Cystic hygroma presenting as an isolated malformation – case report and literature review
Higromă chistică prezentată ca o formaţiune izolată – raportare de caz şi review al literaturii
Abstract
Nuchal translucency (NT) is the ultrasound observation of subcutaneous fluid accumulation at the back of the fetal neck, which, when excessively enlarged, can lead to nuchal edema or cystic hygroma. Elevated NT is associated with chromosomal anomalies and pregnancy complications. Cystic hygroma (CH) is caused by lymphatic system blockage, resulting in fluid-filled pseudocysts. Its incidence varies, but it is usually rare in the general population. CH is commonly detected during prenatal screenings, with higher incidences in populations undergoing extensive testing. It can be associated with genetic conditions like Turner and Down syndromes, influenced by geographic regions and maternal age. Ultrasound is an established method for CH diagnosis, revealing multiseptated cystic masses. A normal karyotype is found in only 20-50% of cases. The management varies from expectant monitoring to pregnancy termination, depending on severity and associated anomalies. The risk of recurrence depends on karyotype; normal karyotypes have a higher recurrence risk. Spontaneous resolution of cystic hygroma has been reported in some cases. To illustrate this situation, we present the case of a patient with a spontaneously regressed CH associated with a normal karyotype and a favorable outcome. In conclusion, cystic hygroma management and counseling should consider the presence of chromosomal abnormalities, but recent studies reveal a more optimistic perspective once these abnormalities are ruled out. Collaborative counseling is essential for informed decision-making during pregnancy regarding fetal interventions, neonatal care or palliative care.Keywords
cystic hygromaprenatal diagnosisultrasonographyprenatalnoninvasive prenatal testingRezumat
Translucenţa nucală (TN) reprezintă acumularea de lichid subcutanat în partea posterioară a gâtului fetal, care, atunci când atinge dimensiuni excesiv de mari, poate conduce la edem nucal sau higromă chistică (HC). Creşterea TN este asociată în general cu anomalii cromozomiale şi cu diverse complicaţii în timpul sarcinii. HC este cauzată de blocarea sistemului limfatic. Incidenţa sa variază, dar este de obicei rară în populaţia generală. Higroma chistică este adesea detectată în timpul screeningului prenatal, cu incidenţă mai mare în populaţiile care beneficiază de metode extinse de testare. Poate fi asociată cu afecţiuni genetice precum sindromul Turner şi sindromul Down, fiind influenţată de regiuni geografice şi de vârsta maternă. Examinarea ecografică este metoda unanim acceptată pentru diagnosticul CH, întrucât permite identificarea unor formaţiuni chistice multiseptate. Un cariotip normal este constatat în doar 20-50% dintre cazuri. Managementul variază de la conduita expectativă la întreruperea sarcinii, în funcţie de severitate şi de anomaliile asociate. Riscul de recurenţă depinde de cariotip, cariotipurile normale având un risc mai mare de recurenţă. Remisiunea spontană a CH a fost raportată în unele cazuri. Pentru a ilustra această situaţie, prezentăm cazul unei paciente cu o higromă chistică remisă spontan, asociată cu un cariotip normal şi cu un rezultat clinic şi obstetrical favorabil. În concluzie, managementul şi consilierea higromei chistice ar trebui să ia în considerare prezenţa anomalilor cromozomiale, iar studiile recente relevă o perspectivă mai optimistă odată ce aceste anomalii sunt eliminate. Consilierea colaborativă este esenţială pentru luarea deciziilor informate în timpul sarcinii în ceea ce priveşte oportunitatea intervenţiilor fetale, îngrijirea neonatală sau îngrijirea paliativă.Cuvinte Cheie
higromă chisticădiagnostic prenatalultrasonografieprenataltest prenatal neinvazivNuchal translucency (NT) is the ultrasound observation of subcutaneous fluid accumulation at the back of the fetal neck. When this accumulation becomes excessively enlarged, it can lead to nuchal edema, which is referred to as increased NT or cystic hygroma. Elevated NT has been demonstrated to be associated with different chromosomal anomalies or structural abnormalities and with unfavorable pregnancy outcomes(1).
Cystic hygroma (CH) is the result of a blockage in the lymphatic system, leading to the development of pseudocysts filled with liquid content in the fetal nuchal region that can reach significant sizes. The term “hygroma” derives from the Greek words hygros, meaning liquid, and oma, meaning tumor.
