What do we know about imaging in pregnancy?
Ce ştim despre imagistica în sarcină?
Abstract
When planning to undertake paraclinical investigations in pregnancy that involve ionizing radiation, a specialist should always think of the most appropriate test or intervention that carries minimal risks to both mother and fetus. A fetal radiation dose well below 50 mGy will be obtained in most cases. The risks of lethality, genetic damage/epigenetic change, teratogenicity, growth impairment or sterility are almost inexistent at this dose. Looking at the literature, one can see that old papers have shown an increased risk for malignancy, but this hasn’t been proven by the more recent studies. The linear no-threshold rule has been contradicted by recent scientific data with regards to malignancy risk. The same applies for iodinated mediums used as contrast. With the recent advances in medicine and the high expectations from the pregnant population, it has become obvious that in our days imaging in pregnancy is something that is frequently used. It is important to know what investigations can be performed in pregnancy with minimal effects on the fetus. A review of the literature has shown that the effects of a radiation below 50 mGy are likely to be negligible in pregnancy, with minimal or none risks in regards to the fetus. Magnetic resonance imaging (MRI) is the investigation of choice when it comes to pregnancy. The informed consent should always be sought and, when possible, the written consent.Keywords
ionizing imagingpregnancy risksradiationRezumat
Imagistica cu radiaţii ionizante poate fi necesară în timpul sarcinii şi impune o evaluare a celei mai adecvate şi mai sigure modalităţi imagistice, care va furniza informaţiile relevante în raport cu riscurile potenţiale pentru mamă şi făt. În majoritatea cazurilor se va obţine o doză de radiaţii fetale cu mult sub 50 mGy. Riscurile de letalitate, leziuni genetice/modificare epigenetică, teratogenicitate, tulburări de creştere sau sterilitate sunt aproape inexistente la această doză. În privinţa literaturii de specialitate, se poate observa că lucrările vechi au arătat un risc crescut de malignitate, dar acest fapt nu a fost dovedit de studiile mai recente. Regula liniară fără prag a fost contrazisă de date ştiinţifice recente cu privire la riscul de malignitate. Acelaşi lucru este valabil şi pentru mediile iodate folosite drept contrast. Odată cu progresele recente în medicină şi cu aşteptările mari de la femeile însărcinate, a devenit evident că în zilele noastre imagistica în timpul sarcinii este frecvent utilizată. Este important de ştiut ce investigaţii pot fi efectuate în sarcină cu efecte minime asupra fătului. O revizuire a literaturii de specialitate a arătat că efectele unei radiaţii sub 50 mGy sunt probabil neglijabile în timpul sarcinii, cu efecte minime sau fără consecinţe în ceea ce priveşte fătul. Imagistica prin rezonanţă magnetică (IRM) este investigaţia de elecţie atunci când vine vorba de sarcină. Consimţământul informat trebuie obţinut întotdeauna şi, atunci când este posibil, consimţământul scris.Cuvinte Cheie
imagistică cu radiaţii ionizanteriscuri în sarcinăradiaţiiIntroduction
Many conditions in pregnancy require noninvasive paraclinical examinations. These kinds of tests should never replace a good clinical examination, a thorough physical exam, and physicians should know what radiological test is best suited for the patient. Our lack of understanding of safety for a certain investigation can be dangerous and can lead to an undesirable result, and the worst-case scenario, when harm to the patient can have consequences, especially if there is a delay in making the right diagnosis. This review is aimed at presenting the benefits and risks of various imaging techniques in pregnancy and to highlight the appropriate techniques to image women presenting with common medical symptoms.
Ionizing radiation
This imaging techniques include X-rays and computed tomography. These imaging techniques that expose the fetus to ionizing radiation may be required in pregnancy to help with decision making and for establishing a diagnosis. Sometimes, a fetus may be exposed to radiation by accident, especially in the first trimester. During pregnancy, there are data to suggest that a fetus is exposed to a background radiation of 1 mGy(1).
