Reconsiderarea strategiei pentru pacientele cu răspuns ovarian scăzut. Ce ştim acum? La ce ne putem aştepta în viitor?
Reconsidering strategies for poor responder patients. What do we know now? What is reasonable to expect from the future?
Abstract
The strategy for the poor responder patients continues to represent one of the most challenging tasks for the clinicians. The reduced number of follicles reaching advanced stages of folliculogenesis may be due to atresia/cellular mitosis malfunction in the early stages of follicle development (exclusively controlled by paracrine factors) or to endocrine activity issues (especially of gonadotropins) in the final stages of development. Due to its complexity, the reproductive process inevitably entails a wide variety of possible pathologies. The aim of the present study was to review the currently available data on poor responder patients and to anticipate further steps for a better management of this condition.Keywords
poor respondersfollicleovaryIVFPOSEIDONRezumat
Stabilirea strategiei pentru pacientele „poor responders” continuă să rămână o mare provocare pentru clinicieni. Prezenţa unui număr redus de foliculi în fazele avansate ale foliculogenezi poate fi cauzată de anomalii în procesul de atrezie/diviziuni celulare (controlate exclusiv de factori paracrini) din fazele precoce ale foliculogenezei sau de probleme de natură endocrină (în special legate de expresia gonadotropinelor). Pornind de la complexitatea deosebită a procesului reproductiv, gama de posibile patologii este extrem de vastă. Scopul acestui studiu este de a evalua datele curente existente despre acest subiect, respectiv de a anticipa paşii viitori în direcţia ameliorării managementului acestor paciente.Cuvinte Cheie
poor respondersfoliculiovarIVFPOSEIDONIntroduction
Poor responders (PR) are a subgroup of patients with impaired response to ovarian stimulation during in vitro fertilization (IVF) procedures.
The special interest in this pathology stems mainly from the extremely high failure rates causing frustration to both the sterile couple and practitioners, as well as from the failure to increase the pregnancy rate significantly, despite the high cost incurred by the various schemes aimed at improving the biological response. The reported prevalence of this pathology varies greatly (9-34%), partly due to the heterogeneity of the sterile population, and partly to a lack of uniform nomenclature.
The history of this condition practically overlaps with the history of the modern period of assisted reproductive technology (ART). Thus, the first report of poor response to standard ovarian stimulation – documented by a level <300 pg/ml of estradiol at ovulation onset – was in 1983.
The first concrete step towards standardizing the definition was taken in 2011, in the form of what is referred to as the Bologna criteria. Thus, the European Society of Human Reproduction and Embryology (ESHRE) working group reported that, in order to define a poor response in IVF, at least two of the following three features must be present: (i) advanced maternal age or any other risk factor for poor ovarian response (more than 40 years old); (ii) a previous poor ovarian response (≤3 oocytes with a conventional stimulation protocol); and (iii) an abnormal ovarian reserve test (ORT) (i.e., antral follicle count [AFC] less than 5-7 follicles or anti-Müllerian hormone [AMH] below 0.5-1.1 ng/ml).
This definition was received with great enthusiasm by the entire scientific community but, unfortunately, its limitations soon became visible. Firstly, inaccurate parameters (AMH or AFC) are a source of unacceptable variation when assessing the effectiveness of different treatments. Secondly, this definition does not set the premises for identifying subgroups in the poor responder population – known to be very heterogeneous. The latter element in particular greatly limits the success of adjuvant therapies that should be adapted to the various particularities of the pathologies responsible for poor ovarian response.
Relatively recently, a new classification (POSEIDON) has been put forward, which meets the needs of clinicians to a far better extent. However, we are still far from a definite protocol in the case of this pathology. The aim of the present study was to review the currently available data on poor responder patients, in an attempt to anticipate the segments that require further analysis in order to customize therapies.
Etiology
Poor response to ovarian stimulation results from alterations occurring at different stages of folliculogenesis. Unfortunately, this is extremely difficult to explore, as the vast majority of the structures involved are of a paracrine nature. Although familial forms have also been described (5-15%), most are sporadic. It is generally accepted that more than 75% of all premature ovarian failure (POI) cases are idiopathic. Specialists favor the term premature ovarian failure to early menopause, because there have been numerous reports of cases of ovulation, and even pregnancy, in patients with an apparently exhausted ovarian reserve.
For didactic considerations, we discern three main categories of problems: congenital alteration of the primordial follicular reserve, alteration of the follicular recruitment or follicular atresia processes and, finally, functional impairment of the specialized cells in the final stages of folliculogenesis.