This congenital malformation occurs in approximately 1% of fetuses between 9 and 16 weeks of gestation and is associated with the occurrence of aneuploidies in 65% of cases. The incidence of CH can vary depending on the population and the specific underlying causes or risk factors, and it is generally considered to occur in approximately 1 in 268 pregnancies(2). The reported incidence of cystic hygroma in the general population is relatively low, estimated to be around 1 in 4000 live births. An older study reported an overall incidence of approximately 1 in 1000-6000 births and 1 in 750 spontaneous abortions(3).
However, the incidence can vary among specific populations or groups, based on various factors such as genetics, ethnicity and geographic regions. Cystic hygroma is often detected during prenatal screenings, and certain studies have reported higher incidences in populations that undergo more extensive prenatal testing and ultrasound examinations. Cystic hygromas can be associated with specific genetic conditions, and the incidence may be higher in populations where these genetic conditions are more prevalent. For example, the incidence of CH may be higher in populations with a higher prevalence of Turner syndrome or Down syndrome. The incidence of cystic hygroma can also vary by geographic region and it may be influenced by factors such as access to healthcare, prenatal screening practices, and the prevalence of genetic conditions in specific regions. Moreover, advanced maternal age is associated with a higher risk of chromosomal abnormalities and, by extension, an increased risk of CH. It is essential to consult with healthcare professionals or genetic counselors for more precise information on the incidence and risk factors related to CH in a specific context or population.
When generalized, it can lead do hydrops fetalis, a condition involving abnormal accumulation of fluid in multiple fetal body compartments, such as the chest and abdomen. Hydrops fetalis can result from a variety of underlying causes, including heart, blood or immune system disorders. Historically, non-immune hydrops fetalis (NIHF) has been regarded as a fetal condition with a high risk of lethality(4).
Cystic hygroma begins its development at about eight weeks of gestation, when six lymphatic sacs can be identified in the developing embryo. These lymphatic sacs are described as follows: two jugulars, two iliac, one at the base of the mesenteric root, and one dorsal to the abdominal aorta (cisterna chyli). Later, a network of lymphatics develops, allowing lymphatic communication between various regions. During the ninth week of gestation, these sacs are invaded by connective tissue as lymph nodes develop. CH arise from the sequestration of lymphatic tissue within the lymphatic-venous sacs during the aforementioned development. These sequestered tissues fail to communicate with the rest of the lymphatic or venous system. Later, dilation of the sequestered lymphatic tissues occurs as lymphatic liquid accumulates, resulting in the cystic morphology of these lesions.
Anatomical studies show that the most frequent locations of CH are the cervicofacial regions (especially the posterior cervical triangle), axilla, mediastinum, inguinal and sublingual regions. Rare locations are represented by the limbs, thoracic wall, cheeks, lumbar region, and the suprasternal area. Most frequently, it is a single and isolated location(5).
The prenatal diagnosis of cystic hygroma through ultrasound is well established. The characteristic ultrasound appearance during antenatal ultrasonography is a multiseptated cystic mass with thin walls. Occasionally, the cystic mass may exhibit a more complex echogenic texture with both cystic and solid components(6).
Cystic hygroma can occur isolated, but a normal karyotype can be found in only 20-50% of cases(7). It can also be diagnosed in fetuses with genetic anomalies, with 62% of cases being associated with conditions such as Turner syndrome, Down syndrome (trisomy 21) or Noonan syndrome(8-11). These genetic syndromes are known to be associated with an increased risk of CH as one of their clinical features.
The differential diagnosis can be made with posterior cervical wall anomalies, such as meningocele or encephalocele, and with anterior cervical wall anomalies, such as thyroglossal duct cyst, branchial cyst (dermoid and epidermoid cyst), bronchogenic (visceral) cyst or mandibular hamartoma and cervical thymic cyst.
The outcome of CH is in close correlation with the associated anomalies, the timing of appearance, and location. A recent study showed that, once the presence of fetal chromosomal abnormalities is ruled out, there is a significantly lower incidence of major structural fetal abnormalities, standing at only 13%, and normal fetuses exhibit a 77% survival rate(12).
