Fetal isolated vein of Galen aneurysmal malformation with spontaneous complete regression – a rare occurrence
Anevrism izolat de venă Galen diagnosticat antepartum, cu remisiune spontană completă – o situaţie rar întâlnită
Abstract
Vein of Galen aneurysmal malformation (VGAM) is a rare intracranial vascular malformation, commonly diagnosed using ultrasound in the third trimester of pregnancy. There is a 2-3:1 male predominance. The prenatal diagnosis enhances appropriate perinatal management. If the prenatal diagnosis is missed, VGAM is reported to be fatal in many cases, due to cardiac and neurological complications. A 24-year-old pregnant woman was referred to our tertiary prenatal diagnosis unit (University of Medicine and Pharmacy of Craiova, County Emergency Clinical Hospital of Craiova) for vascular cerebral malformation suspicion. We confirmed a turbulent arterial and venous flow using the color Doppler technique, within an anechoic structure, located in the midline of the posterior part of the third ventricle. The fetus did not develop signs of hydrops or cardiac failure in the prenatal period. The magnetic resonance imaging (MRI) was performed at 36 weeks of amenorrhea, to confirm the sonographic findings and to better predict the postnatal outcome, in the Radiology and Imaging Department of our university. The fetus (female, Apgar score 9, weighing 2720 grams) was delivered by caesarean section, at 37 gestational weeks. The neonatal period was complicated by pulmonary hypertension and mild cardiac events. The child evolved spontaneously favorably. At 32 months, the MRI showed normal intracranial vasculature. Currently, at 5 years of age, she has a completely normal neurologic development. In the last 15 years, the prenatal diagnosis of VGAM has been facilitated by the use of color Doppler mode, which is crucial for differentiating this malformation from midline cystic lesions of the fetal brain (being the only lesion that accurately displays blood flow within it). Fetal MRI may play an important role in customizing perinatal and long-term management. To our knowledge, this is the first case ever reported having a prenatal diagnosis and a spontaneous complete regression.Keywords
vein of Galen aneurysmal malformationmagnetic resonanceultrasoundcolor Dopplerspontaneous remissionRezumat
Malformaţia anevrismală a venei lui Galen (MAVG) este o malformaţie vasculară intracerebrală rară. De obicei, diagnosticul prenatal se precizează în al treilea trimestru de sarcină. Raportul dintre sexe este de 2-3:1, cu predominanţa sexului masculin. În absenţa diagnosticului prenatal (ce permite un management adecvat), MAVG este o afecţiune fatală în multe cazuri, prin complicaţii cardiace şi neurologice. Prezentăm cazul unei paciente în vârstă de 24 de ani, referită Unităţii de Diagnostic Antenatal (Universitatea de Medicină şi Farmacie Craiova, Spitalul Clinic Judeţean de Urgenţă Craiova) pentru suspiciune de malformaţie vasculară cerebrală. Am constatat în modul Doppler color un flux arterial şi venos turbulent, la nivelul unei structuri anecogene, situată pe linia mediană, posterior de ventriculul al treilea. Fătul nu a dezvoltat hidrops sau semne de afectare cardiacă în perioada prenatală. La 36 de săptămâni, s-a efectuat examinarea imagistică prin rezonanţă magnetică (IRM), în departamentul de radiologie şi imagistică al universităţii noastre, pentru confirmarea aspectelor ecografice şi estimarea prognosticului postnatal. Fătul (de sex feminin) a fost extras prin operaţie cezariană de urgenţă, la 37 de săptămâni, având o greutate de 2720 grame şi scorul Apgar 9. Postnatal au apărut semne de hipertensiune pulmonară şi complicaţii cardiace uşoare. Copilul a evoluat normal spontan, fără a fi supus niciunei intervenţii medicale. La vârsta de 5 ani, are o dezvoltare neurologică perfect normală. În ultimii 15 ani, diagnosticul prenatal al MAVG a fost facilitat de utilizarea modului Doppler color, crucial pentru diferenţierea acestei malformaţii de formaţiuni chistice localizate intracerebral pe linia mediană (MAVG fiind singura leziune caracterizată de flux sangvin intern). Examinarea IRM are un rol important în modularea managementului peripartum şi pe termen lung. În literatura de specialitate, nu am găsit niciun alt caz la care diagnosticul de MAVG să fie precizat prenatal şi evoluţia să fie spontan favorabilă, cu remisiune completă, în afara oricărei intervenţii medicale.Cuvinte Cheie
anevrism de venă Galenrezonanţă magneticăecografieDoppler colorremisiune spontanăIntroduction
Vein of Galen aneurysmal malformation (VGAM), also known as vein of Galen aneurysm, is a rare abnormality of the fetal cerebral vascular system, with an incidence of 1% of all fetal arteriovenous vascular abnormalities(1). Although usually isolated, cardiac and/or neurological abnormalities are often described(2), and these associations worsen the prognosis(3). It has also been reported that children with VGAM diagnosed later in childhood have a better prognosis than those presenting during the neonatal period(4,5).
