Indexul de şoc – metodă de apreciere a hemoragiei post-partum
The shock index – a method to appreciate the postpartum haemorrhage
Abstract
The shock index (SI) is calculated by dividing the HR (heart rate) and SBP (systolic blood pressure), and it was proposed in order to identify the patients who needed blood transfusion. We performed a literature review in order to assess the predictive value of SI in women with postpartum hemorrhage (PPH). We searched PubMed, Medline and medical texts pertaining to SI in PPH up to January 2019. We found two studies, including a number of 1191 patients. For the non-pregnant population, the value was set under 0.6, for the pregnant women between 0.75 and 0.83, and in the postpartum patients, between 0.52 and 0.89. The alarm value of the SI was set as 0.9, while critical situations can be announced by values of 1.7. The SI is a good strategy to act earlier for women who are at high risk of adverse outcome.Keywords
postpartum haemorrhageshock indexblood lossRezumat
Indexul de şoc este calculat împărţind frecvenţa cardiacă la tensiunea arterială sistolică şi a fost propus pentru identificarea pacienţilor care necesită transfuzie sangvină. Am realizat o revizuire a literaturii pentru a evalua valoarea predictivă a indexului de şoc la femeile cu hemoragie post-partum. Am căutat în bazele de date PubMed, Medline şi în publicaţii medicale articole referitoare la indexul de şoc în hemoragia post-partum până în ianuarie 2019. Am găsit două studii, care includeau un număr de 1191 de paciente. Pentru pacientele care nu erau gravide, valoarea indexului de şoc a fost sub 0,6, pentru gravide – între 0,75 şi 0,83, iar în post-partum – 0,52-0,89. Valoarea de alarmă a fost stabilită la 0,9, iar situaţiile critice apar la valori de 1,7. Indexul de şoc reprezintă o strategie bună pentru a acţiona în timp util în cazul femeilor cu risc crescut de a evolua nefavorabil.Cuvinte Cheie
hemoragie post-partumindexul de şocpierdere de sângeIntroduction
Postpartum haemorrhage (PPH) is a medical and obstetrical emergency and it represents one of the top causes of maternal morbidity. Globally, 29.3% of maternal deaths and 26.7% of severe adverse maternal outcomes are related to haemorrhage(1).
The most recent definition of PPH was given by the American College of Obstetricians and Gynecologists, in 2017, representing the cumulative blood loss over 1000 mL, regardless of route of delivery and signs or symptoms of hypovolemia(1).
In healthy pregnant and postpartum women, compensatory mechanisms developed in pregnancy (increase in cardiac output, heart rate and blood pressure) that prevent changes in vital signs until a large amount of blood is lost (usually >1000 mL)(1). In this case, we need a new method to appreciate the blood loss before the symptoms of hypovolemia appear, and this method is the shock index (SI).
The SI is calculated dividing the HR (heart rate) to SBP (systolic blood pressure), and it has been proposed as an earlier marker of compromise. Initially, it was mainly used for non-specific shock, trauma or sepsis in non-pregnant populations(2), but now it is used in evaluating the postpartum bleeding evaluation.
Method
We conducted a literature review study in order to assess the predictive value of SI in women with postpartum haemorrhage (PPH) and we searched PubMed, Medline and medical texts pertaining to SI in PPH up to January 2019.
Results
We found two studies, including 1191 patients with PPH and 21853 non-pregnant patients. The shock index is used mostly to identify the patients who need blood transfusion.
Discussion and conclusions
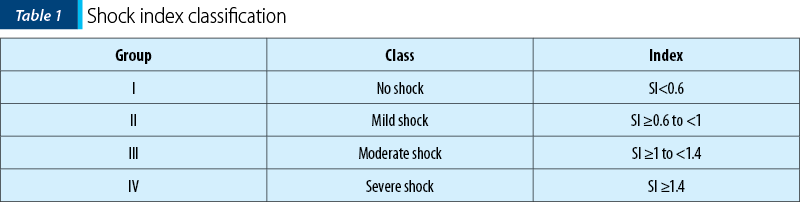
Mutschler et al. included 21,853 non-pregnant patients in his study and concluded that the SI was divided into four groups: group I (SI<0.6), group II (SI ≥0.6 to <1), group III (SI ≥1 to <1.4) and group IV (SI ≥1.4) – Table 1. The increasing transfusion requirement varies from one blood unit in group 1 to 21.4 in group IV(3).
For pregnant women, these values are different due to the cardiovascular modifications mentioned before, and the values of SI increase simultaneously with the weeks of gestation: from 0.756±0.127 at 12 weeks or fewer to 0.831±0.144 at 28-32 weeks(4). Other studies show that the normal ranges were situated between 0.7 and 0.9(5).
