Provocarea trombofiliei: profilul pacientelor cu trombofilii compuse rare
The challenge of thrombophilia: the profile of patients with rare compound thrombophilias
Abstract
Thrombophilia is a multigenic disorder. Factor V Leiden mutation and protein gene G20210A mutation are the most common inherited thrombophilias. Individuals who are homozygous have a higher risk of thrombosis compared to those who are heterozygous. Inherited thrombophilia is associated with a predisposition to venous – not arterial – thromboembolism. Pregnancy increases the risk of developing venous thromboembolism. The aim of this study is to find the link between inherited thrombophilia (compound homozygous polymorphisms) and obstetric pathology in pregnant women.Keywords
venous thrombosisthrombophiliapregnancymiscarriageRezumat
Trombofilia este o patologie multigenică. Mutaţia factorului V Leiden şi mutaţia genei protrombinei G20210A sunt cele mai frecvente trombofilii ereditare din lume. Pacienţii homozigoţi au un risc mai mare de tromboză în comparaţie cu cei care sunt heterozigoţi. Trombofilia ereditară este asociată cu o predispoziţie la tromboembolism venos, nu arterial. Sarcina creşte riscul de a dezvolta tromboembolism venos. Scopul acestui studiu este de a găsi legătura între trombofilia ereditară (homozigotia compusă) şi patologia obstetricală existentă la gravide.Cuvinte Cheie
tromboză venoasătrombofiliesarcinăavortIntroduction
Thrombophilia is a hemostasis disorder that increases the risk of venous thromboembolism. Thrombotic events are recognized as a significant source of mortality and morbidity during pregnancy.
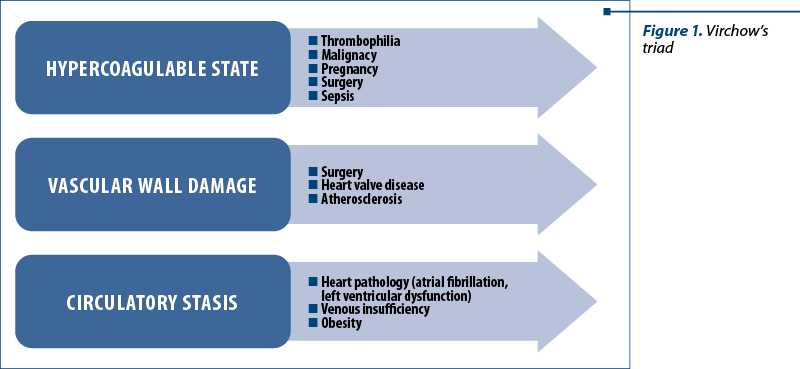
The pathologist Rudolph Virchow was the first to describe the three main factors that predispose to thrombosis. Virchow’s triad postulated that thrombus formation and propagation resulted from abnormalities in three key areas(1,2,3):
-
Activation of blood coagulation.
-
Alterations in blood flow – venous stasis.
-
Vascular endothelial injury – vein damage.
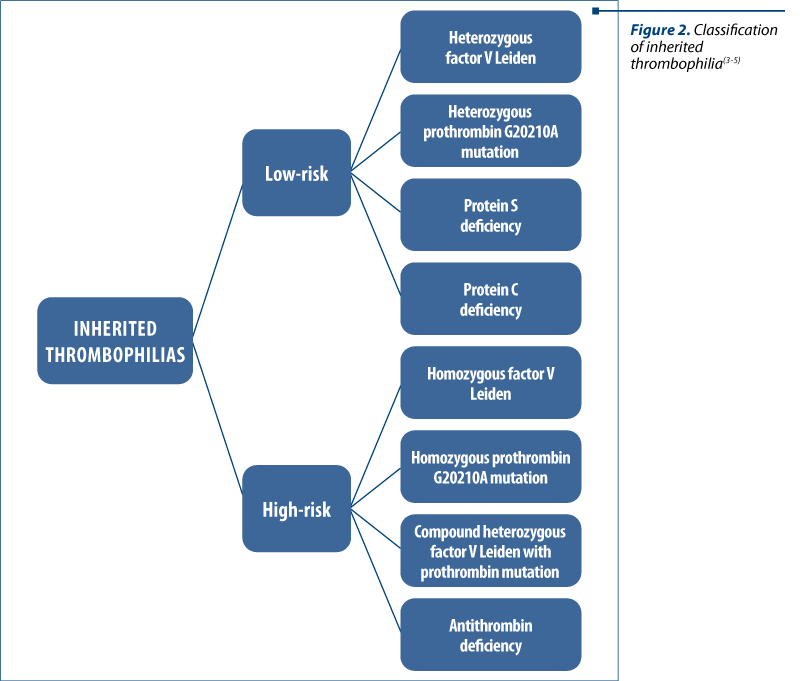
Thrombophilia can be classified as low risk or high risk, based on the relative increased risk of venous thromboembolism associated with the specific thrombophilia.