The therapeutic management varies widely, from expectant management to termination of pregnancy, depending on the severity of the CH and the associated anomalies. The expectant management approach is suitable for cystic hygromas that develop in fetuses without associated chromosomal abnormalities. Close ultrasound monitoring is recommended to assess dynamic changes, such as growth, reduction in size, or even the complete resolution of the fluid accumulation. On the other hand, in severe cases of CH, termination of pregnancy may be recommended, especially when there are severe associated chromosomal abnormalities. In cases with moderate involvement, surgical intervention after birth is recommended, as antenatal drainage of the cystic hygroma has proven to be ineffective. In such cases, it is advisable to transfer the pregnant individual to a specialized neonatal care center (the respiratory complications are most common) and have access to a pediatric surgery center. It is important to acknowledge that the management approach should be tailored to each individual case, and decisions should be made in consultation with healthcare professionals and specialists, based on the specific circumstances and risks involved.
It is generally considered that the recurrence risk of CH depends on its association with fetal aneuploidies. In cases where cystic hygroma is associated with genetic syndromes, the risk of recurrence in future pregnancies is low. Chromosomal abnormalities typically occur sporadically, and the likelihood of them appearing in subsequent pregnancies is small.
However, in cases where the karyotype (chromosome pattern) is normal, the risk of recurrence is increased. This means that, if a previous pregnancy with CH had a normal chromosome pattern, there is a higher chance of cystic hygroma occurring in future pregnancies. It is important to consult with a healthcare provider or genetic counselor for personalized guidance and risk assessment in specific situations.
Regarding the situations in which cystic hygroma has a spontaneous resolution, a retrospective study took into account 68 fetuses diagnosed with simple nuchal hygromas between 10 and 14 weeks of gestation who underwent ultrasound evaluation and karyotyping. Those with normal chromosomal complements were monitored by ultrasound throughout the pregnancy to track the resolution of their hygromas. Twenty-three out of 27 fetuses with normal karyotypes spontaneously resolved their hygromas within four weeks of diagnosis and were phenotypically normal at birth. Forty-one fetuses had abnormal karyotypes, with trisomy 21 being the most frequent anomaly(13).
A more recent retrospective study on 185 cases with cystic hygroma showed that 34.1% of the fetuses had a normal karyotype, of which 56% had a major congenital anomaly(14). The authors suggest that an adverse outcome in pregnancies where first-trimester CH and a normal karyotype are present can be anticipated in the presence of structural anomalies or hydrops fetalis, while normally structured fetuses have a better prognosis.
To clinically illustrate this condition, we have chosen to present the case of a 30-year-old primiparous patient with no significant medical history. At 13 weeks of pregnancy, a diagnosis of cystic hygroma was made, measuring 4.8 mm. No other associated malformations were observed at the first-trimester morphology scan (Figures 1 and 2).
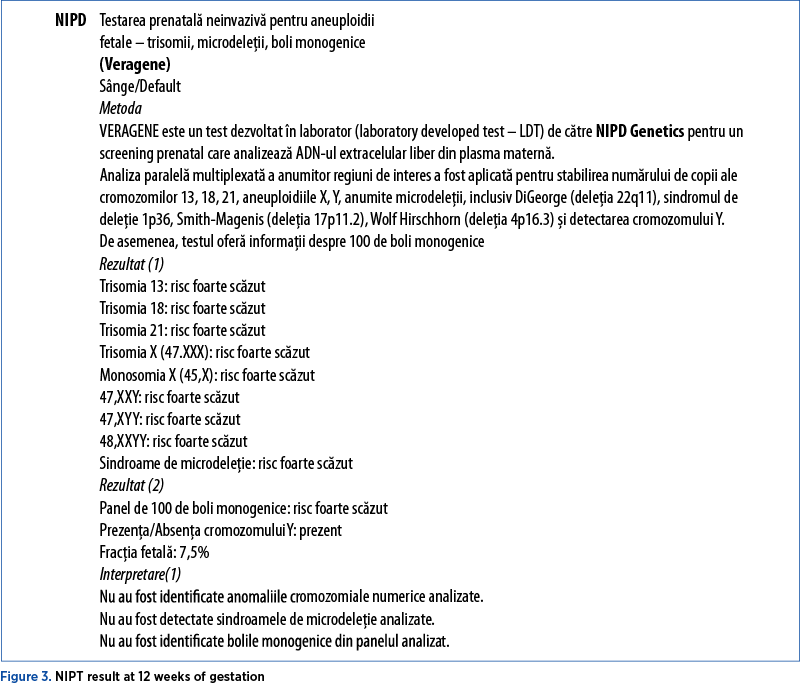
Despite the non-reassuring ultrasound findings, the patient decided to continue the pregnancy, and she underwent non-invasive prenatal testing (NIPD) at 13 weeks of gestation. No numerical chromosomal abnormalities analyzed were identified, the analyzed microdeletion syndromes were not detected, and no monogenic diseases from the analyzed panel were identified (Figure 3).
