The Bartholin gland cyst – actual therapeutic approaches and case report
Chistul de glandă Bartholin – abordări terapeutice actuale şi prezentare de caz
Abstract
Bartholin gland cysts account for 2% of all gynecologic visits per year. Although the treatments for Bartholin gland cysts seem apparently simple, recurrent cysts as well as the differential diagnosis between simple cyst, abscess or malignant pathology can complicate the management for this apparent common problem. Bartholin gland disorders, such as cysts and abscesses, can significantly impact a woman’s quality of life, necessitating effective and lasting interventions. Starting from the standard conduct of authors in Bartholin gland cyst, the article aims to review the current therapeutic techniques and to present a case report of an approach based on the excision of the gland.Keywords
Bartholin glandglandular excisionBartholin gland cystRezumat
Chisturile glandei Bartholin reprezintă 2% din toate vizitele ginecologice pe an. Cu toate că metodele terapeutice pentru chisturile glandei Bartholin sunt aparent simple, chisturile recurente, precum şi diagnosticul diferenţial între chist simplu, abces sau patologie malignă pot complica managementul acestei probleme aparent comune. Tulburările glandei Bartholin, cum ar fi chisturile şi abcesele, pot influenţa semnificativ calitatea vieţii unei femei, necesitând intervenţii eficiente şi de durată. Plecând de la conduita standard a autorilor în ceea ce priveşte chisturile glandei Bartholin, articolul îşi propune să revizuiască tehnicile terapeutice actuale şi să prezinte o abordare bazată pe excizia glandei.Cuvinte Cheie
glandă Bartholinexcizie glandularăchist de glandă BartholinIntroduction
The Bartholin’s glands, initially described in 1677 by the Danish anatomist Casper Bartholin, also known as the greater vestibular glands, encompass a pair of anatomical structures located in proximity to the vaginal entrance. Each gland is characterized by an approximate diameter of 1 cm, accompanied by a narrow duct measuring 2.5 cm, which extends to the surface. Traditionally believed to facilitate lubrication during sexual intercourse and maintain the moist surface of the vulva, the removal of these glands does not appear to compromise the vestibular epithelium or sexual function, due to the presence of other glands(1,2).
These glands are susceptible to obstruction at their vestibular orifice, often due to friction during intercourse, leading to edema. This can result in the formation of cysts or abscesses, with approximately 2% of women experiencing such conditions in their lifetime, particularly observed in single women and in those from lower socioeconomic backgrounds(2,3).
The management of Bartholin’s duct cysts is contingent upon the patient’s symptoms. Asymptomatic cases may not necessitate treatment, whereas symptomatic Bartholin’s duct cysts and gland abscesses typically require drainage. Abscess resolution without intervention is rare unless spontaneous rupture occurs. Surgical treatment options for Bartholin duct or gland abscesses include fistulization, which involves creating a new duct opening through incision and drainage with the insertion of a Word catheter, marsupialization to keep the lesion open and promote healing, or excision of the Bartholin gland(4-6).
Fistulization encompasses the process of making an incision and draining the lesion, followed by the insertion of a Word catheter. This procedure establishes a new duct opening, allowing the lesion to drain continuously and facilitating internal healing. The placement of a Word catheter is contraindicated in individuals with a known latex allergy, as the catheter stem contains latex. In cases of latex allergy, marsupialization is preferred as the procedure of choice(4,6,7).
Marsupialization is a surgical procedure, starting from a 1.5-to-3-cm incision just above the hymenal ring within the introitus. The incision edges are then tented and sutured open to evert the cyst wall, facilitating epithelialization. Marsupialization may be recommended for women with larger or recurrent Bartholin duct cysts or abscesses. In women aged over 40 years old, excision with biopsy may be considered to rule out cancer(8,9).
CO2 laser treatment involves creating an incision with a laser and vaporizing the cyst wall from within. CO2 laser treatment offers numerous benefits, including the ability to perform it in an office setting, with reduced risks of bleeding, recurrence, scarring, and persistent drainage. However, it is important to note that this treatment option is typically more expensive than Word catheter placement(9).