Despite the prenatal diagnosis progress over the last decades, the prenatal diagnosis VGAM hardly increased. Jones et al. reported that only four cases among 13 in their case series were diagnosed prenatally(4). This may be because the third-trimester sonography is still not routinely performed in most units, many cases being detected in the neonatal period when the clinical symptoms occur. The malformation appears to be more frequent in male fetuses.
Two-dimensional (2D) real-time ultrasound (US) remains the main diagnostic method(6), while the Doppler technique elucidates the diagnosis by identifying the abnormal structure as a vascular malformation. For a secure diagnosis and a better assessment of fetal prognosis, complementary methods have been proposed: prenatal magnetic resonance imaging (MRI), postnatal MRI, computed tomography (CT), angiography, and CT angiography.
Although the US features occur usually in the third trimester of pregnancy, the current hypothesis holds that the pathologic process appears between the 6th and the 11th weeks of gestation(7,8). The clinical manifestations of VGAM seem to be related to the volume of arteriovenous shunting. In severe cases, signs of multisystem organ failure may develop in the prenatal period, due to the “steal of blood” phenomenon. In these cases, VGAM has a worse prognosis, especially if the brain injury develops prenatally.
In the neonatal period, the symptoms may be mild or extremely severe: macrocephaly, loud intracranial bruit and dilatation of orbital veins, seizures, hydrocephalus (caused by the obstruction of the aqueduct of Sylvius, through the dilated aneurysm), and subarachnoid hemorrhage.
Currently, two methods are used for treatment: endovascular transarterial embolization and direct surgical removal. Embolization is the first-line method used to treat VGAM, having better results. Unfortunately, the mortality remains as high as 50 percent, even in most specialized centers in the world(6,7).
Case report
A 24-year-old pregnant woman (gravida 1, para 1) was referred to our tertiary center (the Prenatal Diagnosis Unit of the County Emergency Clinical Hospital of Craiova) at 34 weeks and 5 days of gestation, for suspicion of a cerebral vascular malformation. The patient had no medical, obstetrical or family relevant history. The clinical exam was unremarkable. Previous ultrasound and clinical examinations showed normal results, including the fetal morphological survey and biometry.
At presentation, the ultrasound examination confirmed a singleton intrauterine pregnancy, in vertex presentation. The biometric parameters – the biparietal diameter (BPD), the head circumference (HC), the humerus length (HL), the abdominal circumference (AC), and the femur length (FL) – corresponded to the actual gestational age, as determined by the dating scan. The estimated fetal weight was 2620 grams, and the growth percentile – 54.5. The amniotic fluid index was borderline (4 cm) and the biophysical fetal score was 10. The spectral Doppler interrogation (umbilical artery and middle cerebral artery sites) showed normal values in terms of pulsatility index (PI) and peak systolic velocity (PSV). There were no signs of fetal hydrops, and the cardiac investigation showed no abnormalities, both in terms of anatomy and cardiac function.
