Aspecte CT şi IRM în mielomul multiplu cu compresie medulară – o suită de cazuri
CT and MRI aspects in multiple myeloma with spinal cord compression – a suite of cases
Abstract
Spinal involvement of multiple myeloma (MM) can cause spinal cord compression (SCC), which is an oncologic emergency manifested by pain and potential paralysis, and often leads to disability, having a profound impact on prognosis. Magnetic resonance imaging (MRI) or computed tomography (CT) of the entire spine must be performed immediately if this complication is suspected. We present some cases of patients diagnosed with MM who were hospitalized in the hematology department accusing sudden paraplegia, sensory disturbance or severe lumbar pain. They were rapidly investigated by CT or MRI exams in order to achieve a complete lesions report in complicated forms of MM, with medullary or radicular compression.Keywords
multiple myelomaspinal cord compressionmagnetic resonance imagingcomputed tomographyRezumat
Implicarea coloanei vertebrale în mielomul multiplu (MM) poate cauza compresia măduvei spinării (CMS), care este o urgenţă oncologică manifestată prin durere, paralizie şi duce adesea la dizabilităţi, având un impact profund asupra prognosticului. Imagistica prin rezonanţă magnetică (IRM) sau tomografia computerizată (CT) a întregii coloanei vertebrale trebuie efectuate în urgenţă dacă se suspectează această complicaţie. Prezentăm câteva cazuri de pacienţi diagnosticaţi cu MM care au fost spitalizaţi în secţia de hematologie, acuzând brusc paraplegie, tulburări senzoriale sau dureri lombare severe, evaluate în regim de urgenţă prin CT sau IRM în scopul de a realiza un bilanţ complet al leziunilor de MM, în formele complicate cu compresie medulară sau radiculară.Cuvinte Cheie
mielom multiplucompresia măduvei spinăriiimagistică prin rezonanţă magneticăcomputer-tomografieIntroduction
Multiple myeloma (MM) is the most common hematological malignancy which involves the spine(1-6). Spinal involvement of MM may generate infiltrative and large lesions of spinal cord compression (SCC)(2). Most cord-compression lesions occur due to a pathological fracture of the involved vertebral body or extension of a vertebral body MM lesion, with or without neurological impairment(2,3). SCC – which is an oncologic emergency that can cause pain and potential paralysis, occurring in approximately 5-24% of all patients with MM – often leads to disability and has a profound impact on prognosis(2).
For the detection of bone involvement and its aggressive forms in patients diagnosed with MM, we aimed to review the CT and MRI techniques and illustrate the imaging characteristics in complicated forms with medullary or radicular acute compression(5-11).
Method
We reviewed 30 cases of patients, with ages between 39 and 79 years old, suffering from spinal cord or nerve root compression, suddenly installed, caused by MM lesions, who were investigated in emergency by CT and MRI exams. The clinical symptoms of these patients were dominated by severe back pain with irradiation at the costal grille, marked functional impotence, lumbar pain, and persistent paresthesia in the lower limbs or walking disorders(1-6).
CT exams were achieved using a multidetector (MD) CT non-enhanced acquisitions and in particular cases after iodinated non-ionic contrast intravenous injection, followed by multiplanar reconstructions in sagittal and coronal plane using a bone window, depending on the particularities of each case(12). Despite a number of advantages, the conventional CT uses higher doses of radiation, and for this reason the whole-body low-dose (WBLD) CT has begun to be the most widely used imaging method in patients diagnosed with MM, because it uses a lower tube voltage (kV) and current (mAS) to reduce the energy delivered to the patient(3). Low-dose CT is given without i.v. contrast, and it is a unique spiral acquisition including the skull, cervical compartment, the thoracic, abdominal and pelvic regions, proximal humerus, and femoral bones, with a field of view (FOV) set at about 400 mm (adjusted to individual patients during examination planning)(4,11). The diagnostic images can be achieved with parameters such as 120 kV, <70-90 mAs, dose modulation, and iterative reconstruction(4,11). Slice thickness was set at 1 mm and slice increment was set at 0.8 mm (slice increment smaller than thickness was used to avoid step artefacts on secondary coronal/sagittal reconstructions)(4,11). Two sets of axial images were reconstructed from the raw data obtained during scanning: for bone assessment using sharp kernel and for soft tissue assessment using soft kernel(4,10,11). From every set of axial images, secondary coronal and sagittal reconstructions were generated using slice thickness of 1 mm and slice increment of 1 mm(4).