Case report
A 39-year-old female was admitted to the obstetrics and gynecology department, reporting a swelling in the left labial region persisting for approximately one month. Initially small and painless, the swelling exhibited gradual growth, with a more pronounced increase in size observed over the last days.
Upon clinical examination, a single swelling was identified in the left labium majus, spanning from the pubic bone level to just above the vulval fourchette inferiorly. The swelling measured 3/3/3 cm, presenting as a soft yet tense mass with a smooth surface and no discernible tenderness or local warmth. Positioned subcutaneously, it exhibited no deep extension into tissue planes. Fluctuation was evident, while transillumination yielded negative results. No enlargement of lymph nodes was observed. A clinical diagnosis of a Bartholin gland cyst was established, and surgical excision was planned.
Under spinal anesthesia, with the patient positioned in lithotomy, a vertical incision of elliptical configuration was performed. The ensuing elevation of skin flaps facilitated exposure to the sizable cystic swelling, which was subsequently delineated and entirely excised through a combination of blunt and precise dissection along all dimensions.
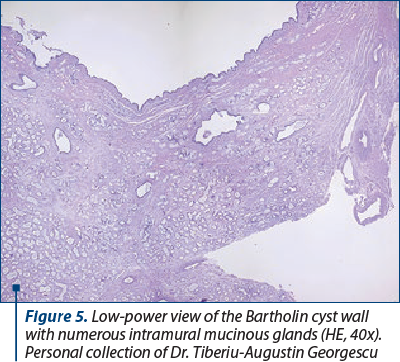
The excised tissue underwent histopathological examination, revealing upon cross-section a uniloculated cyst with a smooth, greyish-brown inner surface. The microscopic examination unveiled a cyst lining composed of cuboidal to columnar epithelium, and the cyst wall exhibited accumulations of inflammatory cells.
The postoperative period underwent without untoward events, with the patient demonstrating expeditious recovery, leading to discharge on the seventh day post-surgery subsequent to suture removal. Upon follow-up three weeks later, the patient presented as comfortable and in a state of overall well-being. Notably, no instances of recurrence have been reported during the following year.
Discussion
Bartholin gland abscesses and cysts are common problems in women of reproductive age. The ideal treatment should have a low recurrence rate and should not cause sexual dysfunction, dyspareunia or decreased lubrication.
Incision, drainage and needle aspiration are simple procedures, but they have higher recurrence rates compared with the previously discussed office procedures, and are not recommended(1,10).
In literature, the impact of Bartholin cyst or abscess treatments on sexual function has not been investigated deeply. The Female Sexual Function Index (FSFI) is a validated assessment tool to evaluate sexual function. The FSFI not only evaluates the existence of dyspareunia, but it also assess sexual desire, arousal, orgasm and lubrication(11).
In their comprehensive study, Mathyk et al. undertook a comparative analysis between excision and marsupialization techniques. Notably, both approaches demonstrated consistently low TFSI scores. However, excision emerged with lower recurrence rates. It is essential to acknowledge that the complete removal of the gland may potentially lead to increased bleeding and scarring. Further research is needed to assess and elucidate the nuanced considerations associated with these surgical interventions(10).
Conclusions
The identification and management of Bartholin gland cysts remain an integral aspect of gynecological practice. Although tried and proven methods of treatment have been described, there is still room for a better, less painful, more successful treatment. When treating patients with Bartholin cysts or abscesses, it is important to remember that the long-term goal of any treatment is the resolution of the problem and suppression of recurrences.
It is important to note, however, that surgical techniques may need to be modified or adapted to account for the differences in other factors that can affect surgical outcomes in these patients. Additionally, further research is needed to confirm the effectiveness of these techniques on each patient and to identify any potential risks or complications. It is also important to consider the unique needs of each patient, as well as the potential long-term effects of the surgery on their overall and sexual health.