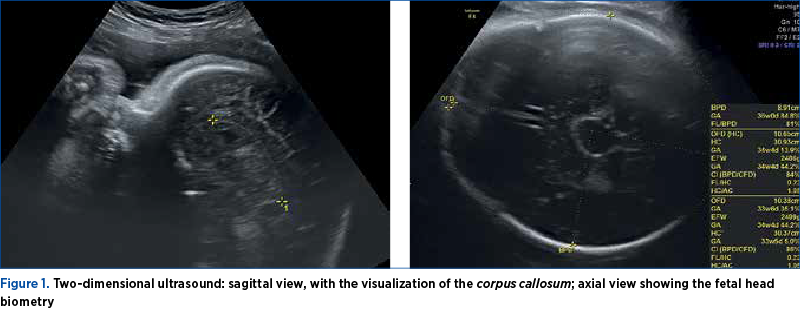
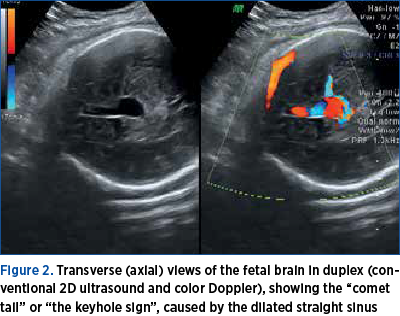
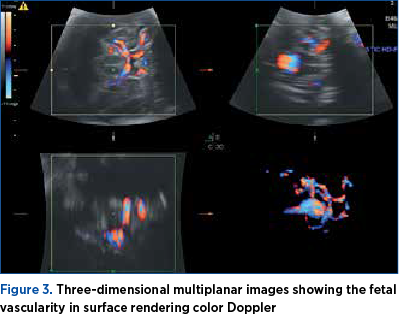
Doppler ultrasonography revealed turbulent arterial and venous flow within a hypoechogenic structure, located in the midline of the posterior part of the third ventricle, and the diagnosis of VGAM was suspected. The dilatation of the straight sinus was visualized, and the arterial flow in the cerebral venous sinuses was evident. The main bulk of feeders originated from the basilar artery and entered a straight sinus-like structure in the area posterior to the thalamus and midbrain (Figures 1 and 2). Three-dimensional multiplanar images also helped in determining the precise location of the malformation and the feeding vessels (Figure 3).
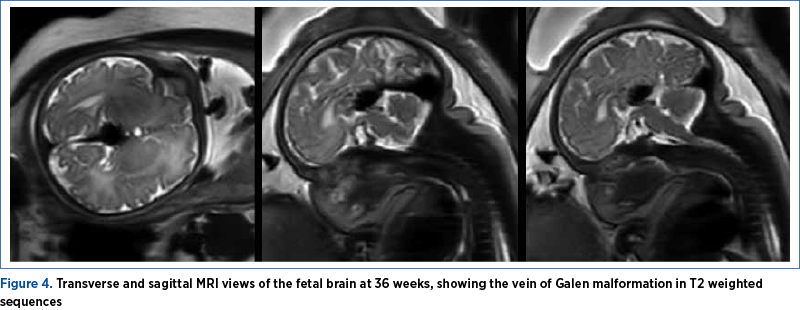
At 36 weeks of amenorrhea, an MRI was performed without fetal paralysis or sedation, on a 3-Tesla (3T) Philips Ingenia Wide Bore system. The scan confirmed the sonographic findings (Figure 3) and depicted prognosis markers of fetal VGAM: it ruled out the presence/the dilation of middle cerebral artery pseudofeeders in T2 weighted sequences. These are more recently described risk factors for further brain melting at birth, cardiac failure and pulmonary hypertension if found on MRI less than a month before birth. Basically, the MRI showed an otherwise normal brain parenchyma, with no associated cerebral structural anomalies (Figures 4 and 5).

The parents were referred for full pediatric specialist consultation. The multidisciplinary counseling process highlighted the extremely poor prognosis after birth, despite the isolated aspect of the malformation. The parents were warned regarding the difficult postnatal management, and the team described the main available strategies, underlining that endovascular transarterial embolization remains the first-choice option. The emotional impact of the repeated counseling sessions was huge, as the patient was carrying her first pregnancy and had a complete, high-quality prenatal care. The late diagnosis of a major congenital brain abnormality was almost devastating for the couple.
Serial follow-up scans were performed to monitor the cardiovascular status of the fetus, which remained stable. The fetus did not develop ventriculomegaly, increasing dilatation of the straight sinus, or brain lesions (other than VGAM). The cardiothoracic ratio (measured as cardiac area/thoracic area on a four-chamber axial view of the fetal thorax) remained normal. We did not find reversed flow in the aortic isthmus, tricuspid regurgitation, or any signs of heart failure (such as hydrops). The volume of the VGAM, calculated from the three diameters using the ellipsoid formula, varied around 10,000 mm3. We used 3D ultrasound equipment (Voluson E8) which provides volume calculation results comparable to those of MRI. The biophysical score remained complete.
At 37 weeks and 3 days, the rupture of membranes occurred, and a female neonate was delivered by caesarean section (weighing 2720 g, with an Apgar score of 9).