The medical conditions responsible for this pathology are genetic, infectious, iatrogenic or related to endocrine inducers.
Genetic disorders
There are syndromic diseases, due to mutations in certain genes involved in the development of germ cells or folliculogenesis (belonging to the X chromosome or autosomal) and genetic variations associated with less potent biochemical forms (polymorphisms).
Syndromic POIs are in most cases responsible for primary ovarian failure associating a number of other pathologies (Blepharophimosis-ptosis-epicanthus inversus syndrome [FOXL2], Perrault syndrome [HSD17B4, HARS2, LARS2 and CLPP], Marinesco-S SIL1), galactosemia [GALT], ovarian leukodystrophy, autoimmune polyendocrine insufficiency type 1, carbohydrate-deficient glycoprotein syndrome type 1, Cushing’s proximal symphalangism Albright’s hereditary osteodystrophy)(6-9). The share of these pathologies in premature ovarian insufficiency is extremely low.
Turner 45X syndrome is an established cause of primary ovarian failure, responsible for 3-5% of these cases. The absence of an X chromosome implies the absence of many genes, vital for ovarian function. In addition to problems with reproductive function, these patients frequently associate other serious conditions. For this reason, the option of sterility treatments – with oocyte donation and exogenous hormonal support – must be analyzed with great caution in order to avoid severe complications(7).
X isochromosome clinically presents with a picture similar to Turner syndrome, but with a lower frequency (1-2%). In this type of pathology, the centromere division is realized in the transverse plane (instead of the normal longitudinal division), resulting in pairs of arms with identical genes(7). Microdeletions on the X chromosome, unapparent to standard karyotyping, can in turn lead to ovarian failure.
Alteration of genes involved in the development of germ cells and folliculogenesis
Anomalies regarding the TGF superfamily
BMP 15 (located on the X chromosome) and GDF 9 (autosomal type) were the first explored due to their consistent role in the development of germ lines. Sporadic anomalies have been described, but cannot be attributed a significant role in POI. Subsequently, the focus shifted to inhibition translocation 46, XX, t (2; 15) (q32.3; q13.3), INHA genes (p.A257T)/activin and AMH, respectively, describing numerous polymorphisms with at least a theoretical role in dysfunctions of different degrees at the level of class IV, V and IV follicles(7,11,12).
Aromatase alterations have been investigated both in the context of POI and PCOS. There are described alterations of genes encoding aromatase 1303 C/T and 1310 G/A, responsible for hermaphroditism(6).
Alterations of genes responsible for estrogen/progesterone proteins or their receptors are responsible for profound dysfunctions in folliculogenesis, culminating with the reduction of follicular pool(8-10). There is also a very wide range of mutations/polymorphisms in FSH and LH receptors, an issue most intensely researched because of the fundamental implications these two hormones have in the final stages of folliculogenesis. Experimental studies were carried out on FSH, as driver of follicular development, and they proved that mutations which biochemically inactivate this hormone are equivalent to primary ovarian failure. In addition, a significant number of patients with suboptimal ovarian response have been shown to present polymorphisms (single nucleotide polymorphisms [SNPs] at positions 29, 307 and 680 have been extensively studied) that may be responsible for much higher doses of gonadotropins during ovarian stimulation. It was also agreed that LH inactivation, or the inactivation of its receptor (Arg 554 stop codon 554 TGA and Ser 616 → Tyr 616/Trp 8 Arg and Ile 15 Thr), is not responsible for premature menopause, but it may instead determine major dysfunctions in the final stages of folliculogenesis(8). For this reason, the association of LH (above normal biological levels) in ovarian stimulation in IVF procedures has become a common practice, especially in groups suspected of biologically inappropriate gonadotropin expression(9,11).
Inflammatory causes
There have been speculations on the possibility of a significant impact of Mumps oophoritis on the primordial follicular reserve (similar to the impact in men), but without convincing evidence. Conversely, the POI rate was found to be much higher in HIV-positive patients.
Autoimmune diseases are more commonly identified in the group of patients with POI. The disorders described in the immune behavior interfere on many levels with the phenomena of recruitment/follicular atresia in the early stages of folliculognesis, as well as with the processes occurring in the gonadotropin-dependent stage. Patients with such syndromes and conditions, ranging from APECED (autoimmune polyendocrine candidiasis ectodermal dystrophy), accountable for a 60% POI rate, to SLE, Sjögren syndrome, myasthenia gravis or rheumatoid arthritis, frequently display impaired folliculogenesis, which places them in the category of poor responders(7).