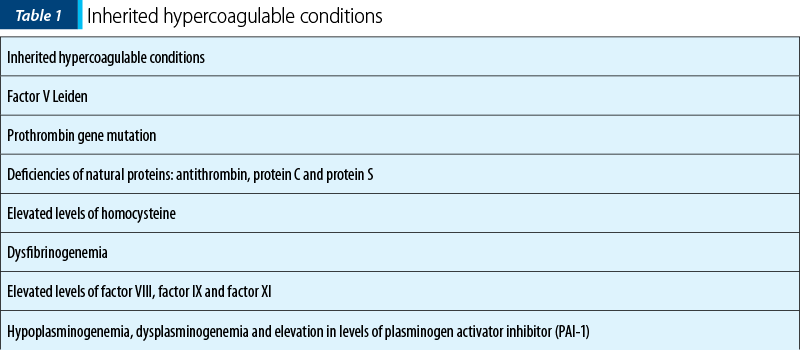
The most frequent causes of an inherited hypercoagulable state are the factor V Leiden mutation and the prothrombin gene mutation, which together represent 50 to 60 percent of cases. The remaining cases are represented by defects in protein S, protein C, and antithrombin III(6-10).
Materials and method
A retrospective 6-month cohort study was conducted within the Bucharest Emergency University Hospital between June and December 2018. We included in the study 459 pregnant women, with gestational ages ranging from 14 weeks to 28 weeks.
The pregnant women included in the study were tested for hereditary thrombophilia and the laboratory samples included: factor V Leiden, homocysteine, prothrombin G20210A mutations and antithrombin, protein S and protein C deficiencies, gene MTHFR mutation and mutation of factor XIII.
This study was approved by the Ethical Committee of the Bucharest University Emergency Hospital, and the informed consent was obtained from each woman. All statistical analyses were performed using SPSS version 21.

Results
The average age of patients included in the study was 33 years old, the average weight was 68 kg, the average height was 165 cm, and the average Body Mass Index was 25.20.
a) Association of the homozygous thrombophilic mutation of factor V Leiden and the homozygous mutation of prothrombin gene
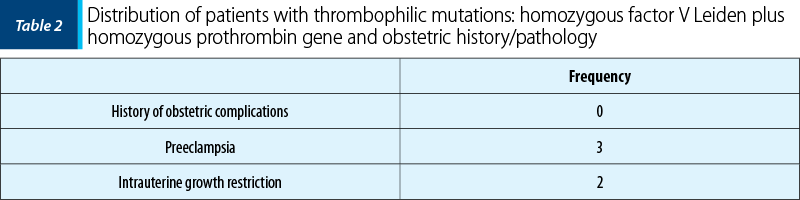
In the studied group, we had three patients who had thrombophilic mutations associated: homozygous factor V Leiden and homozygous prothrombin mutation.
All three patients had a history of two recurrent miscarriages in the first trimester.
All patients who had been diagnosed with compound homozygous factor V Leiden and homozygous prothrombin gene also had preeclampsia (three out of three patients) and intrauterine growth restriction (two patients out of three).