The diagnosis of vein of Galen malformation was confirmed by postnatal transfontanellar ultrasound. The neonatal period was complicated by mild cardiac complications and signs of pulmonary hypertension. Despite them, the neonate’s clinical condition remained good, and her development was normal in the early neonatal period.
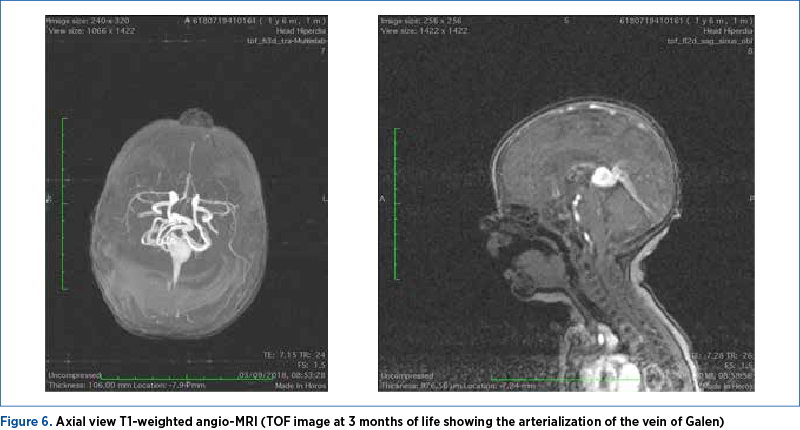
In the follow-up assessment at the age of 3 months old, the MRI showed a partial closure of the VGAM with a normal ventricular system (Figures 5 and 6). Time-of-flight (TOF) magnetic resonance angiography (MRA) was performed, as a noninvasive, non-contrast-enhanced technique. It provides contrast between vessels and stationary tissues by inducing blood inflow effect.
Subsequently, a close follow-up was performed, in multidisciplinary teams. The child’s clinical development remained normal, having appropriate behavioral acquisitions for any given age. No medical or surgical strategy was proposed.
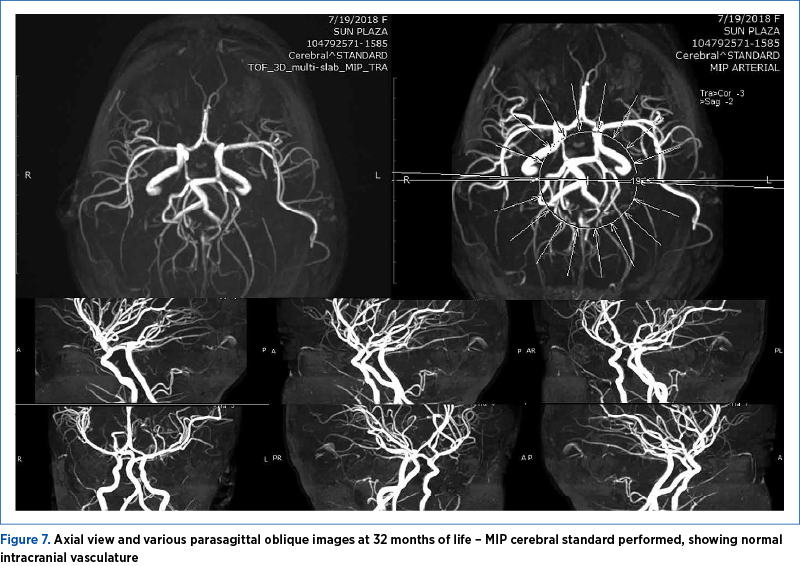
At 32 months of life, the angio-MRI showed a completely normal intracerebral vasculature (Figure 7). Maximum Intensity Projection (MIP) cerebral standard was performed (projecting the voxel with the highest attenuation value on every view throughout the volume onto a 2D image).
Currently, the 5-year-old child continues to be asymptomatic, and her neurodevelopment is completely normal.
Discussion
Vein of Galen aneurysmal malformation is a severe and complex vascular malformation, characterized by multiple arteriovenous shunts between the vein of Galen and the choroidal arteries. Several case series are described in the literature. The direct consequences are the “vascular steal effect” and the overload of the right heart. Often, a progressive heart failure occurs(9). Heart failure leads to progressive nonimmune hydrops, and this is the first detected feature on a routine ultrasound fetal examination in many cases. The secondary effects on the fetus are the cerebral mass effect and cerebral damage. The cerebral vascular steal phenomenon may lead to hydrocephalus, cerebral infarcts and leukomalacia(10). The spontaneously thrombosed vein of Galen aneurysm carries a better prognosis, but, unfortunately, this is an uncommonly reported event. Two main pathophysiological paths are involved in this event occurrence: the slow blood flow and an impediment to the venous outflow(11). Despite the extremely severe prognosis of this condition, our patient evolved toward complete spontaneous remission, having no medical and/or surgical management.