MRI evaluation of the spine in patients with MM and spinal cord compression included: T1 SE and T2 FSE-weighted images (wi), T1 in/out of phase, STIR sequence, diffusion wi (DWI), non-enhanced and enhanced T1-weighted SE with and without fat suppression (FS) sequences. T1 SEwi is an anatomical sequence used in the sagittal plan to prove the presence of spinal lesion and highlights lesions with lipomatous content, hemorrhages, or osteolytic lesions. STIR sequence is realized in sagittal or coronal plan to prove the presence of spinal lesions. T2-FSE wi in sagittal/axial plan shows the level and degree of compression of the cord by a myelomatous mass, detects lesions within the cord itself, and also used in coronal plan highlights the paravertebral extension of the mass. DWI, usually realized in axial plan, highlights myeloma lesions, and it is also applied in the post-therapeutic lesions evaluation. Non-enhanced and enhanced T1 SE wi with fat suppression sequences are realized in sagittal plan and are necessary to assess the loco-regional extension of the lesion. T1 in-phase/opposed-phase imaging is realized in sagittal/coronal or axial plan and may be useful in differentiating acute benign compression fractures from malignant infiltration and pathologic fractures and to delineate lipomatous bone conversion. Furthermore, it may be an early indicator of response to treatment after radiation therapy to the spine and additional research could be performed. Especially for the follow-up of treated MM, it is useful to perform the same T1 weighted sequence with FS non-enhanced, T1 with TE in-phase and out of phase and DWI(5-8).
Results
All patients included in this study were diagnosed with MM and presented neurological complications of this disease. Some of them are presented in Table 1, with their imaging aspects and complications.
The CT findings in multiple myeloma consist of punched-out lytic lesions, expansile lesions with soft tissue masses, diffuse osteopenia, fractures and, rarely, osteosclerosis(8). CT exam can also depict significant soft tissue abnormalities (e.g., disk herniation, ligamentous degenerative hypertrophy, epidural lesions or collections)(8). The most important limitation of this technique remains the inability to provide accurate information on spinal cord lesions and ligamentous injury(9).
On MRI exam, typical myeloma lesions involve the bone marrow and have low signal intensity on T1-weighted images, a high signal intensity on T2-weighted sequences and STIR image, and generally show water restriction on DWI sequences and gadolinium-enhancement in the affected bone and in the epidural mass(8). Tumors arising from the vertebral osseous structures can cause SCC, even in the absence of a pathologic fracture, in the case of extraosseous neoplastic overgrowth and invasion of the epidural space(9).