Endocrine disruptors
In recent years, considerable evidence has been provided on the significant impact of various substances from the external environment (food, environmental substances, chemicals) on cell expression. The term “endocrine disruptors” was first introduced by the U.S. Environmental Protection Agency (EPA) and translates as “an exogenous agent that interferes with synthesis, secretion, transport, metabolism, binding action, or elimination of natural blood-borne hormones that are present in the body and are responsible for homeostasis, reproduction and developmental process”. The mechanisms of action are extremely diverse and include: direct nuclear action (estrogen receptors, androgens), action at membrane level, interference with the oxidation-reduction systems, as well as epigenetic action – with gene expression alteration(14). That these factors play a role in folliculogenesis alteration is irrefutable, but the scope of the process is less clear, which is why it is currently an intensely researched aspect.
Iatrogenic causes
Pelvic surgery is frequently cited as a cause for poor ovarian response and finally for premature ovarian failure. The mechanisms involved range from direct destruction of ovarian tissue during ovarian cystectomy (especially in endometriosis) to postsurgical inflammatory alteration or reduced ovarian vascularization(12).
Chemotherapy treatment initiated for neoplasms or immune diseases can have a major impact on the function of the ovary, especially in the case of prolonged exposure to very aggressive agents. Cyclophosphamida, busulfan, procarbazine, chlorambucil or melphalan belong to the group of aggressive drugs, while metrotrexate, 5-flororiuracil, vincristine or bleomycin are considered to be much safer. These therapies interfere primarily with the growing cohorts of follicles, therefore a deep ovarian suppression induced by GnRh agonists is a consistent protective factor for the ovarian reserve(7,12).
Radiation therapy is generally accepted as a very toxic agent, primarily to the cohort of primordial follicles. High doses of radiation are documented to inflict consistent damage. When irradiation of the iliac ganglion areas is expected, fractionated, targeted doses and especially ovarian pexia are recommended in order to prevent functional castration(12).
Pathogenesis and classification
When considering the potential etiologic factors responsible for poor ovarian response, we can place the onset of this condition anytime during folliculogenesis. Consequences reflect especially upon follicle recruitment and, implicitly, the final oocyte yield, but also their quality – in the context of genetic issues or intrafollicular factors which alter oocyte maturation or the stability of oocyte chromosomes(2-4).
The reduced number of follicles reaching advanced stages of folliculogenesis may be due to atresia/cellular mitosis, malfunction in the early stages of follicle development (exclusively controlled by paracrine factors) or to endocrine activity issues (especially of gonadotropins) in the final stages of development(4). This distinction is obviously artificial since, in many instances, disorders acquired in early stages reflect in modified functional acquisitions responsible for the endocrine response. Moreover, even dysfunctions caused by an altered endocrine system may present several phenotypes.
As a model, the complexity of the FSH receptor (a member of the G proteins family) is enough to suggest the complex processes and large variety of phenotypical variations(13). The FSH receptor shares many connections to the LH, IGF 1 or GH receptors, assuming that, in certain conditions, certain types of dysfunctions may be corrected by using alternate pathways. The intracellular transmission network of the FSH receptor is complex, with a canonical line – the FSHR Gsa/cAMP/PKA signaling pathway, but also accessory pathways which interfere with networks mediated by G protein subtypes, Gi, Gq/11 and Gh or the receptor-associated proteins – beta-arrestins, and have very different functional implications(13). Overall, the activation of the FSH receptor leads to cellular differentiation mitosis, apoptosis, as well as to steroidogenesis or gametogenesis, depending on the duration and extent of exposure(13). This piece of information allows us to anticipate situations in which certain hormones (Gh, LH, androgens) may force alternative pathways capable of ensuring the rebalancing of follicular functions. At the same time, we can anticipate/speculate on the existence of more specific postreceptor alterations which may not be short-circuited through other hormones.
Oocyte quality is a crucial aspect in assisted reproduction, but our understanding of the intimate mechanisms of this feature is still vague. We assume that, behind poor quality oocytes leading to aneuploid embryos, there are especially issues related to the primary alteration of structures responsible for oocyte function or chromosomal integrity (intramitochondrion electron leakage and raised production of reactive oxygen species, decreased telomerase activity)(15). The identification of such problems is unfortunately retrospective, at present; there is no reliable diagnostic test. The quality of the intrafollicular environment was the main focus of many researchers in the context of a possible correlation between alterations of its components and poor oocyte quality. Unfortunately, a clear correlation could not be established even with intrafollicular steroid levels – it is well known that the main induction agent of the moment (letrozole) is responsible for producing much more increased intrafollicular androgen levels without altering the quality of the fertilization process(16).