Despite the reported higher prevalence of male affected fetuses, in our case the fetus was female. All reports – including ours – emphasize the importance of the color Doppler technique(11-13) in the prenatal period, both in diagnosis and especially in the differential diagnosis of this malformation.
The introduction and the spread of 3D sonography in prenatal diagnosis have undoubtedly led to an improvement in understanding the spatial appearance of all intracranial structures. Newer papers stress the additional benefits of 3D color power angiography in describing also the angioarchitecture of this complex intracerebral vascular anomaly and in assessing the spatial relationship of blood vessels(14,15). We also found the 3D surface rendering color Doppler vessel mode informative in this case.
In fetuses with ultrasonographic findings consistent with VGAM, complementary MR imaging enables an accurate assessment of the condition of the brain parenchyma. Besides confirming the diagnosis, it allows a better evaluation of the lesion and aids the decision-making process. Moreover, MRI may help to diagnose recent necrotic lesions that may have escaped the ultrasound recognition. In the case presented, the MRI was crucial in documenting the natural history and the favorable changes in vasculature, facilitating the proposal of an expectance strategy.
Although the mode of delivery must be tailored to each context, elective caesarean delivery may lead to a better prognosis in selected cases. The protective caesarean section (and the postnatal treatment) is not indicated for a fetus/newborn with massive brain atrophy or intractable heart failure at birth, subsequent to the sudden diversion of flow through the malformation. We opted for the caesarean section protective extraction, in the context of an adequate-for-gestational-age fetus, having no signs of heart failure and – apart from the isolated vascular malformation – a confirmed normal brain structure, in the presence of spontaneous ruptured membranes.
Decisions regarding the course of pregnancy after the diagnosis, the mode of delivery, additional diagnostic procedures, and therapeutic measures should be adjusted in each case. The individual approach should be based on the time of detection of VGAM and the presence/absence of associated complications. The case we report may help in tailoring the prenatal and the postnatal counseling. Despite the notorious ominous prognosis of the VGAM(1,2,4,6-8), we documented the excellent spontaneous outcome of this particular baby.
Fetuses diagnosed with VGAM should undergo detailed extended neurosonography, echocardiography and brain MRI. The main risk factors associated with poor outcomes are a low overall neonatal score, major brain lesions (focal parenchymal changes, calcifications, tonsillar herniation, hemorrhage, necrosis, porencephaly, schizencephaly and micropolygyria), more than two groups of multiple arterial feeders(16), arterial steal, tricuspid regurgitation, and a VGAM volume ≥20,000 mm3(17). Our patient developed none of them. The intrauterine progression of the lesion – reported previously in roughly 10% of cases, and having the potential to deteriorate the prognosis(17) – was absent in our case.
Vein of Galen aneurysmal malformation remains a complex malformation, with an incompletely understood natural history. Perinatologists must exercise caution in parental counseling in these cases. It may be the case that a small subgroup of carefully selected patients without risk factors and clinically asymptomatic may have a good outcome even with conservative management and close follow-up.
Although rare, spontaneous thrombosis, with regression and complete disappearance of the VGAM, was reported previously in pediatric patients(18-21). Yet, to our best knowledge, there is no similar previously published case. The diagnostic was established in fetal life. In the case presented, the VGAM presented a complete remission in approximately 32 months, without any evidence of thrombosis and with no active treatment.
We consider this case informative. It underlines the fact that the medical team may become a source of higher-than-necessary anxiety. Although efforts have been made to image the brain early in pregnancy(22,23), central nervous system assessment remains challenging, as the cerebral structures evolve considerably and continuously during pregnancy, and the ultrasound features may become apparent much later than the initiation of the pathogenic process. This is the rationale of the third-trimester ultrasound screening(24).
Conclusions
We add to the literature the first case of vein of Galen aneurysmal malformation diagnosed in fetal life having a complete stable remission, approximately 32 months after birth. We found no evidence of thrombosis, and no active treatment was performed.