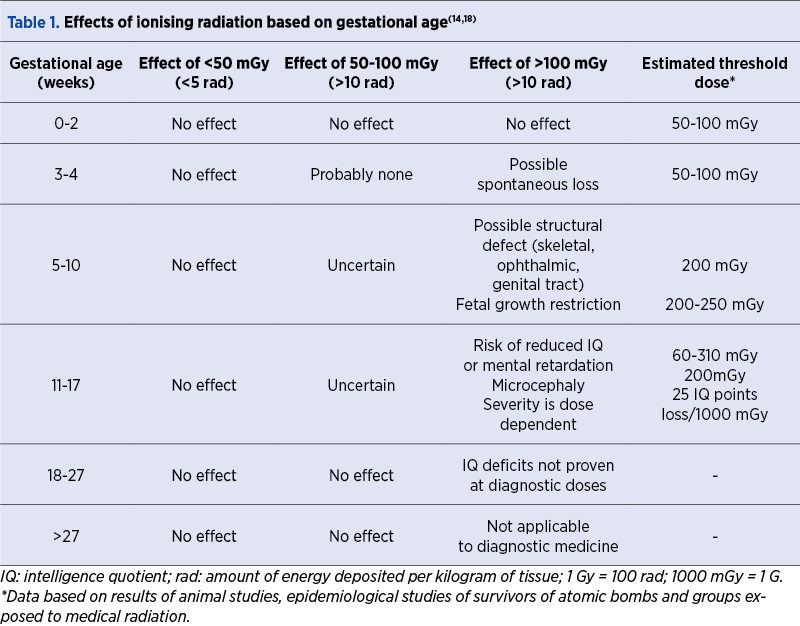
Any physician should know that electromagnetic waves can affect the human tissue in two ways: through stochastic and deterministic effects(2). The first effect – occurrence of malignancies – can appear at any radiation dose, as a result of cellular damage following a germline mutation(3). We do not know what would be the cut-off value for this effect not to take place. There is a strong correlation between the stochastic effect and the increased risk of childhood malignancy(4). The second effect involves the loss of cellular function because of cell death, and it results from very high radiation doses. Aneuploidies can occur as a result of such a destructive injury at cellular level(3). As a consequence, major risks include fetal structural defects (skeletal, ophthalmic and genital tract anomalies), placental injuries (small babies with growth restriction) and brain lesions (microcephaly, intellectual or developmental disability)(1). In Table 1, we have summarized some of the potential consequences of imaging in pregnancy at different gestations and the radiation doses thresholds.
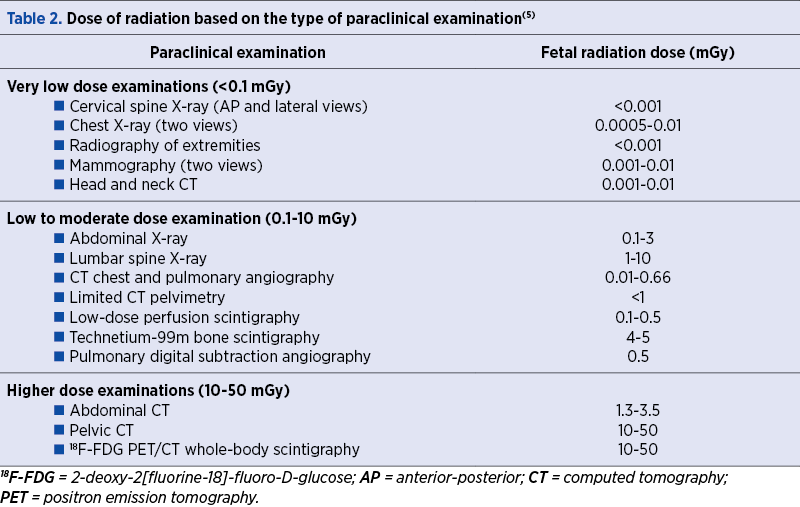
Fetal radiation doses for common radiological investigations are presented in Table 2. The exact fetal exposure dose vary with maternal characteristics like gestational age, maternal Body Mass Index and parameters of the machine, such as image acquisition indices(5).
Radiography
X-rays are used to investigate various symptoms and causes of a disease. Given the minimal risks to the fetus and potential delayed diagnosis, there should be no delay in performing such an investigation in pregnancy, the same as for non-pregnant women(5).