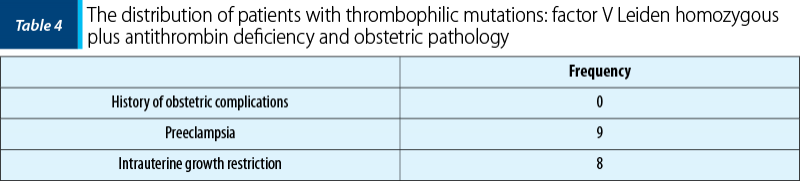
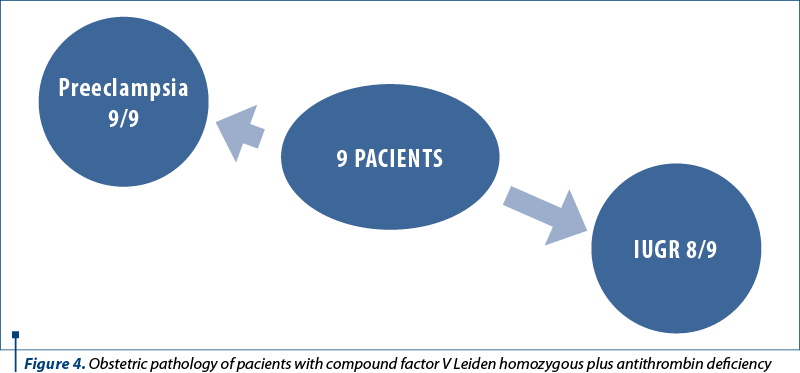
b) Compound homozygous mutation of factor V Leiden and antithrombin deficiency
In the study group, there were nine patients who had thrombophilic mutations associated: homozygous factor V Leiden and antithrombin deficiency.
Six patients had two recurrent miscarriages, two patients lost three pregnancies, and one patient lost five consecutive pregnancies.
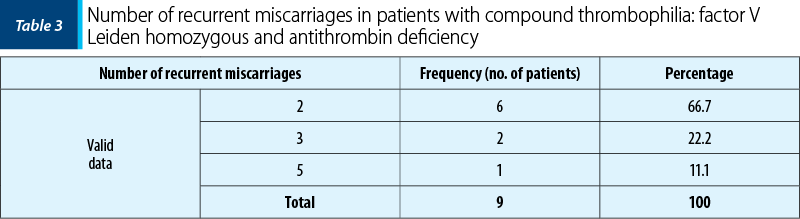
In the first trimester, seven patients had two miscarriages, and two patients had three miscarriages. In the second trimester, one patient lost a pregnancy and one patient lost two pregnancies; in the third trimester, no patient lost any pregnancy.
Of the nine patients who had thrombophilic homozygous mutations of factor V Leiden and antithrombin deficiency, nine had preeclampsia (nine out of nine patients) and eight patients had intrauterine growth restriction (eight patients out of nine).
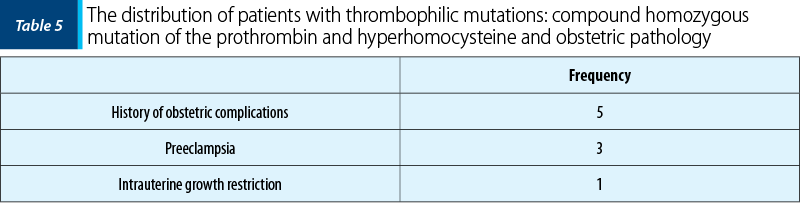
c) Compound homozygous mutation of the prothrombin and hyperhomocysteine
In the studied group, there were five patients with compound homozygous mutation of the prothrombin and hyperhomocysteine.
Of the five patients, four patients lost two pregnancies and one patient lost three consecutive pregnancies. In the first trimester, four patients lost two pregnancies and one patient lost three pregnancies. In the second and third trimesters, the patients did not lose any pregnancies.
Of the five patients who had these thrombophilic mutations, three had preeclampsia (three out of five patients) and one had been diagnosed with intrauterine growth restriction (one patient out of five).
Discussion
Venous thromboembolism is a leading cause of maternal mortality. Few studies have evaluated the individual risk of gestational thrombosis associated with heritable thrombophilia.
The risk of thrombosis in individuals with extremely rare compound thrombophilias, such as homozygous factor V Leiden plus homozygous prothrombin G20210A, homozygous factor V Leiden plus antithrombin deficiency and homozygous prothrombin plus hyperhomocyesteine, is unknown.
Intrauterine growth restriction (IUGR) and preeclampsia are an important cause of fetal and neonatal morbidity and mortality. Several studies showed an association between inherited thrombophilia and complications, such as interauterine fetal death, preeclampsia and placental abruption. The patients included in our study diagnosed with associated thrombophilia mutations had a significant obstetrical history for preeclampsia and IUGR.