Further studies reveal that for all the non-pathological pregnancies, during the entire pregnancy, the SI should be 0.75-0.83; in the postpartum period the SI should be between 0.52 and 0.89, and it can also be influenced by the epidural anesthesia or the use of ergometrine. Up to 20% of the normal pregnancies can present a SI over 0.9, without any pathological implications(1).
A study that involved 958 women with PPH revealed that SI was an important predictive factor of morbidity and death, the value of 0.9 being the inferior limit of SI for patients who needed intervention in the postpartum period. From 958 patients involved, 60 patients (6.3%) had a SI under 0.9(1). Another study that involved 233 patients with PPH revealed a significant value of the SI between 0.8 and 1.15. A number of 202 women (86.7%) had a SI level over 0.7, and 137 (58.8%) had a SI level over 0.9. The women with SI level under 0.9 were not admitted in the intensive care unit. A SI level over 1.7 represents a severe situation which requires major interventions(2).
In conclusion, SI is a good strategy to act earlier in women who are at high risk for adverse outcome. As the two studies showed, the SI value of 0.9 should be the alarm value. Furthermore, SI can be easily calculated, and it can be applied even in not so well-resourced medical centers.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Borovac-Pinheiro A, Pacagnella RC, Cecatti JG et al. Postpartum hemorrhage: new insights for definition and diagnosis. Am J Obstet Gynecol. 2018;219(2):162–8.
- Nathan HL, El Ayadi A, Hezelgrave NL, Seed P, Butrick E, Miller S, Briley A, Bewley S, Shennan AH. Shock index: an effective predictor of outcome in postpartum haemorrhage? BJOG. 2015;122(2):268-75.
- Mutschler M, Nienaber U, Münzberg M et al. The Shock Index revisited – a fast guide to transfusion requirement? A retrospective analysis on 21.853 patients derived from the Trauma Register DGU. Crit Care. 2013; 17(4):R172.
- Borovac‐Pinheiro A, Pacagnella RC, Morais SS, et al. Standard reference values for the shock index during pregnancy. Int J Gynaecol Obstet. 2016; 135(1):11-5.
- Nathan HL, Cottam K, Hezelgrave NL et al. Determination of normal ranges of Shock Index and other haemodynamic variables in the Immediate postpartum period: a cohort study. PLoS One. 2016; 11(12):e0168535.

Diabetul gestaţional
Daniela Stan, Mihai Mitran
Diabetul gestaţional afectează 3-9% din sarcini, implicaţiile acestuia asupra mamei şi copilului fiind uriaşe, întrucât creşte riscul complicaţiilor perinatale. În acelaşi timp, prezice complicaţii metabolice tardive, cronice, atât la mamă, cât şi la copil, iar uneori efectele sale se fac resimţite pe parcurs...
Anomaliile cromozomiale şi defectele orodentare – diagnosticul prenatal
Andrei Kozma, Viorica Radoi, Radu Ursu, Dona Andreea Iordan-Dumitru, L.C. Bohîlțea
Tulburările genetice pot fi clasificate ca moştenire genetică unică, moştenire multifactorială, anomalii cromozomiale sau moştenire mitocondrială. Fiecare defect congenital structural din organism reprezintă o eroare în...
Rolul infecţiilor orale în naşterea prematură
Alexandru Iliescu, Paula Perlea, Kamel Earar, Irina-Maria Gheorghiu
Prematuritatea şi greutatea scăzută la naştere sunt unele din complicaţiile frecvente ale sarcinilor. Infecţiile orale, în special bolile parodontale, reprezintă un factor de risc. Infecţia anaerobă Gram-negativă din spa...
IgG alergen-specifice materne pot proteja copilul împotriva sensibilizării alergice. Review al literaturii
Ileana-Maria Conea, Liana Pleș, Cristian Balalau, Adina-Teodora Corbu
Analiza răspunsurilor IgE specifice alergenului în cohortele de naştere cu alergeni micromatrice a furnizat informaţii detaliate privind evoluţia răspunsurilor IgE-specifice la copii. Sunt necesare...
Infecţia cu Mycoplasma în determinismul naşterii premature – review din literatură
Anca Rîcu, Cristina Moisei, Romina-Marina Sima, Cristian Balalau, Liana Pleș
Naşterea prematură este responsabilă pentru majoritatea cazurilor de deces neonatal. În cele mai multe dintre aceste cazuri, cauzele nu au fost stabilite, deşi mai mulţi factori de risc sunt incriminaţi. Mycoplasma homin...