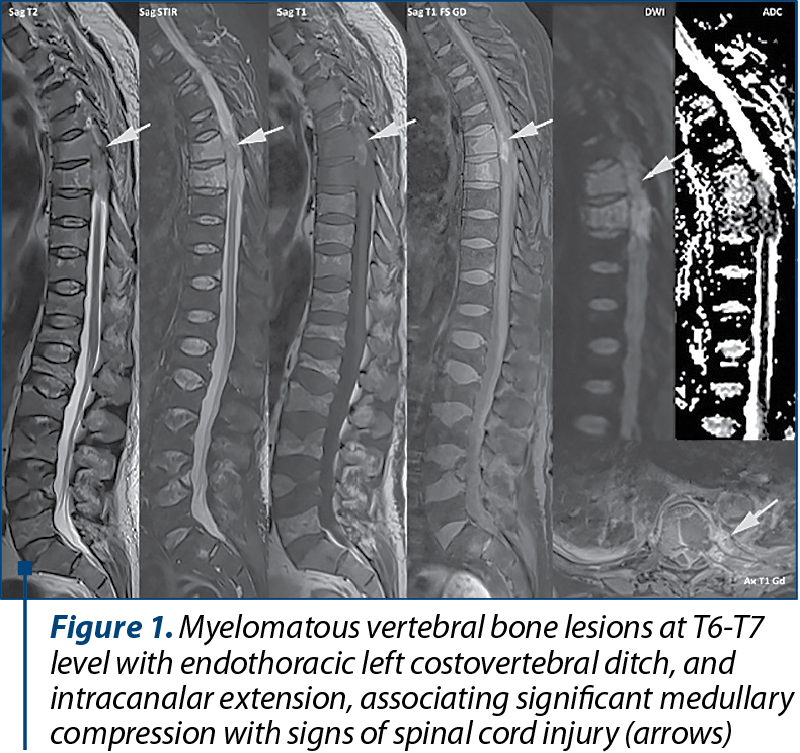
Case 1. A 66-year-old man diagnosed with MM stage IIIB presented in the department of hematology of our clinic accusing back pain with irradiation at the costal grille, and marked functional impotence for which it was performed in emergency an MRI exam that highlighted myelomatous vertebral bone lesions in the toraco-lumbar spine. The bone lesions appear in high signal intensity on T2 and STIR wi, low signal intensity on T1 wi, with paramagnetic contrast enhancement and water restriction on the DWI. It is noticeable that the lesion from T6-T7 level has an endothoracic paravertebral and intracanalar extension, associating significant medullary compression with MR signs of spinal cord injury (Figure 1).
Case 2. A 70-year-old patient, diagnosed with MM in stage IIIB, is hospitalized by emergency for back pain and newly installed paraparesis, for which in the first phase a CT scan is performed. The CT exam highlights a tumor with irregular contour located into the left thoracic posterior wall between the V-VIII posterior costal arches, with the interest of ipsilateral paravertebral muscles and endothoracic prolapse. Then, an MRI evaluation is performed, confirming the presence of the posterior left thoracic parietal tumor mass, which appears in high signal intensity on T2 and STIR images, respectively low signal intensity on T1 wi. The lesion presents endothoracic extension and affects the spinal canal, causing medullary compression with secondary medullary suffering in the T5-T7 segment (Figure 2).

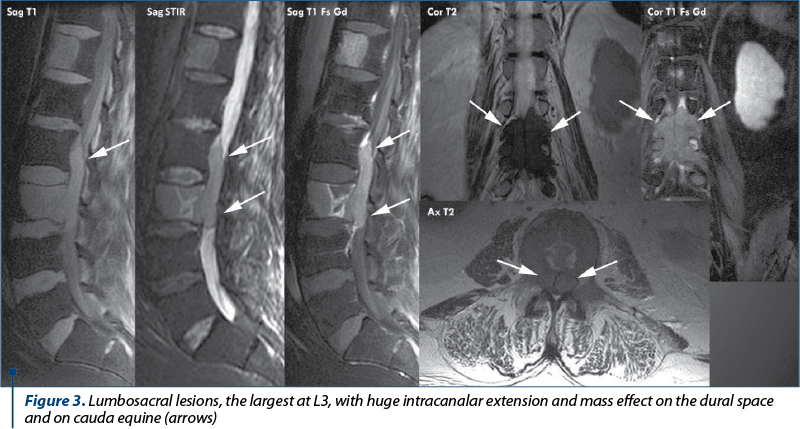
Case 3. A lumbar spine MRI exam was performed in a patient diagnosed with MM stage IIIA for back pain and fatigue that revealed multiple tumoral thoracic and lumbosacral vertebral lesions, the largest at L3 with intracanalar extension and mass effect on the dural space and on cauda equina spinal nerves (Figure 3).