Computed tomography (CT)
In a review of 5270 examinations, performed in more than 3000 women in a 10-year period, Lazarus et al.(6) noted an annual increase of 25% in the use of CT in the time period studied. The indications for the use of CT in pregnancy are numerous, including assessing injuries following trauma(7), diagnosing pulmonary embolism(8,9), investigating gastrointestinal complications (acute abdomen, bowel obstruction)(10,11) and malignancy(12,13).
The ALARA (“as low as reasonably achievable”) principle is well known by most physicians when it comes to the use of radiation(14). The International Commission on Radiological Protection(15) recommends that “imaging radiation must be applied at levels as low as reasonably achievable, while the degree of medical benefit must counterbalance the well-managed levels of risk”. Shielding techniques in our times have significantly reduced the dose of ionizing radiation; for example, the fetal radiation dose received during mammography is in the order of 0.001-0.01 mGy(5). The use of lead shielding can further reduce this risk by an additional 50%(13).
During computed tomography, the fetal exposure to radiations depends on a number of factors: the anatomical region of interest, machine set-up, X-ray tube voltage, tube current and number of image acquisitions(16). As a general rule, the fetal radiation dose is at a maximum when the fetus is captured directly in the X-ray beam – for example, when using abdominal-pelvic CT. For head and chest CT, the fetus is exposed to scatter radiation, which confers a low-dose radiation exposure(16). Radiologists should need to plan very well a scan before the actual procedure takes place, monitor the length of time for the procedure, and check the quality of images collected to minimize the exposure time(17).
The use of intravenous contrast agents may improve the diagnostic accuracy of CT by enhancing soft tissue and vascular structures(18). The most commonly used intravenous contrast media contain iodine, and this carries a small risk of maternal side effects, like nausea, vomiting, flushing and anaphylactoid reactions(19). Iodinated contrast medium can easily cross the placenta and enter the placental circulation or pass directly into the amniotic fluid from the fetus; however, animal studies have not revealed any teratogenic effects from its use(20).
Ultrasound
Ultrasound quickly became a relied upon and widely used imaging technique in pregnancy, being first introduced by Professor Ian Donald in Glasgow(21). Initially, ultrasound imaging was assumed to be safe in pregnancy. The early ultrasound machines used relatively low output settings. Color flow, power Doppler or three-dimensional or four-dimensional imaging of the fetus were introduced at a much later stage(22). Thermal effects on tissue temperature and mechanical effects resulting in tissue cavitation were regarded as potential harmful to the mother or fetus. Thermal injury can potentially affect the fetal central nervous system; animal studies have demonstrated associations with neural tube defects, arthrogryposis, disorders of muscle tone, miscarriage and fetal growth restriction(23). The risk of temperature elevation is lowest in B-mode imaging and is higher with color Doppler and spectral Doppler imaging(24). Cavitation refers to the development of gas bubbles in tissues exposed to ultrasonic vibration(25). These bubbles can cause inertial (transient) or non-inertial (stable) cavitation effects. Inertial cavitation effects have been shown to cause genetic damage in vitro(25), while in vivo studies of non-inertial effects have remained inconclusive(26). There is a general consensus that no significant effects of ultrasound occur, unless fetal exposure is prolonged for more than 60 minutes(23).
Magnetic resonance imaging (MRI)
Magnetic resonance imaging does not use ionizing radiation and permits the visualization of deep soft tissue structures(24). MRI is useful for assessing a variety of medical conditions – for example, encephalopathy syndrome, thrombosis of venous plexuses(27), acute abdomen(10), inflammatory bowel disease(28), and suspected placenta accreta spectrum disorders(29). Antenatal MRI is increasingly used to further evaluate structural fetal anomalies, including cranial lesions (agenesis of the corpus callosum, ventriculomegaly, posterior fossa anomalies, gyral or sulcation pattern)(30), neural tube defects, pulmonary sequestrations, congenital diaphragmatic hernia and heart anomalies (tumors or large vessels anomalies)(29).