The consternation of the clinician lies in the fact that the etiology of poor ovarian response is in 70-80% of the cases unknown. Moreover, 15-20% of the initially poor responder patients will respond normally to a second round of ovarian stimulation, thus assuming the first event as an accident occurring in a patient without ovarian pathology. Finally, many patients of advanced age depict a poor ovarian response given a natural phenomenon which assumes the alteration of cellular control systems and implicitly step out of the logic of therapeutic intervention.
Based on this data, the main problem the practician faces is to correctly identify poor responders or, better said, poor outcome patients, respectively to identify the vulnerable segment of folliculogenesis and consecutively the potential area of intervention. The only parameter with a reasonable estimative value regarding oocyte quality is patient age.
Two indices were proposed to assess follicular performance: FORT (follicular output rate) and FOI (follicle to oocyte index). A ratio of under 50% predicts a poor quality of follicular response by both indices and can be found in patients with unexpected poor ovarian response.
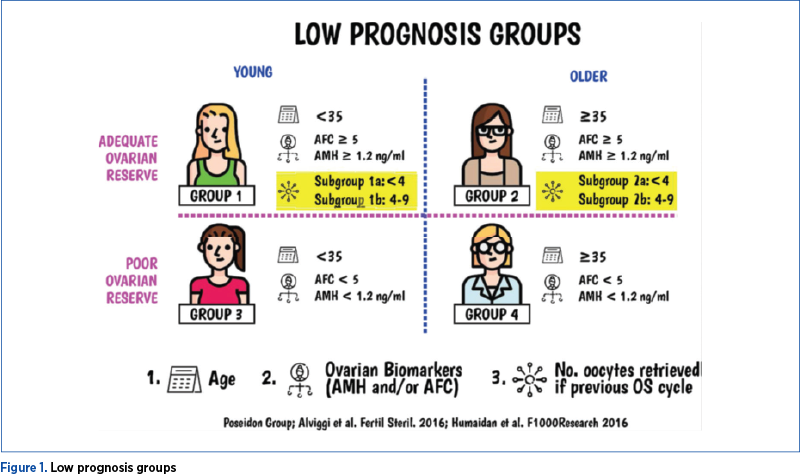
The first classification based on pathogenetic findings was proposed by the POSEIDON (Patient-Oriented Strategies Encompassing Individualized Oocyte Number) group and differentiates, on the one hand, two groups of patients with apparently normal ovarian reserve but weak response to ovarian stimulation, respectively two groups with poor ovarian reserve. The second major pillar of the classification is represented by age, with a threshold value of 35 years old. This classification assumes the existence of certain types of patients who exhibit mainly dysfunctions in early stages of folliculogenesis and other types of patients who exhibit only late follicular dysfunctions. Patient age was introduced as a variable to provide orientation regarding oocyte quality.
The POSEIDON classification was very well received by practitioners, since it allows a better adjusting of treatment doses according to individualized pathogenetic characteristics, as well as a more realistic estimation of pregnancy rates(17). The epidemiologic distribution on groups of patients according to this classification was the following: Group 1 – 5%, Group 2 – 35%, Group 3 – 10%, and Group 4 – 50%. Pregnancy rates were also very different, confirming the heterogeneity of poor responder patients(18).
Unfortunately, in the absence of sensitive parameters to evaluate the intrafollicular environment, it is very difficult to identify forms where early and late folliculogenesis stage dysfunctions coexist, respectively the clear identification of the gonadotrophin type which is not correctly biologically expressed. In the absence of functional mapping of mature ovarian follicles, it is impossible to refine the classification and the individual adjustment of therapeutic regimens.
Treatment
Pituitary suppression regimens
Poor responders were, par excellence, the ideal candidates for exploring diverse variants of pituitary suppression. Thus, over time, long GnRh agonist (AgGnRh) protocol, short GnRh agonist protocol, ultrashort Ag GnRh, GnRh antagonist protocol, or “priming” formula with oestrogen or progesterone were examined.
The long Ag GnRh protocol aims to prolong the period before stimulation in order to widen the selectable cohort and to increase the follicular synchronization. As a disadvantage, in case of excessive prolongation, it may induce a deep blockage of natural FSH production which might be responsible for follicular atresia.
The agonist GnRh short protocol aims to exploit equally the initial stimulating effect of agonist in the first part of the cycle and the suppressive effect on hypophysis in the second part of the cycle. It has the advantage of maximizing the body’s resources and thus reducing the exogenous need for FSH. It is blamed for a poor pituitary control, with a relatively important rate of premature luteinisation.