Conclusions
The diagnosis of most thrombophilias is relatively easy and is accomplished with blood tests. Thrombophilias are associated with an increased risk of adverse obstetric outcomes such as stillbirth, fetal growth impairment and preeclampsia. The present report documents a clear association between compound thrombophilias mutations and fetal loss, preeclampsia and intrauterine growth restriction. n
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Dickson BC. Venous thrombosis: on the history of Virchow’s triad. Univ Toronto Med J. 2004; 81(3):166-71.
-
Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol. 2008; 143(2):180-90.
-
Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. 2005; 143(10):697-706.
-
Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141(2):e691S-e736S.
-
Marik PE, Plante LA. Venous thromboembolic disease and pregnancy. N Engl J Med. 2008; 359(19):2025-33.
-
Mateo J, Oliver A, Borrell M, Sala N, Fontcuberta J. Laboratory evaluation and clinical characteristics of 2,132 consecutive unselected patients with venous thromboembolism. Results of the Spanish Multicentric Study on Thrombophilia (EMET Study). Thromb Haemost. 1997; 77(03):444-451.
-
Margaglione M, Brancaccio V, Giuliani N, D’Andrea G, Cappucci G, Iannaccone L, Di Minno G. Increased risk for venous thrombosis in carriers of the prothrombin G→ A20210 gene variant. Ann Int Med. 1998; 129(2):89-93.
-
Crowther MA, Kelton JG. Congenital thrombophilic states associated with venous thrombosis: a qualitative overview and proposed classification system. Ann Int Med. 2003; 138(2):128-34.
-
Dahlbäck B. Advances in understanding pathogenic mechanisms of thrombophilic disorders. Blood. 2008; 112(1):19-27.
-
Haverkate F, Samama M. Familial dysfibrinogenemia and thrombophilia. Thromb Haemost. 1995; 73(1):151-61.

Nefrectomie laparoscopică cu extragerea transvaginală a rinichiului. Primul caz realizat în România – premieră naţională
Titus Sorin Pătrăşcoiu, Corneliu Roşulescu, Elvira Brătilă, Ioan Prie, Laura Popa, Claudia Pătrăşcoiu, Narcis Copca
Introducere şi obiectiv. Prezentăm cazul unei femei de 32 de ani care s-a prezentat în departamentul nostru de la Spitalul Clinic ...
Caracteristicile neonatale după transfer de embrioni fresh sau congelaţi la paciente normogonadotrope, tinere şi sănătoase
Annamaria Virginaş, Bogdan Cârstea, Szidonia Koszeghi, Istvan Barna Nagy, Zolna Virginas, Tamas Korosi, Gabor Vajta
Scop. A evalua dacă transferul de embrioni congelaţi (FET) are efecte benefice asupra greutăţii nou-născutului, comparativ cu tran...
Diagnosticul adenomiozei uterine la pacientele de vârstă reproductivă
Livia Cosma, Corina Gică, George Iancu, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu, Nicolae Gică
Adenomioza uterină este o patologie ginecologică ce este caracterizată de prezenţa insulelor ectopice de ţesut endometrial în miometru. Această boală afectează 20% dintre femeile de vârstă reproduc...
Tumoră spinală cervicală asociată sarcinii
Oana Bodean, Mirela Moarcăş, Diana Ioana Voicu, Octavian Munteanu, Luciana Grozavu-Arsene, Florina Păuleț, Monica-Mihaela Cîrstoiu
Tumorile spinale sunt rar întâlnite în sarcină, dar atunci când sunt extinse, pot cauza probleme grave prin efectele neurologice rapid progresive date de compresia medulară. Tumorile cu celule Schw...
Pitiriazisul rozat în timpul sarcinii – ce ar trebui să ştie obstetricienii?
Anca A. Simionescu
Pitiriazisul rozat (PR) este o boală eruptivă cutanată care apare frecvent în sarcină. Lucrarea abordează diagnosticul şi tratamentul pe care ar trebui să le cunoască obstetricienii în privinţa acestei patologii. PR apare ca o erupţie eritemato-nepruriginoasă, de obicei localizată pe torace şi umeri, sub fo...