Corresponding author:
Tiberiu-Augustin Georgescu
E-mail: tiberiuaugustin.georgescu@gmail.com
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
- Omole F, Kelsey RC, Phillips K, Cunningham K. Bartholin duct cyst and gland abscess: office management. Am Fam Physician. 2019;99(12):760-6.
- Cunningham FG, Leveno KJ, Bloom S, Gilstrap L. Williams Obstetrics (23rd Edition). McGraw-Hill Professional Publishing, New York, USA, 2010.
- Marzano DA, Haefner HK. The Bartholin gland cyst: past, present, and future.
- J Low Genit Tract Dis. 2004;8(3):195–204.
- Kessous R, Aricha-Tamir B, Sheizaf B, Steiner N, Moran-Gilad J, Weintraub AY. Clinical and microbiological characteristics of Bartholin gland abscesses. Obstet Gynecol. 2013;122(4):794-99.
- Heller DS. Benign tumors and tumor-like lesions of the vulva. Clin Obstet Gynecol. 2015;58(3):526-35.
- Lee MY, Dalpiaz A, Schwamb R, Miao Y, Waltzer W, Khan A. Clinical pathology of Bartholin’s glands: a review of the literature. Curr Urol. 2015;8(1):22-5.
- Dole DM, Nypaver C. Management of Bartholin duct cysts and gland abscesses. J Midwifery Women’s Health. 2019;64(3):337-43.
- Pundir J, Auld BJ. A review of the management of diseases of the Bartholin’s gland. J Obstet Gynaecol. 2008;28(2):161-5.
- Frega A, Schimberni M, Ralli E, et al. Complication and recurrence rate in laser CO2 versus traditional surgery in the treatment of Bartholin’s gland cyst. Arch Gynecol Obstet. 2016;294(2):303-9.
- Mathyk BA, Cetin BA, Cetin H. Sexual function after Bartholin gland abscess treatment: A randomized trial of the marsupialization and excision methods. Eur J Obstet Gynecol Reprod Biol. 2018;230:188–91.
- Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191-208.

March-May 2024 Calendar
March-May 2024 Calendar...
Giant isthmic fibromatous nodule developing within the cervix – clinical case
Diana Popovici, Răzvan Socolov, Emil Anton, Loredana Hurjui, Cătălina Stan, Raluca Bălan, Costel Bradea, Ion Hurjui, Andrei Hurjui, Svetlana Bereşteanu, Florina-Iuliana Rusu, Sorana-Caterina Anton
The fibromatous nodule (uterine fibroid) is a benign tumor that develops from tissue similar to the uterine muscle, being aided by...
Ultrasound-based differential diagnosis of fetal abdominal wall defects in early pregnancy
Mircea Octavian Poenaru, Delia-Maria Bogheanu, Romina-Marina Sima, Liana Pleș
Fetal abdominal wall defects (AWDs) encompass a wide range of congenital anomalies that involve the incomplete closure or disruption of the abdominal wall during the embryonic development. ...
Giant isthmic fibromatous nodule developing within the cervix – clinical case
Diana Popovici, Răzvan Socolov, Emil Anton, Loredana Hurjui, Cătălina Stan, Raluca Bălan, Costel Bradea, Ion Hurjui, Andrei Hurjui, Svetlana Bereşteanu, Florina-Iuliana Rusu, Sorana-Caterina Anton
The fibromatous nodule (uterine fibroid) is a benign tumor that develops from tissue similar to the uterine muscle, being aided by...
Miomectomia concomitentă operației cezariene: controverse, indicaţii şi complicaţii
Diana Șerban, Mădălina-Nicoleta Mitroiu, Cristiana-Elena Durdu, Roxana-Elena Bohîțea
Miomectomia efectuată în timpul operației de cezariană rămâne un subiect de controversă, din cauza potențialelor complicații asociate, în special în cazul mioamelor de dimensiuni mari....