The patient returned for an ultrasound at 16 weeks of pregnancy, when the nuchal anomaly has regressed, with normal growth of the fetus. The second-trimester morphology scan did not reveal any pathological changes, and a nuchal fold measurement of 7 mm was described.
Amniocentesis was performed at 16 weeks of gestation, molecular prenatal karyotype from amniotic fluid was performed, and the microarray analysis identified a normal male profile without clinically significant microdeletions or microduplications in the analyzed chromosomal regions.
At 22 weeks of gestation, the fetus showed normal morphological development, without any pathological signs (Figures 4 and 5). There was no evidence of cystic hygroma, and there were no other associated ultrasound abnormalities. The fetus was following a typical growth curve. At present, the fetus is 31 weeks, showing a normal development, normal nuchal fold and the absence of other structural anomalies.
Cases of spontaneously regressed cystic hygroma, unassociated with other congenital malformations, with a favorable prognosis at birth, have been reported in the literature. In 2008, a case was presented in the literature, involving a patient in her third pregnancy, with no previous obstetric history(15). At nine weeks of gestation, the fetus exhibited CH, which spontaneously resolved at 12 weeks of gestation. The patient declined further investigations for karyotyping. At 24 weeks of gestation, an abdominal cystic formation was detected on ultrasound, which also spontaneously resolved at 26 weeks of gestation. At birth, the newborn had a normal karyotype and showed no developmental defects. Thus, it is emphasized that fetal anomalies such as cystic hygroma, when associated with a normal karyotype, have a favorable prognosis regarding spontaneous resolution.
Conclusions
When counseling individuals facing first-trimester septate cystic hygroma, the initial focus is often on the high probability of an abnormal karyotype, which is observed in 61% of cases(12).
Nevertheless, comprehending the underlying pathophysiological processes has resulted in the conceptualization of diagnostic protocols, enhanced comprehension of the root causes and, consequently, advances in fetal or neonatal treatments. Collaborative counseling is pivotal in assisting families in navigating choices during pregnancy, considering potential therapeutic interventions for the fetus, making decisions about neonatal management and, when necessary, embracing or transitioning to palliative care. Recent studies that prove the possibility of normal chromosomal fetuses with high survival rates highlight that such counseling can be more optimistic than previously anticipated once chromosomal abnormalities have been ruled out.



Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- Narava S, Balbir Singh S, Barpanda S, Bricker L. Outcome of pregnancies with first-trimester increased nuchal translucency and cystic hygroma in a tertiary maternity hospital in United Arab Emirates. Int J Gynaecol Obstet. 2022;159(3):841-849.
- Sherer DM, Hsieh V, Hall A, et al. Current Perspectives of Prenatal Cell-free DNA Screening in Clinical Management of First-Trimester Septated Cystic Hygroma. Int J Womens Health. 2022;14:1499-1518.
- Chen CP, Liu FF, Jan SW, et al. Cytogenetic evaluation of cystic hygroma associated with hydrops fetalis, oligohydramnios or intrauterine fetal death: the roles of amniocentesis, postmortem chorionic villus sampling and cystic hygroma paracentesis. Acta Obstet Gynecol Scand. 1996;75:454–8.
- Swearingen C, Colvin ZA, Leuthner SR. Nonimmune Hydrops Fetalis. Clin Perinatol. 2020;47(1):105-121.
- Mirza B, Ijaz L, Saleem M, Sharif M, Sheikh A. Cystic hygroma: an overview. J Cutan Aesthet Surg. 2010;3(3):139-44.
- Chen YN, Chen CP, Lin CJ, Chen SW. Prenatal Ultrasound Evaluation and Outcome of Pregnancy with Fetal Cystic Hygromas and Lymphangiomas. J Med Ultrasound. 2017;25(1):12-15.