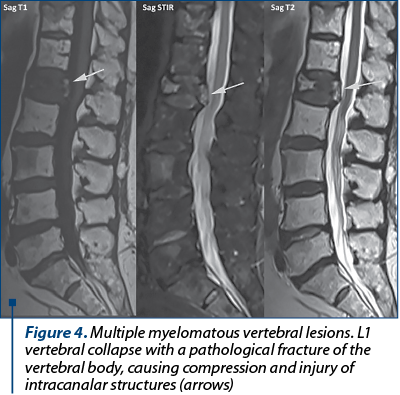
Case 4. A 77-year-old patient known with MM was hospitalized for severe lumbar pain, persistent paresthesia in the lower limbs, walking disorders, and left paraparesis. MRI evaluation was performed and revealed L1 vertebral collapse with a medio-corporeal fracture, causing compression of the intracanalar structures (Figure 4).
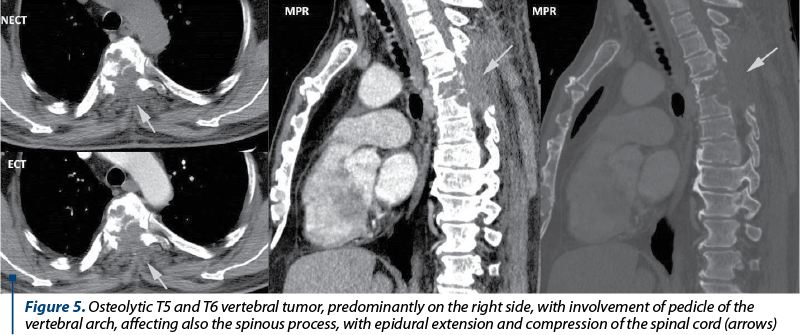
Case 5. A patient diagnosed with MM came into the hematology emergency room for paraparesis. The unenhanced and enhanced CT exam performed in emergency, followed by multiplanar reconstructions highlighted an osteolytic vertebral tumor centered at the T5 and T6 vertebral bodies, predominantly on the right side, with pedicle damage, and with the involvement of spinous process, epidural extension and compression of the spinal cord (Figure 5).
Discussion
MM is a hematological multicentric disorder(1,2). It comprises 1% of malignant tumors and 10-15% of hematopoietic neoplasms. The spine is one of the most commonly involved sites and pathological fractures of the spinal column are the most common spinal involvement of MM. In extensive spinal involvement of MM, tumors can generate SCC, which is reported to develop in 11-24% of patients(2). SCC is a severe complication of vertebral body myeloma lesion and should be diagnosed and treated urgently(2). Usually, this complication is associated with far advanced malignancy and with a poor prognosis(2).
Nonenhanced CT with bone reconstruction algorithm is extremely helpful in defining both lytic and blastic lesions and in visualizing the presence of cortical destruction(9). CT exam can also depict significant soft tissue abnormalities (e.g., disk herniation, ligamentous degenerative hypertrophy, epidural lesions or collections)(8). The most important limitation of this technique remains the inability to provide accurate information on spinal cord lesions and ligamentous injury(9).
Multiple myeloma represents one of the most common causes of SCC from osseous spine tumors. Usually, these myeloma lesions show a low T1 signal, a high T2 signal and contrast enhancement in the affected bone and in the epidural mass(9,11).
The imaging report of the CT or MRI examination should contain the following information: the topography of lesions; number of lesions; the semiological features of the lesions; the loco-regional extension of the mass; the complications of lesions (if they associate medullary or radicular compression, fractures), others incidental findings.