The antagonist protocol has a good pituitary control, without the need for deep endogenous suppression of FSH. In addition, the priming with oestrogen in the lutheal phase can reduce/block intercyclic FSH growth, and thus improve follicular synchronization.
Most of the currently available data are provided by studies on poor responder patients as a whole, disregarding subgroup particularities. These studies reported better results when using the long agonist and the antagonist protocol for suppression(19-21). However, more recent studies, which differentiated between the various poor responder patient groups (according to the POSEIDON classification), have reported a slight advantage of the long agonist protocol in early follicular phase in young patients (below 35 years old – types 1 and 3) compared to the antagonist protocol(22). This advantage translated into a higher number of oocytes collected, a higher rate of transferred embryos, lower ET cancellation rate and a higher pregnancy rate. By contrast, no differences were identified in groups 2 and 4 as far as the two protocols were concerned(22).
Type and dose of gonadotropins
There has been much controversy about the stimulus doses of poor responders. Beyond the immediate impulse to force follicular stimulation, it is necessary to take into account the negative impact that these high doses can exert on follicles with quasi-abnormal resistance, on the endometrium and, last but not least, the financial burden of gonadotropins massive dose increments. There is an agreement assumed by most practitioners and validated by ESHRE recommendations to impose a limit of 300 IU based on studies documenting the absence of benefits beyond this dose(18). Relatively recently, the idea of lowering this dose below 150-225 IU (the Optimist study)(23) was advanced, but most specialists considered that the authors of that study did not judiciously select patients of the poor responders type.
For the time being, good clinical practice guidelines recommend a maximum dose of 300 IU for POSEIDON groups 3 and 4 and lower values (150-225) for POSEIDON groups I and II, which can be still increased to the maximum value if other detrimental factors are encountered (smokers, endometriosis, FSH receptor resistance)(24).
There are no data to support a preference for purified FSH over recombined FSH(24).
Adjuvant treatment
The administration of androgens to poor responder patients has solid documentation. Even though no spectacular results are reported, the usefulness of these preparations is obvious – at least, for certain types of patients.
The intimate mechanism of action is not clarified, but the major role of androgens in the final stages of folliculogenesis is well known. The presence of androgen receptors in specialized cells and oocytes starting from classes IV-V of follicles, associated with the major impact on FSH expression, intimate connections with LH and, lastly, the recruitment-type action in PCOS pathology are arguments in favor of including this class of substances in the care of poor responders. However, the existing data require a nuanced use of androgens, assuming the existence of ovarian dysfunction in which excess androgens are either useless or detrimental(25,26). In addition, considering the physiology of folliculogenesis, we must accept that androgens have a positive effect only at the time of follicular recruitment, and less so in the final follicular maturation phases. The ESHRE guide recommends the administration of testosterone or of its precursor DHAS to POSEIDON groups 3 and 4 patients, assuming that androgen production by the thecal cells is insufficient(18).
LH administration
The synergistic action of LH with FSH is well documented and targets both steroidogenesis and oocyte maturation. The addition of LH in IVF procedures was initially proposed for patients with suboptimal response(27). The biological rationale relies on the observation that certain patients present a low level of LH (particularly in the long AgGnRh protocol) or a decreased LH biological action due to certain polymorphisms of LH or LH receptor. Several studies reported significant benefits in terms of collected oocytes but also on the pregnancy rate in certain subgroups of poor responder patients treated with LH(27,28). Guidelines for good medical practice recommend LH supplementation in groups with an unexpected poor response – POSEIDON groups 1, 2 and for patients older than 35 years of age(18,29).
GH administration has been proposed in the treatment of poor responders, primarily due to structural similarities with IGFI and its synergistic action with FSH. Somewhat surprisingly beyond the steroidogenetic action – the increase in androgen levels, there was also an apparent direct effect on oocytes materialized by increasing the quality of embryos. Most studies confirm a certain beneficial effect of GH in terms of embryo quality and the rate of pregnancy(30-32). However, the wide use of GH is still limited due to the cost of the treatment and also because of some concerns regarding its safety in certain patients with other conditions. Guidelines for good medical practice recommend these preparations for POSEIDON groups 3 and 4(18).
Q10 coenzyme administration
The enzymatic systems involved in redox processes are a topic of great interest in fertility diseases. The intracellular accumulation of reactive oxygen species (ROS) is frequently associated with elderly patients and causes dysfunction at all functional levels of the cell. The examination of the possible pathogenesis lines responsible for the disorders of this system obviously starts with the mitochondria – the most abundant organelles in oocytes, responsible for over 85% of ROS production. Coenzyme Q10 is known to be an essential structure in mitochondrial functionality. Coenzyme Q10 administration has been shown to be useful in cardiovascular disease by limiting the peroxidation of membrane lipids and DNA oxidation. In the absence of stratified studies – administration to poor responders –, promising results were obtained, however insufficient to be introduced into current practice(33). The groups of patients who seem to benefit the most from this treatment include older patients and patients with poor oocyte quality, despite young age(18).
