Infecţiile postoperatorii în obstetrică
Surgical site infections in obstetrics
Abstract
Reaching up to 3% of maternal mortality, alongside postpartum hemorrhage, the infection in obstetrics is the second-mentioned contributor to maternal mortality. In order to review the literature on the surgical site infections in obstetrics, including risk factors, diagnosis and management, published electronic databases such as PubMed and Medline were reviewed and searched, from the 1st of January 2015 to the 30th of April 2020, using keywords such as surgical site infection, infection prevention in obstetrics, risk factors, caesarean section, along with medical texts pertaining to surgical site infections in obstetrics. From a total of 666 eligible studies, 22 papers were selected as relevant to the subject and included in our final review, 7 trial studies, totaling 48,262 patients, and 15 clinical guidelines and systematic reviews incorporating risk factors, methods of diagnosis, prevention and treatment. As caesarean section delivery rates are unceasingly increasing around the world, complications such as surgical site infections continue to concern the obstetricians and healthcare professionals.Keywords
surgical site infectioninfection prevention in obstetricsrisk factorscaesarean sectionRezumat
Alături de hemoragia postpartum, infecţiile în obstetrică sunt amintite ca fiind a doua cauză a mortalităţii materne, atingând un procentaj de 3% din totalul cazurilor menţionate. Pentru o bună analiză a literaturii de specialitate privind infecţiile postoperatorii în obstetrică, incluzând factorii de risc, diagnosticul şi tratamentul, au fost utilizate baze de date electronice precum PubMed şi Medline, din perioada 1 ianuarie 2015 – 30 aprilie 2020, fiind folosite cuvinte-cheie precum infecţii postoperatorii, prevenirea infecţiilor în obstetrică, factori de risc, operaţie cezariană, alături de texte medicale care fac referire la infecţiile postoperatorii în obstetrică. Dintr-un total de 666 de studii eligibile, 22 de lucrări au fost selectate ca fiind relevante pentru subiectul dezbătut şi incluse în studiul nostru final, 7 studii clinice, totalizând 48.262 de pacienţi, şi 15 ghiduri clinice care au cuprins factori de risc, metode de diagnostic, prevenţie şi tratament. Din moment ce la nivel global rata naşterilor prin operaţie cezariană se află într-o continuă creştere, complicaţiile precum infecţiile postoperatorii continuă să preocupe atât obstetricienii, cât şi profesioniştii din domeniul medical.Cuvinte Cheie
infecţii postoperatoriiprevenţia infecţiilor în obstetricăfactori de riscoperaţie cezarianăIntroduction
In the past decades, caesarean delivery rates have increased dramatically(1) in defiance of paucity of data regarding the increasing percentages of obstetric emergencies(2), in some countries reaching up to 50% of the total deliveries(3). Caesarean section is the most important surgical obstetrical procedure with complications that consist of postpartum hemorrhage, endometritis, thromboembolic events or incision infections(3). In 2013, the European Health for All database recorded in Romania a caesarean section delivery rate of 40.1%, one of the highest in the world(4).
Definition
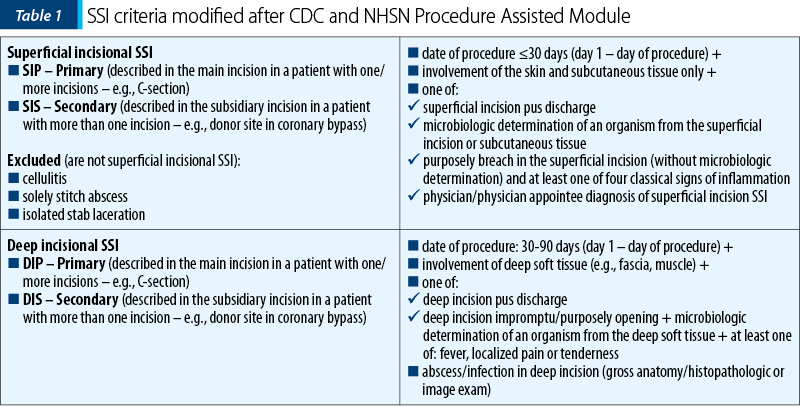
A surgical site infection (abbreviated as SSI) is described as a condition that alters the skin incision or the tissues underneath it, which can evolve up to thirty days after the surgical procedure(5). According to the Procedure Assisted Module, published in January 2020 by the Centers for Disease Control and Prevention (CDC) and the National Healthcare Safety Network (NHSN), SSIs represent a considerable determinant of morbidness, extended treatment and hospitalization, with criteria exemplified in Table 1(5).