In obstetrics, many times, performing an MRI can be challenging due to fetal movements and lack of trained personnel. However, MRI has several advantages over antenatal ultrasound. This imaging modality has improved image quality, and imaging of the fetal head allows the direct visualization of the entire brain. Additional limitations of sonography, resulting from reduced amniotic fluid, breech or transverse presentation and lack of visualization from the ossifying head bones, can be overcome using this type of investigation(29). Other maternal complications include phobia and back or abdominal pain, particularly at term, when it is difficult to lie in a certain position for a long period of time(31,32).
MRI does expose the fetus to a magnetic field far greater than that of Earth (50 lT), but there are no side effects from ionizing radiation because it doesn’t use this(5). The possible virtual risks are: firstly, a teratogenic risk as a result of fetal exposure to the static magnetic field and cell destruction due to quick movement, proliferation and differentiation; secondly, tissue heating due to exposure to intermittent radiofrequency fields; thirdly, hearing damage, given the fetal exposure to high-gradient electromagnetic fields, needed in order to acquire good quality images(33). The American College of Radiology stipulates clearly that MRI is safe to use in pregnancy, but we should always balance risks versus benefits(34). The consequences of first-trimester MRI on fetal growth, pregnancy loss and optic nerve damage have not been proven in studies performed in humans(32). Strizek et al.(35) evaluated the effects of exposure to MRI in pregnancy (1.5 T) on fetal growth and neonatal hearing function in a group of newborns at low risk for congenital hearing impairment or congenital deafness (n=751). The median gestational age at first MRI exposure was 37 weeks of gestation (range: 16-41+6 weeks). None of the exposed neonates had hearing loss or impairment. In terms of growth, both cohorts had similar mean percentile (50.6%) and controls (48.4%; p=0.22)(35).
Contrast agents
In a large retrospective cohort study conducted by Ray et al.(36), the long-term safety of MRI was evaluated in more than a million matched maternal-child pairs. MRI was carried out either in the first trimester of pregnancy or with gadolinium at any time during pregnancy. The MRI exposure was 3.97 per 1000 pregnancies. Comparing first-trimester MRI (n=1737) with no MRI (n=1,418,451), there was no significant difference in morbidity and mortality rate between the exposed and unaffected groups (19 versus 9844; adjusted relative risk [RR] 1.68; 95% CI; 0.97-2.90). When MRI was performed in the first trimester, there was no increase in the risk of structural defects, malignancies, affected hearing or vision. Inflammatory skin diseases and other autoimmune diseases were more likely in the group exposed to MRI with gadolinium contrast (123 versus 384,180 births; adjusted HR 1.36; 95% CI; 1.09-1.69). In regards to other pregnancy outcomes, the stillbirth and neonatal death rate was higher in the gadolinium-exposed group (adjusted RR 3.70; 95% CI; 1.55-8.85). Given the available evidence, it is therefore recommended that gadolinium contrast be avoided in pregnancy, unless the benefits clearly outweigh the possible risks to the fetus.
There is no requirement to cease breastfeeding following the administration of gadolinium to a lactating woman, as it has low lipid solubility, with less than 0.04% measurable in breast milk(37).
Nuclear medicine imaging
The following investigations are included: pulmonary ventilation/perfusion (V/Q scan), thyroid, bone and renal scans(18). Technetium-99m is a commonly used isotope in V/Q scanning to diagnose pulmonary embolism (PE) in pregnancy. It has a half-life of approximately 6 hours. In general, V/Q scans result in a fetal radiation exposure below 5 mGy(19). A normal chest radiograph can be used as a surrogate marker of ventilation and half-dose perfusion scans could be considered to reduce the exposure time. In contrast, radioactive iodine (iodine-131), for the assessment of thyroid pathology, readily crosses the placenta, has a half-life of eight days and may cause fetal hypothyroidism, especially if used after 10-12 weeks of gestation. When considering imaging of the thyroid gland, technetium-99m is the isotope to use, but it shouldn’t be used routinely(18,19).