Double stimulation in the same ovarian cycle
The concept of double ovarian stimulation emerged as a result of studies focused on the physiology of follicular recruitment. Thus, recent data question the classical theory of a single recruitment episode and bring arguments both in favor of a multistage recruitment (the waves theory) and a continuous recruitment (continuous recruitment theory)(34). According to these studies, the number and quality of oocytes obtained by stimulation in the luteal phase did not differ significantly from those obtained by standard stimulation. Under these conditions, double stimulation – during the follicular and the luteal phases – would allow for the collection of a larger number of oocytes in a shorter time(35-37). However, it presents several drawbacks, namely: a significant rate of cancelled cycles in the luteal phase, exposure to high doses of gondatotropins and, last but not least, the absence of randomized studies to evaluate the long-term safety and efficacy of this strategy. Currently, this is considered an option only in patients with oncological pathology and in patients with a significantly diminished ovarian reserve (POSEIDON group 4), with careful circumspection(18).
Natural cycle IVF/mild stimulation
This approach is reserved for patients with extremely low ovarian reserves in which it is expected that, regardless of the aggressiveness of stimulation, the number of oocytes collected will be very small. Under these conditions, a minimal stimulation (clomiphen/letrozole) or even a cycle without stimulation will allow a massive reduction in expenses and also a much greater comfort for the patient, without the pregnancy rate being much lower(38).
Conclusions
Due to its complexity, the reproductive process inevitably entails a wide variety of possible pathologies. The therapeutic strategies rely primarily on an accurate description of the type of pathology, as well as on an accurate determination of the patient’s biological resources. At present, the POSEIDON classification allows practitioners to differentiate only to a certain extent among the types of obstacles they must address. It goes without saying that the improvement of medical performance is closely related to the ability to describe and access the follicular space as easily as possible.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Ferraretti AP, La Marca A, Fauser BC, Tarlatzis B, Nargund G, Gianaroli L; ESHRE working group on Poor Ovarian Response Definition. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011;26(7):1616-24.
- Keay SD, Liversedge NH, Mathur RS, Jenkins JM. Assisted conception following poor ovarian response to gonadotrophin stimulation. Br J Obstet Gynaecol. 1997;104:521–7.
- Patrizio P, Vaiarelli A, Setti L, Tobler KJ, Shoham G, Leong M, Shoha Z. How to define, diagnose and treat poor responders? Responses from a worldwide survey of IVF clinics. Reprod Biomed. 2015 Jun;30(6):581-92.
- Surcel M, Stamatian F, Micu R. Infertile patients with a poor ovarian response during IVF procedures (poor responders) – Definition and Pathogenesis, Obstetrica şi Ginecologia. 2014;1(ian-martie):27-38.
- Alviggi C, Andersen CY, Buehler K, Conforti A, De Placido G, Esteves SC, Fischer R, Galliano D, Polysoz NP, Sunkara SK, et al. A new more detailed of low responders to ovarian stimulation: From a poor ovarian response to a low prognosis concept. Fertil Steril. 2016 Jun;105(6):1452-3.
- Ito Y, Fisher CR, Conte FA, et al. Molecular basis of aromatase deficiency in an adult female with sexual infantilism and polycystic ovaries. Proc Natl Acad Sci USA. 1993;90:11673–11677.
- Rafique S, Sterling E, Lawrence N. A new approach to primary ovarian insufficiency. Obstet Gynecol Clin N Am. 2012;39:567–586.
- Laan M, Grigorova M, Huhtaniemi IT. Pharmacogenetics of follicle-stimulating 618 hormone action. Curr Opin Endocrinol Diabetes Obes. 2012 Jun;19(3):220-7.
- Laue L, Chan W-Y, Hsueh AJW, Kudo M, Hsu SY, Wu S-M, Blomberg L, Cutler GB Jr. Genetic heterogeneity of constitutively activating mutations of the human luteinizing hormone receptor in familial male-limited precocious puberty. Proc Natl Acad Sci USA. 1995;92:1906-1910.
- Latronico AC, Anasti J, Arnhold IJ, Rapaport R, Mendonca BB, Bloise W, et al. Brief report: testicular and ovarian resistance to luteinizing hormone caused by inactivating mutations of the luteinizing hormonereceptor gene. N Engl J Med. 1996;334(8):507–12.