Microbiology
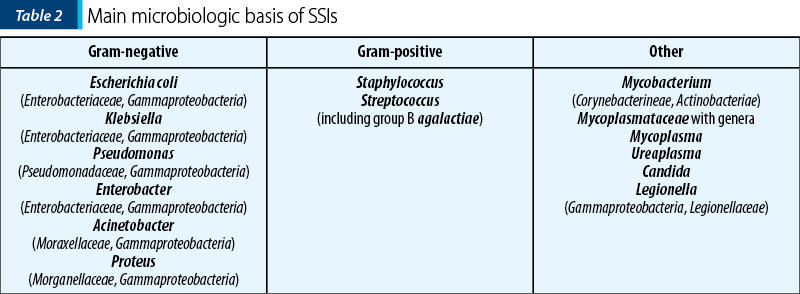
Up to 20% of cases of SSIs had a positive microbiologic determination of Staphylococcus aureus, followed by Enterococcus species and Escherichia coli, both the skin and the vagina being appointed as the dual source of the bacterium, with high rates of polymicrobial infections consisting of both aerobic and anaerobic organisms (Table 2)(6).
Risk factors
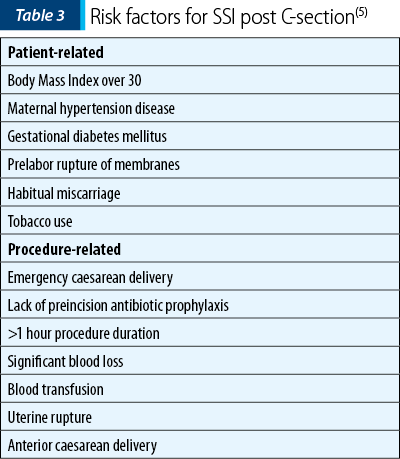
Through a retrospective population-based cohort study, in an article published in January 2017, Krieger et al.(7) described the main risk factors that lead to SSI post-caesarean delivery, as indicated in Table 3. Patients who acquired SSIs had a history of habitual miscarriage or previous caesarean section delivery, they were of a slightly older age and with a higher parity rate. It is noted that procedure-related risk factors included emergency caesarean delivery, lack of preincision antibiotic prophylaxis, procedure duration more than one hour or complications such as significant blood loss with subsequent blood transfusion, uterine rupture or caesarean hysterectomy(7).
Management
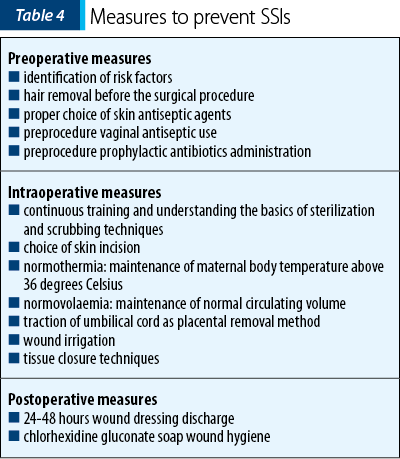
To reduce the incidence of SSIs post-caesarean delivery, preventive care and measures are taken in order to determine the risk factors and to identify the proper pre-/intra- and postoperative procedures that can lead to a higher success rate, as indicated in Table 4.
Preoperative measures
One of the most frequently mentioned risk factors is gestational diabetes in pregnant women, which is associated with a higher rate of surgical site complications post-caesarean delivery(8). As indicated in a study conducted by Hu et al. and published in July 2016, there are physiologic elements involved in the dysfunction of epidermal keratinocytes caused by a rich glucose climate, therefore an improvement in the patient’s glycemic control may lead to a better outcome, with auxiliary benefits of a normal glycemic range that is lessening the risk of hypoglycemia in the neonates and ketoacidosis of the mother(9).
