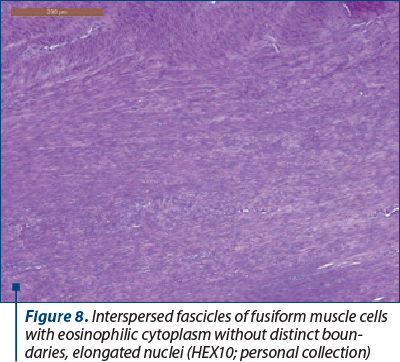
The histopathological diagnosis (hematoxylin eosin staining) revealed, from a microscopic point a view (Figures 6, 7 and 8):
- Uterine body – leiomyoma with edematous area, rare adenomyosis foci, secretory endometrium.
- Cervix – narrowed areas of endocervical and exocervical mucosa due to the expansion of the leiomyoma.
- Right ovary – hemorrhagic corpus luteum, corpus albicans.
- Left ovary – corpus albicans, epithelial inclusion cyst.
- Right fallopian tube – without microscopic changes.
- Left fallopian tube – without microscopic changes.
Results and discussion
Isthmic-cervical leiomyomas can reach large sizes and can cause extreme discomfort. The surgical removal of these isthmic-cervical leiomyomas is a technical challenge, with an increased risk of operative and postoperative complications. Isthmic-cervical leiomyomas are treated surgically, but the surgery requires good preoperative preparation and a well-trained and experienced gynecology surgeon. In all cases of giant isthmic-cervical fibroids, the radical total abdominal hysterectomy is recommended(1).
Our case of giant isthmic-cervical leiomyoma required the radical dissection of the pelvis to ensure the success of the total hysterectomy. The radical pelvic dissection at the time of the hysterectomy is necessary in all cases of large isthmic-cervical leiomyoma to minimize the risk of intraoperative complications(1).
This is the reason why the surgical management of large isthmic-cervical fibroids must be personalized and individualized, and a pluridisciplinary medical team needs to be present.
The uterine leiomyoma is the most frequent benign tumor of the female genital tract, which appears in 30-50% of women over 35 years old(1).
The cervical leiomyoma is less frequent, being estimated to appear in 0.6% of cases(2). The cases of giant isthmic-cervical leiomyoma – such as the one we successfully solved in our hospital – are even more rare.
Isthmic-cervical leiomyomas are histologically identical with those found in the uterine body. However, they can reach very large sizes (like in our case) and have a particularly extended vascularization, with intraoperative hemorrhagic risk. These giant isthmic-cervical fibroids can affect (include) the orifices of the cervix and can significantly distort pelvic anatomy, thus compromising the surgical field.
These factors explain the difficulty of their surgical excision and the high risk of operative complications, such as hemorrhage, lesions of the rectum and lesions of the urinary tract.
In our case, taking into consideration the age of the patient and the very difficult location of the tumor, it was necessary to perform an operation called radical total extended hysterectomy, which is the complete removal of the uterus, a surgery in which participated a pluridisciplinary medical team (gynecologist, general surgeon, urologist, and intensive care physician)(2).
A MEDLINE (bibliographical database) search was conducted, using the keywords “isthmus”, “isthmic”, “cervical”, “intramural”, “leiomyoma” and “surgical approach”, from January 1970 to January 2023(3).
After this search, only a few cases of giant isthmic-cervical leiomyoma were found (rarities), including an article that describes the difficulties encountered during the surgery(3).
We found no article that defined or standardized the surgical approach to these large fibroids with unusual locations (isthmic-cervical)(3).
In our case, the laparotomy revealed the left ovary which had a small cystic formation, the right adnexa which had a normal aspect, a slightly enlarged uterine body, and a large isthmic-cervical formation that extended approximately from the lower pelvis to the upper third of the vagina.
The surgery we performed was modified radical abdominal hysterectomy, with bilateral adnexectomy and adhesiolysis, in which the blood loss was estimated at 400 ml.
The retroperitoneal space was dissected and the rectovaginal, pararectal, vesicovaginal and paravesical spaces were developed to facilitate the dissection of the anterior, lateral and posterior parts of the isthmic-cervical leiomyoma, from the ureter, urinary bladder and rectum.
The rectovaginal space was entered by incising the peritoneum at the bottom of the pouch of Dougles, and the posterior vaginal wall from the perirectal fascia that covers the rectum was dissected(3).
The next space that was significantly enlarged was the paravesical space. The posterior wall of the urinary bladder was identified and dissected bit by bit from the isthmic-cervical tumor.
We dissected the right and left parametria, singling out the ureters and preserving them.
At this level, after the pelvic inspection and palpation done intraoperatively, we ascertained that the giant isthmic-cervical formation was also extended towards the upper third of the vagina, concealing the cervicovaginal junction.
The total en bloc hysterectomy was performed, and in order to find the cervicovaginal junction, a finger was inserted into the vagina, which allowed us to avoid the performing of a partial vaginectomy; the suture of the vaginal stump was done with continuous absorbable suture no. 1; the hemostasis was checked on; a drain was placed in the pouch of Douglas, through which the patient drained in the first 24 hours postoperatively approximately 80 ml of serosanguinous fluid; the tube was suppressed on the third day after surgery, the evolution of the patient being favorable(4).
Since the tumor was large and very deep within the pelvis, with a difficult approach, the surgery lasted longer than usual, but the postoperative evolution and recovery were favorable.
The uterine leiomyoma affects most frequently women over 35 years of age. While most women with fibroids are asymptomatic, the size and location of these benign tumors varies – they can grow very large, producing significant discomfort(4).