Corresponding author: Ştefania Tudorache, e-mail: stefania.tudorache@gmail.com
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Beucher G, Fossey C, Belloy F, Richter B, Herlicoviez M, Dreyfus M. Antenatal diagnosis and management of vein of Galen aneurysm: review illustrated by a case report. J Gynecol Obstet Biol Reprod (Paris). 2005;34(6):613–9.
-
Deloison B, Chalouhi GE, Sonigo P, Zerah M, Millischer AE, Dumez Y, Brunelle F, Ville Y, Salomon LJ. Hidden mortality of prenatally diagnosed vein of Galen aneurysmal malformation: retrospective study and review of the literature. Ultrasound Obstet Gynecol. 2012;40(6):652–8.
-
Mannaerts D, Muys J, Ramaekers P, Jacquemyn Y. Relapsing fetal bilateral hydrothorax, an isolated expression of a vein of Galen aneurysmal malformation. BMJ Case Rep. 2015;2015:bcr2014208384.
-
Jones BV, Ball WS, Tomsick TA, Millard J, Crone KR. Vein of Galen aneurysmal malformation: diagnosis and treatment of 13 children with extended clinical follow-up. AJNR Am J Neuroradiol. 2002;23(10):1717–1724.
-
Messori A, Polonara G, Salvolini U. Prenatal diagnosis of a vein of Galen aneurysmal malformation with fetal MR imaging study. AJNR Am J Neuroradiol. 2003;24(9):1923-5; author reply 1925.
-
Herghelegiu D, Ionescu CA, Pacu I, Bohîlţea R, Herghelegiu C, Vlădăreanu S. Antenatal diagnosis and prognostic factors of aneurysmal malformation of the vein of Galen A case report and literature review. Medicine (Baltimore). 2017;96(30):e7483.
-
Bohîlţea RE, Ţurcan N, Mihalea C, Dorobăţ B, Cinteză EE, Dan A, Mihai M, Dimitrade A, Boroş C, Dumitru M, Gobej I, Munteanu O, Cîrstoiu MM. Ultrasound Prenatal Diagnosis and Emergency Interventional Radiologic Therapy of Galen Aneurysmal Malformation in a Newborn. Maedica (Bucharest). 2016;11(4):334-340.
-
Marinaş MC, Mîndrilă I, Zorilă GL, Tudorache S, Căpitanescu RG, Zorilă MV, Iliescu DG. A Severe Case of Aneurysmal Malformation of the Vein of Galen. Curr Health Sci J. 2018;44(1):76-79.
-
Gailloud P, O’Riordan DP, Burger I, Levrier O, Jallo G, Tamargo RJ, Murphy KJ, Lehmann CU. Diagnosis and Management of Vein of Galen Aneurysmal Malformations. J Perinatol. 2005;25(8):542-51.
-
Wagner MW, Vaught AJ, Poretti A, Blakemore KJ, Huisman TA. Vein of Galen aneurysmal malformation: prognostic factors depicted on fetal MRI. Neuroradiol J. 2015;28:72–5.
-
Yan J, Gopaul R, Wen J, Li XS, Tang JF. The natural progression of VGAMs and the need for urgent medical attention: a systematic review and meta-analysis. J Neurointerv Surg. 2017;9(6):564-570.
-
Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: Embryonic and anatomical features relating to the pathogenesis of the malformation. Neuroradiology. 1989;31(2):109-28.
-
Pilu G, Falco P, Sandri F, Cocchi G, Ancora G, Bovicelli L. Differential diagnosis and outcome of fetal intracranial hypoechoic lesions: report of 21 cases. Ultrasound Obstet Gynecol. 1997;9(4):229–36.
-
Heling KS, Chaoui R, Bollmann R. Prenatal diagnosis of an aneurysm of the vein of Galen with three-dimensional color power angiography. Ultrasound Obstet Gynecol. 2000;15(4):333-6.
-
Sepulveda W, Vanderheyden T, Pather J, Pasquini L. Vein of Galen malformation: prenatal evaluation with three-dimensional power Doppler angiography. J Ultrasound Med. 2003;22(12):1395-8.
-
Geibprasert S, Krings T, Armstrong D, Terbrugge KG, Raybaud CA. Predicting factors for the follow-up outcome and management decisions in vein of Galen aneurysmal malformations. Childs Nerv Syst. 2010;26(1):35-46.