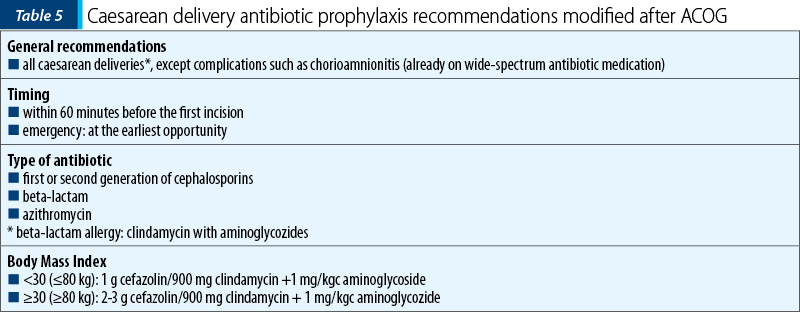
According to the Global guidelines on the prevention of surgical site infections, hair removal before the surgical procedure does not considerably influence the rates of SSIs(10), but using razors, that can cause microscopic skin breach, instead of clippers, may cause more harm than good. Microorganisms found on the skin and their pathogenic aspect are seen as the main determinant involved in SSIs. To address this topic, a randomized controlled trial comparing skin antiseptic agents use such as chlorhexidine-alcohol and iodine-alcohol in caesarean delivery was conducted by Tuuli et al. at the University of South Florida and published in February 2016. From 1147 patients, 4% of the chlorhexidine-alcohol category had SSIs complications versus 7.3% in the iodine-alcohol category (relative risk 0.55; 95% confidence interval; 0.34 to 0.90; p=0.02)(11). In a Cochrane review updated in April 2020, it was noted that the use of vaginal antiseptic such as povidone-iodine or chlorhexidine anterior to caesarean delivery may be considered to reduce the risk of SSIs (RR 0.62; 95% CI; 0.50 to 0.77; 18 trials, 6385 women)(12). To reduce the incidence of SSIs, the American College of Obstetricians and Gynecologists (ACOG), in its committee opinion from September 2018, proposed the prophylactic antibiotic administration as a routine measure for all patients who have to go through a caesarean delivery. Recommendations were made for the use of first-generation cephalosporins or their alternative, clindamycin with aminoglycosides, in patients with beta-lactam allergy, as shown in Table 5(13).
Intraoperative measures
The continuous training and understanding the basics of sterilization and scrubbing techniques play a pivotal role in diminishing the prevalence of SSIs(14). Addressing the issue of choice of skin incision, compared to the Pfannenstiel incision, the Joel-Cohen incision reported up to 65% less cases of hyperyrexia complications post-caesarean delivery (RR 0.35; 95% CI; 0.14-0.87; p=0.023), with no significant differences in SSIs(14). Intraoperative hypothermia enhances the risk of surgical site infections and prolongs the period of hospitalization, therefore the World Health Organization guidelines recommend maintaining the intraoperative maternal body temperature above 36 degrees Celsius(15). Equally as important as maintaining an intraoperative body temperature above 36 degrees Celsius is the maintenance of normovolaemia. In accordance with the new World Health Organization recommendations on intraoperative and postoperative measures for surgical site infection prevention, a diminished incidence of surgical site infections was reported for intraprocedure goal-directed fluid therapy (GDFT) versus an average intraprocedure fluid management (OR 0.56; 95% CI; 0.35-0.88)(15). A higher rate of endometritis as a complication of post-caesarean delivery has been reported in manual removal as placental removal method versus intraoperative controlled traction of umbilical cord (RR 1.64; 95% CI; 1.42-1.90)(15). Wound irrigation does not occupy a statistically important role in the management of post-caesarean delivery surgical site infections. The irrigation of the tissues found above the fascial area with povidone-iodine solution did not reduce the incidence of SSIs post-caesarean delivery, as shown in a substantial randomized controlled trial published in 2016 by K. Mahomed et al. (RR 0.97; 95% CI; 0.78 to 1.21)(16). The same result was obtained evaluating the use of intraprocedure saline irrigation that led to maternal nausea, but did not influence the outcome of surgical site infections or endometritis (RR 1.68; 95% CI; 1.36 to 2)(17). Updated in September 2019, the NICE clinical guidelines on caesarean section encourage different tissue closure techniques in order to prevent SSIs(18). Multiple layer tissue closure is not recommended for all women undergoing caesarean delivery; ergo, for patients with an increased Body Mass Index or a subcutaneous tissue thickness over 2 cm, two-layer closure is encouraged(18). Wound breach or skin infections have been reported with a higher incidence in obese women undergoing staples closure versus subcuticular suture as indicated in a retrospective cohort study that included 1147 women (RR 1.78; 95% CI; 1.27 to 2.49)(19).
