Miomectomia laparoscopică la pacientele de vârstă fertilă
Laparoscopic myomectomy in women of reproductive age
Abstract
Uterine leiomyoma represents the most common benign tumour in women of reproductive age, with a prevalence of 20-50%. Most women are asymptomatic, but 30% of them report mettrorhagia, pelvic pain, dyspareunia, urinary and bowel symptoms or infertility. Symptomatic fibromas and the desire for childbearing are the most common indications for myomectomy. Some patients are candidates for laparoscopic myomectomy.Keywords
myomectomyuterine fibromaslaparoscopic myomectomyRezumat
Mioamele uterine reprezintă cea mai frecventă patologie ginecologică benignă la pacientele în premenopauză, având o prevalenţă de 20-50%. Majoritatea pacientelor sunt asimptomatice, dar 30% dintre acestea se pot prezenta pentru metroragii, pelvialgii, infertilitate, dispareunie, simptomatologie urinară iritativă sau simptomatologie digestivă. Fibroamele uterine simptomatice la pacientele tinere care optează pentru prezervarea fertilităţii reprezintă principala indicaţie pentru miomectomie. Unele paciente vor fi candidate pentru miomectomie laparoscopică.Cuvinte Cheie
miomectomiefibroame uterinemiomectomie laparoscopicăIntroduction
Uterine leiomyoma represents the most common benign tumour in women of reproductive age, with a prevalence cited in the literature of 20-50%(1). Most patients are asymptomatic, but 30% of patients with fibromatous uterus may develop metrorrhagia, pelvic pain, dyspareunia, low urinary symptomatology, digestive symptoms and infertility.
Multiple therapeutic options are proposed for the treatment of uterine fibroids, which are divided into surgical and non-surgical methods. Choosing the optimal surgical method depends on several factors, some patients being candidates for laparoscopic surgery. The first laparoscopic excision of subserous fibroids was described in 1979(2), and it was practiced for intramural myomas in 1990(3-6).
Hysterectomies are usually performed for symptomatic uterine fibroids(7,8). Minimally invasive approach has taken the place of classical myomectomies practiced for decades as treatment of symptomatic uterine fibroids(9).
Patient selection/indications
The primary indication for laparoscopic myomectomy is the excision of subserous and intramural fibroids. During laparoscopy, if submucosal myomas are present, the concomitant hysteroscopy can be performed.
The inclusion criteria for laparoscopic treatment is important in order to ensure a successful intervention. This is defined by minimal postoperative complications and the lack of laparotomy conversion. Currently, literature data are insufficient and the success depends mostly on the gynecologist’s learning curve. The main features that influence the way of approaching the myomas by laparotomy or laparoscopy are the location, the relationship with pelvic/abdominal important structures, the depth of myometrium penetration, the size and the number of fibroids. Sizzi et al. published the results of the largest prospective study which included 2050 patients with laparoscopic myomectomy from January 1996 to December 2004. The authors report that the most important risk factors for major complications, such as blood transfusions and the rate of failure of surgery, are the number of fibroids (more than three), intraligamentar localization of the tumors, and especially the fibroma size (over 5 cm). The intramural localization was associated with an increase of minor complications(10).
Myomectomy
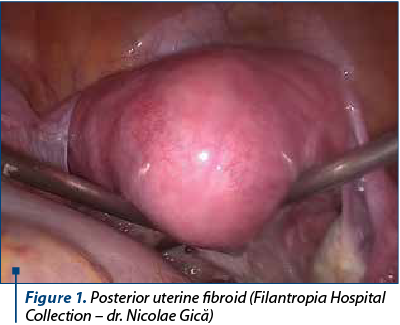
Using a manipulator facilitates the myomas excision and the suturing of the uterus by mobilizing the uterus according to the tumor location (Figure 1).