Imaging of malignancy during pregnancy may warrant investigation with a positron emission tomography (PET) scan(38). In pregnant women with cancer, the use of PET imaging has been debated, because it uses radioactive-labelled tracers, therefore increasing the risk of exposing the fetus to radiation. The most commonly used radiotracer is 2-deoxy-2-[fluorine-18] fluoro-D-glucose (18F-FDG). The highest exposure risk is in the first trimester, but the total absorbed dose of radiation is well below the threshold for non-cancer health effects throughout pregnancy(39). Studies in the second and third trimesters of pregnancy also indicate that the fetal radiation dose from 18F-FDG administration is low. When medically indicated in pregnant women, 18F-FDG PET scanning should not be withheld for fear of excessive radiation exposure to the fetus(40).
Common investigations
Calf pain/swelling
First-line imaging for suspected deep venous thrombosis (DVT) is with compression duplex ultrasound, and women should remain on therapeutic anticoagulation until the diagnosis is ruled out. If the ultrasound is negative and a high level of clinical suspicion remains, anticoagulant treatment should be stopped, but the ultrasound should be repeated on days 3 and 7(8).
Shortness of breath
Women presenting with signs or symptoms of an acute pulmonary embolism (PE) should be investigated as a matter of urgency. Initial investigations should include an electrocardiogram and a chest radiograph. In those presenting with a suspected PE, but without symptoms and signs of deep vein thrombosis, a V/Q scan or a CT pulmonary angiogram (CTPA) should be performed. A Cochrane review looked at the diagnostic accuracy of CTPA and V/Q scanning for the diagnosis of pulmonary embolism and has shown that the median frequency of inconclusive results was 5.9% for CTPA and 4% for V/Q scanning(9).
CTPA is many times preferred to V/Q imaging, due to disponibility, relatively low fetal radiation exposure and superior identification of other pathologies, including chest infection (5-7%) and pulmonary oedema (2-6%). A downside of CTPA is the delivery of up to 20 mGy of radiation to maternal breast tissue, so that the risk of breast cancer is slightly increased. Delivery of 10 mGy radiation to a woman’s breast before the age of 35 years old is expected to increase her lifetime risk of developing breast cancer by 13.6% above that of the general population(41).
V/Q scanning may withhold an increased childhood malignancy risk when compared with CT owing to a slightly higher fetal radiation dose. The International Commission on Radiological Protection(15) estimates an increased risk of fatal childhood cancer up to the age of 15 years old following in utero radiation exposure of 0.006% per mGy, which equates to a risk of 1 in 17,000 per mGy.
Abdominal pain
The most common causes of non-obstetric pain in pregnancy are appendicitis and cholecystitis(10). Ultrasound and MRI (without contrast) are the primary imaging modalities recommended for the evaluation of abdominal pain in pregnancy; however, abdominal radiography can be used(10). Ultrasound is a useful first-line investigation to image the appendix, bowel, hepatobiliary tree, renal tract and adnexa. In the setting of active infection or inflammation, particularly inflammatory bowel disease, MRI can also help identify bowel obstruction, fistulas or abscess formation(10).
Headache
Headaches remain the most frequent reason for referral to an outpatient neurology clinic(27). Most headaches are benign, but they should be urgently investigated. In many cases, headaches are a primary disorder: migraine, tension-type headache and cluster headache. However, clinicians must be alert to causes of secondary headache in pregnancy, including preeclampsia, posterior reversible encephalopathy syndrome, reversible cerebral vasoconstriction syndrome and acute arterial hypertension. Other possible causes for secondary headache in pregnancy include cerebral venous thrombosis, intracranial hemorrhage, subarachnoid hemorrhage, ischemic stroke, pituitary adenoma and malignancy(27).