-
Paladini D, Deloison B, Rossi A, Chalouhi GE, Gandolfo C, Sonigo P, Buratti S, Millischer AE, Tuo G, Ville Y, Pistorio A, Cama A, Salomon LJ. Vein of Galen aneurysmal malformation (VGAM) in the fetus: retrospective analysis of perinatal prognostic indicators in a two-center series of 49 cases. Ultrasound Obstet Gynecol. 2017;50(2):192-199.
-
Kuroki K, Uozumi T, Arita K, Takechi A, Matsuura R, Fujidaka M. Spontaneous disappearance of an aneurysmal malformation of the vein of Galen. Neuroradiology. 1995;37(3):244-6.
-
Mohanty CB, Srinivas D, Sampath S. Spontaneous thrombosis of a vein of Galen malformation. Asian J Neurosurg. 2016;11(1):69.
-
Mahmoodi R, Habibi Z, Heidari V, Nejat F. Spontaneous regression and complete disappearance of the vein of Galen aneurysmal malformation. Childs Nerv Syst. 2016;32(4):593-8.
-
Kumar KK, Fornoff LE, Dodd RL, Marks MP, Hong DS. Spontaneous regression of a vein of Galen aneurysmal malformation in a pediatric patient: illustrative case. J Neurosurg Case Lessons. 2021;1(8):CASE20171.
-
Ungureanu DR, Drăguşin RC, Căpitănescu RG, Zorilă L, Ofiţeru AMI, Marinaş C, Pătru CL, Comănescu AC, Comănescu MC, Sîrbu OC, Vrabie MS, Dijmărescu LA, Streaţă I, Burada F, Ioana M, Drăgoescu AN, Iliescu DG. First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies. Brain Sci. 2023;13(1):118.
-
Ushakov F, Sacco A, Andreeva E, Tudorache S, Everett T, David AL, Pandya PP. Crash sign: new first-trimester sonographic marker of spina bifida. Ultrasound Obstet Gynecol. 2019;54(6):740-745.
-
Mărginean C, Calomfirescu M, Vlădăreanu,R, Mureşan D, Pleş L, Ceauşu I, Tudorache S, Iliescu D, Veduţa A, Pelinescu-Onciul D, Stamatian F. Ultrasound screening in the third trimester of pregnancy. Obstetrica şi Ginecologia. 2020;68(3):112.

Severe primary hypothyroidism-related hyperprolactinemia and secondary amenorrhea
Alexandra-Ioana Trandafir, Eugenia Petrova, Alexandru-Florin Florescu, Mara Carsote, Claudiu-Eduard Nistor, Aida Petca, Răzvan Petca, Mihai-Cristian Dumitraşcu, Florica Şandru
The most frequent cause of hypothyroidism in iodine-sufficient regions is chronic autoimmune thyroiditis, commonly referred to as ...
Conundrum of differentiated thyroid cancer amid pregnancy
Claudiu-Eduard Nistor, Anca-Pati Cucu, Eugenia Petrova, Aida Petca, Oana-Claudia Sima, Răzvan Petca, Florica Şandru, Mara Carsote
Primary thyroid malignancy embraces several types, namely differentiated (papillary and follicular), medullary and anaplastic, the differentiated forms representing the most frequent endocrine cancer(...
Uterine carcinosarcoma – case report
Roxana Cristina Drăguşin, Marina Dinu, Andreea-Denisa Hodorog, Andreea-Florentina Stăncioi-Cismaru, Ştefania Tudorache, Raluca-Maria Aron
Uterine carcinosarcoma (UCS) – also called malignant mixed mesodermal tumor or malignant mixed Müllerian tumor – has been described as a high-grade non-differentiated endometrial cancer with carcinoma...
Severe primary hypothyroidism-related hyperprolactinemia and secondary amenorrhea
Alexandra-Ioana Trandafir, Eugenia Petrova, Alexandru-Florin Florescu, Mara Carsote, Claudiu-Eduard Nistor, Aida Petca, Răzvan Petca, Mihai-Cristian Dumitraşcu, Florica Şandru
The most frequent cause of hypothyroidism in iodine-sufficient regions is chronic autoimmune thyroiditis, commonly referred to as ...
Conundrum of differentiated thyroid cancer amid pregnancy
Claudiu-Eduard Nistor, Anca-Pati Cucu, Eugenia Petrova, Aida Petca, Oana-Claudia Sima, Răzvan Petca, Florica Şandru, Mara Carsote
Primary thyroid malignancy embraces several types, namely differentiated (papillary and follicular), medullary and anaplastic, the differentiated forms representing the most frequent endocrine cancer(...