A large isthmic-cervical fibromatous nodule enclosed within the pelvis can cause complications, from urinary and rectal symptoms, ureterovaginal fistula to intraoperative morbidities, such as ureteral lesions, lesioning of the urinary bladder, lesioning of the rectum/sigmoid, vascular incidents, and severe postoperative anemia(5).
The optimal management of the large fibroids developing isthmic-cervically has not been completely established(5,6).
Different types of management have been proposed – surgical, medical and on hold, depending on the symptoms of the patient, the associated medical comorbidities, and the wish for fertility(6).
The use of GnRH agonists or the preoperative embolization of the uterine arteries can be taken into consideration before opting for the radical definitive hysterectomy(7).
Still, the time needed until the treatment becomes efficient and possibly jeopardizing the ovarian function must be considered and discussed with the patient.
We did not use the medical therapy in the handling of our case due to the severity of the symptoms, which required immediate surgery.
In less aggravating circumstances, the preoperative placement of a ureteral stent may be considered, to reduce the risk of intraoperative ureteral lesions(5).
The abdominopelvic CT with contrast or the MRI represents the most precise type of imagery for the mapping, diagnostic and characterization of leiomyomas. They must be required after the ultrasound examination, especially to identify and localize isthmic-cervical fibroids(8).
Large isthmic-cervical fibroids are a unique challenge for the gynecology surgeon, since they distort and change significantly the pelvic anatomy by occupying the pelvis and the upper third of the vagina, the surgeon having reduced access to the retroperitoneal space. The reduced visualization of the pelvic surgical landmarks increases the risk of intraoperative hemorrhage and ureteral lesions.
It is advisable for the gynecology surgeon to be familiarized with the retroperitoneal and pelvic anatomy and to be prepared for radical pelvic surgery(6).
Conclusions
Gynecologists need to be aware of the intraoperative complications associated with the surgical removal of a giant isthmic-cervical fibroma.
The gynecologist together with the general surgeon and the urologist which were part of the surgical team proved themselves to be competent, and they had high manuality and surgical ability in the radical pelvic dissection.
The radical pelvic dissection at the time of the total hysterectomy is necessary in all cases of giant isthmic-cervical tumors to minimize the risk of intraoperative complications.
We have attempted and, at the same time, succeeded in minimizing the intraoperative risks for the presented case, the removal of a giant isthmic-cervical tumor.
Corresponding author:
Diana Popovici
E-mail: dianapopovici1964@yahoo.com
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
- Lee DW, Gibson TB, Carls GS, Ozminkowski RJ, Wang S, Stewart EA. Uterine fibroid treatment patterns in a population of insured women. Fertil Steril. 2009;91(2):566-74.
- Tiltman AJ. Leiomyomas of the uterine cervix: A study of frequency. Int J Gynecol Pathol. 1998;17(3):231-4.
- González Calzada GJ. Miomatosis ítsmicocervical como problema quirúrgico [Isthmic-cervical myomatosis as a surgical problem]. Ginecol Obstet Mex. 1986;54:176-180.
- Wallach EE, Vlahos NF. Uterine myomas: An overview of development, clinical features, and management. Obstet Gynecol. 2004;104(2):393-406.
- Basnet N, Banerjee B, Badani U, et al. An unusual presentation of huge cervical fibroid. Kathmandu Univ Med J (KUMJ). 2005;3(2):173-4.
- Suneja A, Taneja A, Guleria K, Yadav P, Agarwal N. Incarcerated procidentia due to cervical fibroid: An unusual presentation. Aust N Z J Obstet Gynaecol. 2003;43(3):252-3.
- Guzin K, Sezginsoy S, Tuncay YA, Naki M, Kanadikirik F. The management of an unusually sited isthmicocervical leiomyoma and a huge prolapsed pedunculated submucous leiomyoma. Gynecol Surg. 2005;2(1):35-8.
- Vitiello D, McCarthy S. Diagnostic imaging of myomas. Obstet Gynecol Clin North Am. 2006;33(1):85-95.

March-May 2024 Calendar
March-May 2024 Calendar...
The Bartholin gland cyst – actual therapeutic approaches and case report
Valentin Burcan, Cristiana-Elena Durdu, Tiberiu Augustin Georgescu, Roxana-Elena Bohîlţea
The Bartholin’s glands, initially described in 1677 by the Danish anatomist Casper Bartholin, also known as the greater vestibular glands, encompass a pair of anatomical structures located in proximity to the vaginal ent...
Ultrasound-based differential diagnosis of fetal abdominal wall defects in early pregnancy
Mircea Octavian Poenaru, Delia-Maria Bogheanu, Romina-Marina Sima, Liana Pleș
Fetal abdominal wall defects (AWDs) encompass a wide range of congenital anomalies that involve the incomplete closure or disruption of the abdominal wall during the embryonic development. ...
The Bartholin gland cyst – actual therapeutic approaches and case report
Valentin Burcan, Cristiana-Elena Durdu, Tiberiu Augustin Georgescu, Roxana-Elena Bohîlţea
The Bartholin’s glands, initially described in 1677 by the Danish anatomist Casper Bartholin, also known as the greater vestibular glands, encompass a pair of anatomical structures located in proximity to the vaginal ent...
A rare case of complete hydatidiform mole with prolonged evolution – clinical case
Mona Akad, Răzvan Socolov, Raluca Bălan, Diana Popovici, Eduard Crauciuc, Roxana Covali, Fawzy Akad, Tudor Buţureanu, Ana-Maria Apetrei, Alina Andriucă, Demetra Socolov
Mola hidatiformă, cunoscută drept sarcină molară, reprezintă o boală gestaţională trofoblastică cu punct de plecare placentar şi c...