Postoperative measures
The periodic checkup of the caesarean delivery wound is fundamental to assess the postprocedure progression in order to identify any signs of inflammation or infection. Although it is recommended that all wound bandage be removed between 24 and 48 hours postprocedure(20), a randomized controlled trial conducted by Peleg et al. in 2016 revealed that there is no difference regarding the rate of complications between bandage discharge at 6 hours (n=160) versus 24 hours (n=160) postprocedure, while the rate of satisfaction in women pertaining to the first category has increased (OR 2.35; 95% CI; 1.46-3.79)(21).
Management
Although the procedures required to prevent surgical site infections play a crucial role, measures meant to raise the rate of success, such as the right choice of antibiotics or the type of wound dressing (as indicated in Table 6), are important in the management and treatment of complications.
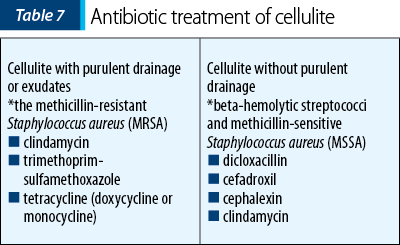
There are different types of wound bandage materials available, from foam, beads, hydrocolloids, plaster with chlorhexidine to povidone iodine and mercury chloride solutions, that can be used in order to isolate and treat the wound site(22). The “wet-to-dry” technique consists of securing the wound with a moist plaster followed by a dry bandage coating. In some circumstances, cellulitis, a complication that affects the dermis and the subcutaneous tissue, can be treated with antibiotics, without demanding incision and drainage. Two types of cellulitis are taken into consideration: with purulent drainage or exudates, and the empiric treatment covers the methicillin-resistant Staphylococcus aureus (MRSA) with options that consist of clindamycin, trimethoprim-sulfamethoxazole and tetracycline (doxycycline or monocycline); and cellulite without purulent drainage, with therapy such as dicloxacillin, cefadroxil, cephalexin and clindamycin taken into consideration to cover beta-hemolytic streptococci and methicillin-sensitive Staphylococcus aureus (MSSA), as indicated in Table 7. Incision and drainage are required when hematoma, abscess or exudates complicate the wound(22).
Conclusions
Pregnancy plays an important role in a woman’s life and healthcare providers around the world are constantly searching for new methods for the diagnosis and treatment of pregnancy-related complications in pursuance of a safe parturiency journey and childbirth process. Understanding the importance of this issue, the current Procedure Assisted Module, published in January 2020 by the Centers for Disease Control and Prevention and the National Healthcare Safety Network, precisely stipulates the diagnosis criteria for surgical site infections, and identifying the microbiological basis of the infection contributes greatly to the end result. As prevention is better than cure, conjointly with proper identification of risk factors, pre-/intra- and postoperative procedures are needed to be implemented. With accessible treatment options, all cohesive efforts are made for a better outcome for the new mother and her child.
Bibliografie
-
Fuhler GM. The immune system and microbiome in pregnancy. Best Pract Res Clin Gastroenterol. 2020;44-5:101671.
-
Mamo T, Abebe TW, Chichiabellu TY, Anjulo AA. Risk factors for surgical site infections in obstetrics: a retrospective study in an Ethiopian referral hospital. Patient Saf Surg. 2017;11:24.
-
Mulchandani R, Power HS, Cavallaro FL. The influence of individual provider characteristics and attitudes on caesarean section decision-making: a global review. J Obstet Gynaecol. 2020;40(1):1-9.
-
European Health for All Database (HFA-DB). WHO Regional Office for Europe; 2015, http://data.euro.who.int/hfadb
-
National Healthcare Safety Network (NHSN). Patient Safety Component Manual. Jan 2020. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/pcsmanual_current.pdf.
-
Andersen BM. Prevention of postoperative wound infections. Prevention and Control of Infections in Hospitals. 2018;377–437.
-
Krieger Y, Walfisch A, Sheiner E. Surgical site infection following cesarean deliveries: trends and risk factors. J Matern Fetal Neonatal Med. 2017;30(1):8-12.
-
Kawakita T, Landy HJ. Surgical site infections after cesarean delivery: epidemiology, prevention and treatment. Matern Health Neonatol Perinatol. 2017;3:12.
-
Hu S C-S, Lan C-C E. High-glucose environment disturbs the physiologic functions of keratinocytes: Focusing on diabetic wound healing. J Dermatol Sci. 2016;84(2):121-7.