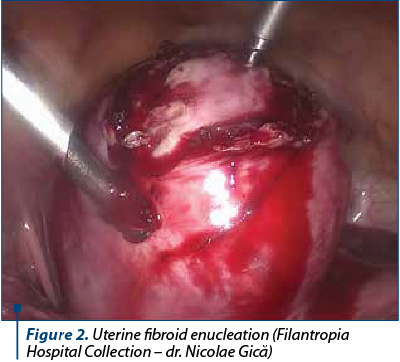
One of the techniques used to reduce bleeding is the injection of the subcapsular space with dilute vasopressin(11), but there are several important complications reported, such as pulmonary edema, severe hypotension and bradycardia(12). The horizontal or vertical incision can be made using a monopolar (hook or scissor) in order to reduce bleeding(13,14). After highlighting the myoma pseudocapsule, the myoma can be easily enucleated, especially if the avascular cleavage plan is found (Figure 2).
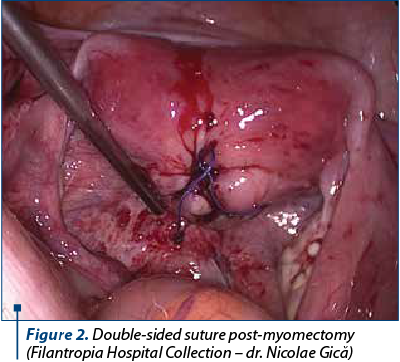
The suture of the uterus is practiced in one or more layers, and it is of particular importance for scar resistance during a future pregnancy and labor(12,14). Slow absorbable material will be used (Figure 3).
The specimen can be extracted using mechanical or electrical morcellator. Since 2014, the Food and Drug Administration (FDA) has discouraged the use of morcellation to extract the specimens. The morcellation is recommended using an “endo-bag” to reduce the risk of intraabdominal dissemination of tumor tissue (undiagnosed preoperatively) if laparoscopic myomectomy/hysterectomy is the most appropriate therapeutic method.
Laparoscopy or laparotomy?
The laparoscopic myomectomy offers the advantages of minimally invasive surgery. Since Semm performed the first laparoscopic myomectomy(2), multiple studies and articles have been published regarding the safety and feasibility of the technique. Retrospective studies have shown that laparoscopic myomectomy is associated with lower blood loss, reduced morbidity and hospitalization period(15,16).
In a double-blind study, Holzer et al. compared pain scores within 72 hours postoperatively in patients who underwent laparoscopic and classical myomectomy, and demonstrated that laparoscopic myomectomy is associated with a significantly reduced pain than classic myomectomy(17).
Postoperative peritoneal adhesions are reported in 93% of the post-laparotomy cases(18), and the consequences may be unfavorable for the prognosis of women fertility, with a negative impact in patients who underwent myomectomy for infertility.
Kubinova et al. performed a “second-look” study with a total of 96 patients who underwent laparoscopic and classical myomectomy. They reported an intraabdominal adherence rate of 96.65% post-classical myomectomy and 71.43% post-laparoscopic myomectomy. The adhesion density was much higher after laparotomy, and the incidence of adnexal adhesions de novo after classic myomectomy was 89.29%, in contrast to 10.6% after laparoscopic myomectomy, an important factor which may compromise fertility(19).
In conclusion, although laparoscopic myomectomy cannot completely prevent the formation of adhesions, it can at least greatly reduce their post-surgery incidence.
The involvement of uterine fibroids in infertility etiopathogenesis is controversial. Submucosal uterine fibroids can reduce fertility rates, and their excision can improve the fertility prognosis(20). Subserous fibroids do not influence fertility prognosis, and the impact of intramuscular fibroids on fertility prognosis is still uncertain(21).