- Lamminen T, Huhtaniemi I. A common genetic variant of luteinizing hormone; relation to normal and aberrant pituitary-gonadal function. Eur J Pharmacol. 2001;414(1):1–7.
- Vujovic S. Aetiology of premature ovarian failure. Menopause Int. 2009;15:72-75.
- Ulloa-Aguirre A, Zarinan T. The Follitropin Receptor: Matching Structure and Function. Mol Pharmacol. 2016;90:596-608.
- Fowler PA, Bellingham M, Sinclair KD, Evans NP, Pocar P, Fischer B, et al. Impact of endocrine-disrupting compounds (EDCs) on female reproductive health. Mol Cell Endocrinol. 2012;355(2):231–9.
- Hansen KR, Knowlton NS, Thyer AC, et al. A new model of reproductive aging: The decline in ovarian non-growing follicle number from birth to menopause. Hum Reprod. 2008;23:699–708.
- Garcia-Velasco JA, Moreno L, Pacheco A, Guillen A, Duque L, Requena A, Pellicer A. The aromatase inhibitor letrozole increases the concentration of intraovarian androgens and improves in vitro fertilization outcome in low responder patients: a pilot study. Fertil Steril. 2005;84:82–87.
- Poseidon Group (Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number); Alviggi C, Andersen CY, Buehler K, Conforti A, De Placido G, Esteves SC, Fischer R, Galliano D, Polyzos NP. A new more detailed stratification of low responders to ovarian stimulation: From a poor ovarian response to a low prognosis concept. Fertil Steril. 2016;105:1452–1453
- Abu-Musa A, Haahr T, Humaidan P. Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations. Int J Mol Sci. 2020;21:1–20.
- Lambalk CB, Banga FR, Huirne JA, Toftager M, Pinborg A, Homburg R, van der Veen F, van Wely M. GnRH antagonist versus long agonist protocols in IVF: a systematic review and meta-analysis accounting for patient type. Hum Reprod Update. 2017 Sep 1; 23(5):560-579.
- Errázuriz J, Drakopoulos P, Pening D, Racca A, Romito A, De Munck N, et al. Pituitary suppression protocol among Bologna poor responders undergoing ovarian stimulation using corifollitropin alpha: does it play any role? Reprod Biomed Online. 2019;38:1010–7.
- Huang M-C, Tzeng S-L, Lee C-I, Chen H-H, Huang C-C, Lee T-H, et al. GnRH agonist long protocol versus GnRH antagonist protocol for various aged patients with diminished ovarian reserve: a retrospective study. PLoS One. 2018 Nov 7;13(11):e0207081.
- Li F, Ye T, Kong H, Li J, Hu L, Jin H, Su Y, Li G. Efficacies of different ovarian hyperstimulation protocols in poor ovarian responders classified by the POSEIDON criteria. Aging (Albany NY). 2020 May 31;12(10):9354–9364.
- van Tilborg TC, Torrance HL, Oudshoorn SC, Eijkemans MJC, Koks CAM, Verhoeve HR, et al. Individualized versus standard FSH dosing in women starting IVF/ICSI: an RCT. Part 1: The predicted poor responder. Hum Reprod (Oxford England). 2017;32(12):2496–505.
- La Marca A, Blockeel C, Bosch E, Fanchin R, Fatemi HM, Fauser BC, et al. Individualized FSH dosing improves safety and reduces iatrogenic poor response while maintaining live-birth rates. Hum Reprod. 2018;33:982–3.
- Nagels HE, Rishworth JR, Siristatidis CS, Kroon B. Androgens (dehydroepiandrosterone or testosterone) for women undergoing assisted reproduction. Cochrane Database Syst Rev. 2015;11:CD009749 10.1002/14651858.CD009749
- Polyzos NP, Davis SR, Drakopoulos P, Humaidan P, De Geyter C, Vega AG, et al. Testosterone for poor ovarian responders: lessons from ovarian physiology. Reprod Sci. 2016;25:980–2.
- Bosch E, Labarta E, Crespo J, et al. Impact of luteinizing hormone administration on gonadotropin-releasing hormone antagonist cycles: an age-adjusted analysis. Fertil Steril. 2011;95:1031–1036.
- Alviggi C, Pettersson K, Longobardi S, Andersen CY, Conforti A, De Rosa P, Clarizia R, Strina I, Mollo A, De Placido G, et al. A common polymorphic allele of the LH beta-subunit gene is associated with higher exogenous FSH consumption during controlled ovarian stimulation for assisted reproductive technology. Reprod Biol Endocrinol. 2013;11:51.