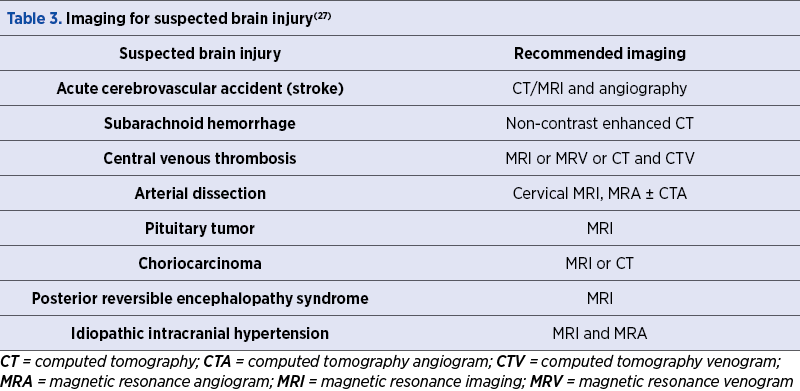
Women with focal neurological deficits or signs of raised intracranial hypertension should be referred for urgent intracranial imaging after a thorough history taking and clinical evaluation(42). Table 3 summarizes the intracranial imaging techniques that can be used to investigate the underlying causes of headache in pregnancy(27).
Breast mass
Women of young age still have a very high risk of dying before they turn 55 years old because of breast cancer (a lifetime risk of 1 in 9)(12). When there is a suspicion of malignancy, the suspicious looking breast should be scanned and a tissue biopsy must be taken. Samples should be sent for histology, and if malignancy is identified, mammography is advised to evaluate the spread of the disease, visualize small calcifications and assess the contralateral breast. The sensitivity of mammography during pregnancy is thought to be between 78% and 90% in women with clinical abnormalities. Both breasts should always be evaluated(38). Mammography exposes the tissue to a radiation dose in the order of 0.001-0.01 mGy.
Conclusions
It is important to know which investigations can be performed in pregnancy with minimal effects on the fetus. A review of the literature has shown that the effects of a radiation below 50 mGy are likely to be negligible in pregnancy, with minimal or no consequences in regards to the fetus. MRI is the investigation of choice when it comes to pregnancy. The informed consent should always be sought and, when possible, the written connect, as well.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- REFERENCES
- Patel SJ, Reede DL, Katz DS, Subramaniam R, Amorosa JK. Imaging the pregnant patient for nonobstetric conditions: algorithms and radiation dose considerations. Radiographics. 2007;27(6):1705-22.
- Wang PI, Chong ST, Kielar AZ, Kelly AM, Knoepp UD, Mazza MB, et al. Imaging of pregnant and lactating patients: part 1, evidence-based review and recommendations. American Journal of Roentgenology. 2012;198(4):778-84.
- Wieseler KM, Bhargava P, Kanal KM, Vaidya S, Stewart BK, Dighe MK. Imaging in pregnant patients: examination appropriateness. Radiographics. 2010;30(5):1215-29.
- Wakeford R. The risk of childhood leukaemia following exposure to ionising radiation – a review. Journal of Radiological Protection. 2013;33(1):1.
- Tremblay E, Thérasse E, Thomassin-Naggara I, Trop I. Quality initiatives: guidelines for use of medical imaging during pregnancy and lactation. Radiographics. 2012;32(3):897-911.
- Lazarus E, DeBenedectis C, North D, Spencer PK, Mayo-Smith WW. Utilization of imaging in pregnant patients: 10-year review of 5270 examinations in 3285 patients, 1997-2006. Radiology. 2009;251(2):517-24.
- Raptis CA, Mellnick VM, Raptis DA, Kitchin D, Fowler KJ, Lubner M, et al. Imaging of trauma in the pregnant patient. Radiographics. 2014;34(3):748-63.
- Thomson A, Greer I. Royal College of Obstetricians and Gynaecologists. Thromboembolic disease in pregnancy and the puerperium: acute management. Green-top Guideline no. 37b. London, RCOG, 2019.
- van Mens TE, Scheres LJ, de Jong PG, Leeflang MM, Nijkeuter M, Middeldorp S. Imaging for the exclusion of pulmonary embolism in pregnancy. Cochrane Database Syst Rev. 2017;1(1):CD011053.
- Woodfield CA, Lazarus E, Chen KC, Mayo-Smith WW. Abdominal pain in pregnancy: diagnoses and imaging unique to pregnancy. AJR Am J Roentgenol. 2010;194(6 Suppl):WS14-30.
- van der Woude CJ, Metselaar HJ, Danese S. Management of gastrointestinal and liver diseases during pregnancy. Gut. 2014;63(6):1014-23.