The risk of uterine rupture post-myomectomy is an important cause of concern in patients undergoing myomectomy with the purpose to improve the fertility prognosis. Some cases of uterine rupture are reported after both classical myomectomy and laparoscopic methods(22,23,24). The risk factors for uterine rupture include tissue necrosis due to excessive electrocoagulation after haemostasis(25), the formation of hematomas or inappropriate suture of the uterus(26). Therefore, some authors recommend the suture of myometrial defect in several layers(25,27). In a prospective study, Kumakiri et al. concluded that uterine rupture following laparoscopic myomectomy is a rare event during pregnancy, and that vaginal birth can be performed under safe conditions for a particular patient population(27).
Conclusions
Symptomatic uterine fibroids are the main indication for laparoscopic myomectomy and fertility preservation. Laparoscopic myomectomy has numerous advantages than classical myomectomy, such as lower blood loss, reduced hospitalization, low overall morbidity and less postoperative pain. The rate of postoperative adhesions is lower for laparoscopic myomectomy. The vaginal delivery post-laparoscopic myomectomy can be performed under safe conditions.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Novak ER, Woodruff JD. Myoma and other benign tumors of the uterus. In: Gynecologic and Obstetric Pathology. 8th ed. Philadelphia, USA: W.B. Saunders, 1979; pp. 260–78.
- Semm K, Mettler L. Technical progress in pelvic surgery via operative laparoscopy. Am J Obstet Gynecol. 1980; 138:121–7.
- Daniell JF, Gurley LD. Laparoscopic treatment of clinically significant symptomatic uterine fibroids. J Gynecol Surg. 1991; 7:37–9.
- Dubuisson JB, Lecuru F, Foulot H, Mandelbrot L, Aubriot FX, Mouly M. Myomectomy by laparoscopy: A preliminary report of 43 cases. Fertil Steril. 1991; 56:827–30.
- Hasson HM, Rotman C, Rana N, Sistos F, Dmowski WP. Laparoscopic myomectomy. Obstet Gynecol. 1992;80:884–8.
- Nezhat C, Nezhat F, Silfen SL, Schaffer N, Evans D. Laparoscopic myomectomy. Int J Fertil. 1991; 36:275–80.
- Whiteman MK, Hillis SD, Jamieson DJ, et al. Inpatient hysterectomy surveillance in the United States, 2000-2004. Am J Obstet Gynecol. 2008; 198:34.e1.
- Stang A, Merrill R, Kuss O. Hysterectomy in Germany. Dtsch Arztebl Int. 2011; 108:508e514.
- Parker WH. Uterine myomas: management. Fertil Steril. 2007; 88:255e271.
- Sizzi O, Rossetti A, Malzoni M, et al. Italian multicenter study on complications of laparoscopic myomectomy. J Minim Invasive Gynecol. 2007; 14:453.
- Shimanuki H, Takeuchi H, Kitade M, Kikuchi I, Kumakiri J, Kinoshita K. The effect of vasopressin on local and general circulation during laparoscopic surgery. J Minim Invasive Gynecol. 2006; 13:190e194.
- Mattei A, Cioni R, Bargelli G, Scarselli G. Techniques of laparoscopic myomectomy. Reprod BioMed Online. 2011; 23:34e39.
- Agdi M, Tulandi T. Minimally invasive approach for myomectomy. Semin Reprod Med. 2010; 28:228e234.
- Hurst BS, Matthews ML, Marshburn P. Laparoscopic myomectomy for symptomatic uterine myomas. Fertil Steril. 2005; 83:1e23.
- Stringer N, Walker JC, Meyer P. Comparison of 49 laparoscopic myomectomies with 49 open myomectomies. J Am Assoc Gynecol Laparosc. 1997; 4:457e464.
- Marret H, Chevillot M, Giraudeau B. A retrospective multicentre study comparing myomectomy by laparoscopy and laparotomy in current surgical practice. What are the best patient selection criteria? Eur J Obstet Gynecol Reprod Biol. 2004; 117:82e86.
- Holzer A, Jirecek ST, Illievich UM, Huber J, Wenzl R. Laparoscopic versus open myomectomy: a double-blind study to evaluate postoperative pain. Anesth Analg. 2006; 102:1480e1484.