- Malone FD, Ball RH, Nyberg DA, et al. First-trimester septated cystic hygroma: prevalence, natural history, and pediatric outcome. Obstet Gynecol. 2005;106(2):288–94.
- Izquierdo L, Kushnir O, Sanchez D, et al. Prenatal diagnosis of Noonan’s syndrome in a female infant with spontaneous resolution of cystic hygroma and hydrops. West J Med. 1990;152(4):418–21.
- Chen HY, Zheng JQ, Zhang HP. A case report of Turner syndrome associated with fetal nuchal cystic hygroma and bilateral syndactyly of the hands and feet. Ital J Pediatr. 2019;45(1):85.
- Vičić A, Hafner T, Bekavac Vlatković I, et al. Prenatal diagnosis of Down syndrome: A 13-year retrospective study. Taiwan J Obstet Gynecol. 2017;56(6):731-735.
- Witters G, Van Robays J, Willekes C, et al. Trisomy 13, 18, 21, Triploidy and Turner syndrome: the 5T’s. Look at the hands. Facts Views Vis Obgyn. 2011;3(1):15-21.
- Malone CM, Mullers S, Kelliher N, et al. Euploid First-Trimester CH: A More Benign Entity than Previously Thought? Fetal Diagn Ther. 2021;48(9):667-671.
- Johnson MP, Johnson A, Holzgreve W, Isada NB, Wapner RJ, Treadwell MC, Heeger S, Evans MI. First-trimester simple hygroma: cause and outcome. Am J Obstet Gynecol. 1993;168(1 Pt 1):156-61.
- Schreurs L, Lannoo L, De Catte L, et al. First trimester cystic hygroma colli: Retrospective analysis in a tertiary center. Eur J Obstet Gynecol Reprod Biol. 2018;231:60-64.
- Merenda A, Pisaturo ML, Laviscio P, et al. P25.12: Spontaneous resolution of cystic hygroma colli and intraabdominal cyst in a fetus with normal karyotype. Ultrasound Obstet Gynecol. 2008;32(Issue 3):401.

The importance of chronic endometritis and dysbiosis in implantation failure in IVF cycles
Laurenţiu-Mihai Dîră, Roxana Cristina Drăguşin, Constantin-Cristian Văduva, George Lucian Zorilă, Rodica Daniela Nagy, Ştefan-Gabriel Ciobanu, Elena-Iuliana-Anamaria Berbecaru, Iuliana-Alina Enache, Gabriel Dominic Iliescu
We often face in vitro fertilization cycles in which embryo implantation does not occur despite the apparent exclusion of other ma...
The role of the sentinel lymph node mapping in the actual treatment of endometrial cancer
Anca Hashemi, Andrei Manu, Cristina-Maria Iacob, Mihaela-Arina Banu, Cătălin Bogdan Coroleucă, Ciprian Andrei Coroleucă, Elvira Brătilă
In high-income countries, endometrial cancer is perhaps the most prevailing gynecological malignancy, with an incidence rate risin...
Endometrioma – the tip of the iceberg?
Andrei Manu, Ciprian Andrei Coroleucă, Cătălin Bogdan Coroleucă, Diana-Elena Comandașu, Diana-Elena Soare, Alexandra Bauşic, Cristina-Maria Iacob, Mihaela-Arina Banu, Anca Hashemi, Elvira Brătilă
About 10% of women of reproductive age have endometriosis, a chronic illness that may cause serious morbidity, being ultimately a ...
The role of the sentinel lymph node mapping in the actual treatment of endometrial cancer
Anca Hashemi, Andrei Manu, Cristina-Maria Iacob, Mihaela-Arina Banu, Cătălin Bogdan Coroleucă, Ciprian Andrei Coroleucă, Elvira Brătilă
In high-income countries, endometrial cancer is perhaps the most prevailing gynecological malignancy, with an incidence rate risin...
Endometrioma – the tip of the iceberg?
Andrei Manu, Ciprian Andrei Coroleucă, Cătălin Bogdan Coroleucă, Diana-Elena Comandașu, Diana-Elena Soare, Alexandra Bauşic, Cristina-Maria Iacob, Mihaela-Arina Banu, Anca Hashemi, Elvira Brătilă
About 10% of women of reproductive age have endometriosis, a chronic illness that may cause serious morbidity, being ultimately a ...