- Royal College of Obstetricians and Gynaecologists. Pregnancy and breast cancer. Green-top Guideline no. 12. London, RCOG, March 2011.
- Shachar SS, Gallagher K, McGuire K, Zagar TM, Faso A, Muss HB, et al. Multidisciplinary Management of Breast Cancer During Pregnancy. Oncologist. 2017;22(3):324-34.
- American College of Radiology. ACR-SPR practice parameter for imaging pregnant or potentially pregnant adolescents and women with ionizing radiation. Resolution no. 39, 2018.
- The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007;37(2-4):1-332.
- Goldberg-Stein SA, Liu B, Hahn PF, Lee SI. Radiation dose management: Part 2, estimating fetal radiation risk from CT during pregnancy. American Journal of Roentgenology. 2012;198(4):W352-W6.
- Wagner LK, Lester RG, Saldana LR, Hobbs B. Exposure of the pregnant patient to diagnostic radiations: a guide to medical management. Canadian Association of Radiologists Journal. 1998;49(6):426.
- Committee Opinion No. 723. Guidelines for Diagnostic Imaging During Pregnancy and Lactation. Obstet Gynecol. 2017;130(4):e210-e6.
- Adam A, Dixon AK, Grainger RG, Allison DJ. Grainger and Allison’s diagnostic radiology: a textbook of medical imaging. Churchill-Livingstone, 2015.
- Webb JA, Thomsen HS, Morcos SK. The use of iodinated and gadolinium contrast media during pregnancy and lactation. Eur Radiol. 2005;15(6):1234-40.
- Oakley A. The history of ultrasonography in obstetrics. Birth. 1986;13(1):8-13.
- Barnett SB, Ter Haar GR, Ziskin MC, Rott H-D, Duck FA, Maeda K. International recommendations and guidelines for the safe use of diagnostic ultrasound in medicine. Ultrasound in Medicine & Biology. 2000;26(3):355-66.
- Joy J, Cooke I, Love M. Is ultrasound safe? The Obstetrician & Gynaecologist. 2006;8(4):222-7.
- Committee Opinion No. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation [published correction appears in Obstet Gynecol. 2018 Sep;132(3):786]. Obstet Gynecol. 2017;130(4):e210-e216.
- Barnett S, Ter Haar G, Ziskin M, Nyborg W, Maeda K, Bang J. Current status of research on biophysical effects of ultrasound. Ultrasound in Medicine & Biology. 1994;20(3):205-18.
- Shankar H, Pagel PS, Warner DS. Potential adverse ultrasound-related biological effects: a critical review. The Journal of the American Society of Anesthesiologists. 2011;115(5):1109-24.
- Negro A, Delaruelle Z, Ivanova T, Khan S, Ornello R, Raffaelli B, et al. Headache and pregnancy: a systematic review. The Journal of Headache and Pain. 2017;18(1):1-20.
- Stern MD, Kopylov U, Ben-Horin S, Apter S, Amitai MM. Magnetic resonance enterography in pregnant women with Crohn’s disease: case series and literature review. BMC Gastroenterology. 2014;14:1-9.
- Wataganara T, Ebrashy A, Aliyu LD, Moreira de Sa RA, Pooh R, Kurjak A, et al. Fetal magnetic resonance imaging and ultrasound. J Perinat Med. 2016;44(5):533-42.
- Tee LM, Kan EY, Cheung JC, Leung WC. Magnetic resonance imaging of the fetal brain. Hong Kong Med J. 2016;22(3):270-8.
- Glenn O, Barkovich A. Magnetic resonance imaging of the fetal brain and spine: an increasingly important tool in prenatal diagnosis, part 1. American Journal of Neuroradiology. 2006;27(8):1604-11.
- Patenaude Y, Pugash D, Lim K, Morin L, Bly S, Butt K, et al. RETIRED: the use of magnetic resonance imaging in the obstetric patient. Journal of Obstetrics and Gynaecology Canada. 2014;36(4):349-55.