- Alviggi C, Conforti A, Esteves SC, Andersen CY, Bosch E, Bühler K, et al. Recombinant luteinizing hormone supplementation in assisted reproductive technology: a systematic review. Fertil Steril. 2018;109:644–64.
- Bachelot A, Monget P, Imbert-Bolloré P, Coshigano K, Kopchick JJ, Kelly PA, et al. Growth hormone is required for ovarian follicular growth. Endocrinology. 2002;143:4104–12.
- Duffy JM, Ahmad G, Mohiyiddeen L, Nardo LG, Watson A. Growth hormone for in vitro fertilization. Cochrane Database Syst Rev. 2010;1:CD000099 10.1002/14651858.CD000099.
- Norman RJ, Alvino H, Hull LM, Mol BW, Hart RJ, Kelly T-L, et al. Human growth hormone for poor responders: a randomized placebo-controlled trial provides no evidence for improved live birth rate. Reprod Biomed Online. 2019;38:908–15.
- Gat I, Blanco Mejia S, Balakier H, Librach CL, Claessens A, Ryan EA. The use of coenzyme Q10 and DHEA during IUI and IVF cycles in patients with decreased ovarian reserve. Gynecol Endocrinol. 2016 Jul;32(7):534-7.
- Baerwald AR, Adams GP, Pierson RA. Ovarian antral folliculogenesis during the human menstrual cycle: a review. Hum Reprod Update. 2012;18:73–91.
- Moffat R, Pirtea P, Gayet V, Wolf JP, Chapron C, de Ziegler D. Dual ovarianm stimulation is a new viable option for enhancing the oocyte yield when the time for assisted reproductive technnology is limited. Reprod Biomed Online. 2014;29:659–61.
- Vaiarelli A, Cimadomo D, Trabucco E, et al. Double stimulation in the same ovarian cycle (DuoStim) to maximize the number of oocytes retrieved from poor prognosis patients: a multicenter experience and SWOT analysis. Front Endocrinol (Lausanne). 2018;9:317.
- Alsbjerg B, Haahr T, Elbaek HO, Laursen R, Povlsen BB, Humaidan P. Dual stimulation using corifollitropin alpha in 54 Bologna criteria poor ovarian responders – a case series. Reprod Biomed Online. 2019;38(5):677–682.
- Drakopoulos P, Romito A, Errázuriz J, et al. Modified natural cycle IVF versus conventional stimulation in advanced-age Bologna poor responders. Reprod Biomed Online. 2019;39:698–703.

Managementul rezultatelor anormale în urma screeningului pentru cancer de col uterin în timpul sarcinii
Ioana Cristina Rotar, Suzana Mariam Chaikh-Sulaiman, Antonia Mihaela Levai, Monica-Mihaela Cîrstoiu, Daniel Mureşan
În prezent, s-a înregistrat o tendinţă de creştere a detectării cancerelor ginecologice în cursul sarcinii, în principal din cauza...
Impactul fibroamelor asupra ratei fertilităţii. Management chirurgical şi rezultate obstetricale
Andreea Elena Dumitru, Tamara Maria Pătraş, Nicolae Gică, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu
Fibroamele uterine sunt cea mai frecventă tumoră benignă la femeile de vârstă reproductivă. Atunci când sunt simptomatice, se mani...
Cât de des recomandaţi suplimentarea cu vitamină D în sarcină? Ce trebuie să ştie obstetricienii despre vitamina D şi sarcină
Bianca Danciu, Ana Maria Alexandra Stănescu, Ana-Maria Cioti, Nastasia Serban, Alexandra Toma, Anca A. Simionescu
Vitamina D (calciferolul), măsurată prin 1,25-dihidroxivitamina D în serul matern, este importantă pentru dezvoltarea unităţii fet...
Managementul rezultatelor anormale în urma screeningului pentru cancer de col uterin în timpul sarcinii
Ioana Cristina Rotar, Suzana Mariam Chaikh-Sulaiman, Antonia Mihaela Levai, Monica-Mihaela Cîrstoiu, Daniel Mureşan
În prezent, s-a înregistrat o tendinţă de creştere a detectării cancerelor ginecologice în cursul sarcinii, în principal din cauza...
Impactul fibroamelor asupra ratei fertilităţii. Management chirurgical şi rezultate obstetricale
Andreea Elena Dumitru, Tamara Maria Pătraş, Nicolae Gică, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu
Fibroamele uterine sunt cea mai frecventă tumoră benignă la femeile de vârstă reproductivă. Atunci când sunt simptomatice, se mani...