-
https://www.who.int/gpsc/ssi-guidelines/en/
-
Tuuli MG, Liu J, Stout MJ, Martin S, Cahill AG, Odibo AO, Colditz GA, Macones GA. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647-55.
-
Haas DM, Morgan S, Contreras K, Kimball S. Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections. Cochrane Database of Systematic Reviews 2020;4:CD007892.
-
ACOG Practice Bulletin. Prophylactic antibiotics in labor and delivery. 2018;9; https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2018/09/use-of-prophylactic-antibiotics-in-labor-and-delivery
-
Zuarez-Easton S, Zafran N, Garmi G, Salim R. Postcesarean wound infection: prevalence, impact, prevention, and management challenges. Int J Womens Health. 2017;9:81-8.
-
Allegranzi A, Zayed B, Bischoff P, Zeynep Kubilay N, de Jonge S, de Vries F SM, Gans S, Wallert ED, Wu X, Abbas M, Boermeester MA, Patchen Dellinger E, Egger M, Gastmeier P, Guirao X, Ren J, Pittet D, Solomkin JS. WHO Guidelines Development Group. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Inf Dis. 2016;16(12):e288-e303.
-
Mahomed K, Ibiebele I, Buchanan J. The Betadine trial – antiseptic wound irrigation prior to skin closure at caesarean section to prevent surgical site infection: a randomised controlled trial. Aust NZ J Obstet Gynaecol. 2016;56:301-6.
-
Eke AC, Shukr GH, Chaalan TT, Nashif SK, Eleje GU. Intra-abdominal saline irrigation at cesarean section: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2016;29:1588-94.
-
Clinical Guideline No. 132. Caesarean Section. NICE, UK, 2011, https://www.nice.org.uk/guidance/cg132/resources/caesarean-section-pdf-35109507009733
-
Zaki MN, Truong M, Pyra M, Kominiarek MA, Irwin T. Wound complications in obese women after cesarean: a comparison of staples versus subcuticular suture. J Perinatol. 2016;36:819-22.
-
Toon CD, Sinha S, Davidson BR, Gurusamy KS. Early versus delayed post-operative bathing or showering to prevent wound complications. Cochrane Database Syst Rev. 2015;2015(7):CD010075.
-
Peleg D, Eberstark E, Warsof SL, Cohen N, Ben Shachar I. Early wound dressing removal after scheduled cesarean delivery: a randomized controlled trial. Am J Obstet Gynecol. 2016;215(3):388.e1-5.
-
Martin EK, Beckmann MM, Barnsbee LN, Halton KA, Merollini K, Graves N. Best practice perioperative strategies and surgical techniques for preventing caesarean section surgical site infections: A systematic review of reviews and meta-analyses. BJOG. 2018;125(8):956-64.

September – December 2020 Calendar
...
Restaurarea directă în masă („bulk fill”) cu răşini compozite în sarcină – prezentare de caz
Irina-Maria Gheorghiu, Loredana Mitran, Mihai Mitran, Alexandru Iliescu, Sânziana Scărlătescu
In pregnant women, all dental treatments, which are absolutely required, are strictly related to the fact that the female patient is in a special physiological condition, which reflects on the physica...
Complicaţiile perinatale şi neonatale la pacientele cu răspuns ovarian scăzut în sarcinile obţinute prin proceduri de reproducere umană asistată
Cătălin Ioan Bosoancă, Simona Vlădăreanu, Alina-Gabriela Marin, Radu Vlădăreanu
In vitro fertilization (IVF) technologies with a controlled ovarian hyperstimulation approach have classified patients into three ...
Hemangiom vertebral agresiv care determină afectare neurologică severă în al treilea trimestru de sarcină – prezentare de caz
Oana Mihaela Teodor, Alexandru Baroş, Dan Teleanu, Monica-Mihaela Cîrstoiu
Hemangiomas are benign vascular tumors characterized by endothelial cell proliferation, most commonly affecting the soft tissues, but they can also be identified in bones, including the vertebral bo...
Tehnici de sutură în operaţia cezariană
Ducu Ioniţă, Natalia Ţurcan, Roxana-Elena Bohîlţea
Operaţia cezariană este una dintre cele mai frecvente intervenţii chirurgicale abdominale ce nu beneficiază de o tehnică standard. ...