- De Wilde J, Rivers A, Price D. A review of the current use of magnetic resonance imaging in pregnancy and safety implications for the fetus. Progress in Biophysics and Molecular Biology. 2005;87(2-3):335-53.
- Expert Panel on MR Safety, Kanal E, Barkovich AJ, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging. 2013;37(3):501-530.
- Strizek B, Jani JC, Mucyo E, De Keyzer F, Pauwels I, Ziane S, et al. Safety of MR Imaging at 1.5 T in Fetuses: A Retrospective Case-Control Study of Birth Weights and the Effects of Acoustic Noise. Radiology. 2015;275(2):530-7.
- Ray JG, Vermeulen MJ, Bharatha A, Montanera WJ, Park AL. Association between MRI exposure during pregnancy and fetal and childhood outcomes. JAMA. 2016;316(9):952-61.
- American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice. Committee Opinion No. 656: Guidelines for Diagnostic Imaging During Pregnancy and Lactation. Obstet Gynecol. 2016;127(2):e75-e80.
- de Haan J, Vandecaveye V, Han SN, Van de Vijver KK, Amant F. Difficulties with diagnosis of malignancies in pregnancy. Best Practice & Research Clinical Obstetrics & Gynaecology. 2016;33:19-32.
- Zanotti-Fregonara P, Laforest R, Wallis JW. Fetal radiation dose from 18F-FDG in pregnant patients imaged with PET, PET/CT, and PET/MR. Journal of Nuclear Medicine. 2015;56(8):1218-22.
- Takalkar AM, Khandelwal A, Lokitz S, Lilien DL, Stabin MG. 18F-FDG PET in pregnancy and fetal radiation dose estimates. Journal of Nuclear Medicine. 2011;52(7):1035-40.
- Remy-Jardin M, Remy J. Spiral CT angiography of the pulmonary circulation. Radiology. 1999;212(3):615-36.
- Jarvis S, Dassan P, Piercy CN. Managing migraine in pregnancy. BMJ. 2018;360:k80.

The importance of chronic endometritis and dysbiosis in implantation failure in IVF cycles
Laurenţiu-Mihai Dîră, Roxana Cristina Drăguşin, Constantin-Cristian Văduva, George Lucian Zorilă, Rodica Daniela Nagy, Ştefan-Gabriel Ciobanu, Elena-Iuliana-Anamaria Berbecaru, Iuliana-Alina Enache, Gabriel Dominic Iliescu
We often face in vitro fertilization cycles in which embryo implantation does not occur despite the apparent exclusion of other ma...
Cystic hygroma presenting as an isolated malformation – case report and literature review
Ioana Păvăleanu, Alexandra Popa, Ana-Maria Haliciu
Nuchal translucency (NT) is the ultrasound observation of subcutaneous fluid accumulation at the back of the fetal neck. When this accumulation becomes excessively enlarged, it can lead to nuchal edema, which is referre...
The role of the sentinel lymph node mapping in the actual treatment of endometrial cancer
Anca Hashemi, Andrei Manu, Cristina-Maria Iacob, Mihaela-Arina Banu, Cătălin Bogdan Coroleucă, Ciprian Andrei Coroleucă, Elvira Brătilă
In high-income countries, endometrial cancer is perhaps the most prevailing gynecological malignancy, with an incidence rate risin...
Is the mesh necessary for the treatment of female urinary stress incontinence?
Mihaela-Arina Banu, Andrei Manu, Cristina-Maria Iacob, Anca Hashemi, Cătălin Bogdan Coroleucă, Ciprian Andrei Coroleucă, Elvira Brătilă
The International Continence Society (ICS) defines stress urinary incontinence (SUI) as ‘‘the complaint of involuntary leakage on ...
Anatomic landmarks in radical hysterectomy
Cristina-Maria Iacob, Andrei Manu, Mihaela-Arina Banu, Anca Hashemi, Diana Soare, Cătălin Bogdan Coroleucă, Ciprian Andrei Coroleucă, Elvira Brătilă
Cervical cancer provides one of the few examples of controversial treatment management throughout medical history. Radical hysterectomy was first described and performed by Clark and Reis in 1895(1). ...