- Menzies D, Ellis H. Intestinal obstruction from adhesions – how big is the problem? Ann R Coll Surg Engl. 1990;72:60e63.
- Kubinova K, Mara M, Horak P, Kuzel D, Dohnalova A. Reproduction after myomectomy: comparison of patients with and without second-look laparoscopy. Minim Invasive Ther Allied Technol. 2012; 21:118e124.
- Agdi M, Tulandi T. Endoscopic management of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2008;22:707e716.
- Klatsky PC, Tran ND, Caughey AB, Fujimoto VY. Fibroids and reproductive outcomes: a systematic literature review from conception to delivery. Am J Obstet Gynecol. 2008; 198:357e366.
- Levi AA. Rupture of the pregnant uterus. Obstet Gynecol. 1961; 18:223e229.
- Garnet J. Uterine rupture during pregnancy. Obstet Gynecol. 1964; 23:898e905.
- Golan D, Aharoni A, Gonen R, Boss Y, Sharf M. Early spontaneous rupture of the post myomectomy gravid uterus. Int J Gynecol Obstet. 1990; 31:167e170.
- Dubuisson JB, Fauconnier A, Deffarges J, Norgaard C, Kreiker G, Chapron C. Pregnancy outcome and deliveries following laparoscopic myomectomy. Hum Reprod. 2000; 15:869e873.
- Parker WH, Einarsson J, Istre O, Dubuisson JB. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol. 2010; 17: 551e554.
- Kumakiri J, Takeuchi H, Itoh S, et al. Prospective evaluation for the feasibility and safety of vaginal birth after laparoscopic myomectomy. J Minim Invasive Gynecol. 2008; 15:420e424.

Mastita post-partum
Daniela Stan, Mihai Mitran
Începutul în alăptare poate fi lin, fără probleme, sau poate fi uşor anevoios, cu dificultăţi mai mici sau mai mari. Printre aceste dificultăţi se numără mastita, denumirea clinică a infecţiei mamare prezentă la mamele care alăptează. Aceasta este provocată de blocarea canalelor de lapte atunci când bebe...
Restaurarea cu răşini compozite prin „stamp technique” în sarcină – prezentare de caz
Iulian Băluţă, Irina-Maria Gheorghiu, Paula Perlea, Loredana Mitran, Mihai Mitran
Restaurările coronare directe ale pierderilor de ţesut dur dentar, utilizând răşini compozite, în perioada de sarcină, prezintă particularităţi de tratament condiţionate de situaţia fiziologică ...
Cancerul colorectal în sarcină
Anca Zgură, Laurenţia Galeş, Elvira Brătilă, Rodica ANGHEL
Incidenţa cancerului colorectal în timpul sarcinii este mică, de un caz la 1. 000 de sarcini. Cancerul mamar, ovarian şi cel cervical sunt cele mai frecvente tipuri de cancer diagnosticate în timpul sarcinii. Manifestările întâlnite în cancerul colorectal, precum dureri abdominale, constipaţie, vărsături, gre...
Enterocel voluminos – studiu de caz
Constantin Viorel Cristurean, Dragoş-Marian Brezeanu
Enterocelul reprezintă protruzia intestinului subţire la nivelul peretelui superior al vaginului. Prolapsul genital are o prevalenţă de aproximativ 3-6%. În majoritatea cazurilor, peste 90%, este în stadiul I sau II, cu o incidenţă de aproximativ 43,3% pentru stadiul I şi de aproximativ 47% pentru stadi...
Corelaţia dintre factorii demografici şi rata de persistenţă/recurenţă a leziunilor CIN după conizaţie
Calina Maier, Mihai Mitran, Radu Vlădăreanu, Elvira Brătilă
Cu toate că înţelegerea epidemiologiei leziunilor cervicale intraepiteliale de grad înalt (CIN 2/3) s-a îmbunătăţit semnificativ, cofactorii implicaţi în istoria naturală a infecţiei c...