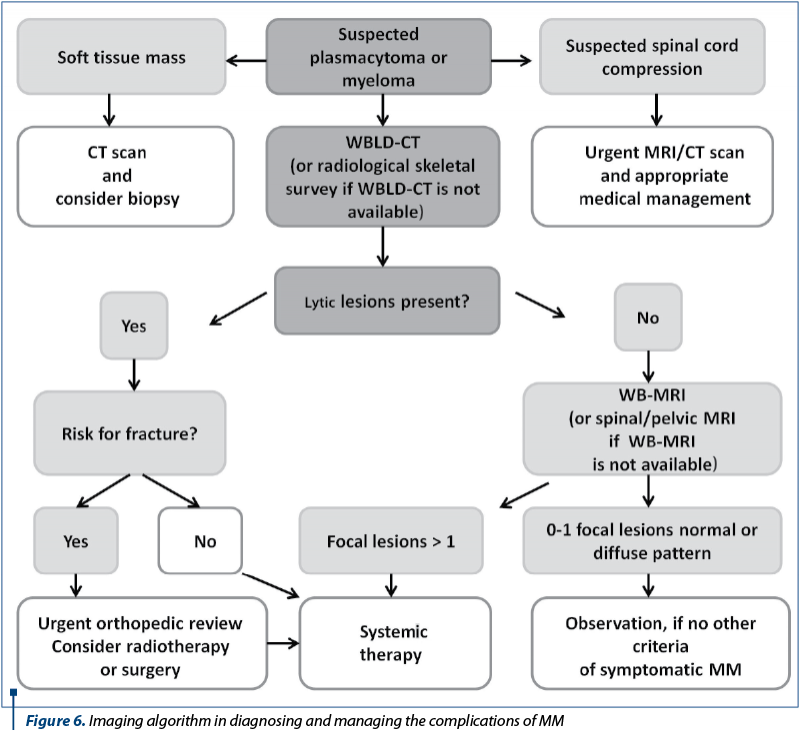
The European guidelines for MM recommend in cases which associate medullary compression syndrome (MCS) to perform immediately an MRI or CT evaluation in order to establish the correct diagnosis and the best therapy – Figure 6(10).
A multidisciplinary approach is essential for the diagnosis and treatment of vertebral lesions in MM, and the collaboration between experts (hematologists, neurologists, radiologists, orthopedists, radiotherapists) is compulsory for an optimal management of these patients.
Conclusions
CT examination is sensitive in the detection of osteolytic lesions that may be associated with expansive masses, diffuse osteopenia, and fractures on the pathological bone. MRI is the best diagnosis modality for detecting spinal cord compression, epidural masses, and marrow involvement of MM.
Nowadays, the gold standard in imaging for suspected SCC is the MRI evaluation, while the CT scan can be used in cases of MRI contraindications and in patients with an altered clinical condition, due to its accessibility and the rapid acquisition.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Sen E, Yavas G. The Management of Spinal Cord Compression in Multiple Myeloma. Ann Hematol Oncol. 2016; Vol 3 (5). ISSN : 2375-7965,
- www.austinpublishinggroup.com
- Kee-Yong H, et al. Multiple Myeloma and Epidural Spinal Cord Compression: Case Presentation and a Spine Surgeon’s Perspective. Journal Korean Neurosurgical Society. 2013; 54(2): 151–154.
- Chantry A, et al. Guidelines for the use of imaging in the management of patients with myeloma. British Journal of Haematology. 2017; 178, 380–393.
- Chrzan R, Jurczyszyn A, Urbanik A, et al. Whole-Body Low-Dose Computed Tomography (WBLDCT) in Assessment of Patients with Multiple Myeloma – Pilot Study and Standard Imaging Protocol Suggestion. Polish Journal of Radiology. 2017; 82: 356-363.
- Myeloma in adults: diagnosis and management. NICE Guideline. 2015.
- Derlin T, et al. Imaging of multiple myeloma: Current concepts. World Journal of Orthopedics. 2014 Jul; 5(3): 272–282.
- Erly WK, et al. The Utility of In-Phase/Opposed-Phase Imaging in Differentiating Malignancy from Acute Benign Compression Fractures of the Spine. AJNR. 2006; 27:1183–88.
- Healy CF, et al. Multiple Myeloma: A Review of Imaging Features and Radiological Techniques. Bone Marrow Research. 2011; vol. 2011:583439.
- Distefano D, et al. Imaging of spinal cord compression. Imaging Med. 2014; Vol. 6 (1).
- Terpos E, et al. European Myeloma Network Guidelines for the Management of Multiple Myeloma-related Complications. Haematologica. 2015; 100(10): 1254–1266.
- Alnuaimi OSA, et al. Current and particular CT and MRI aspects of multiple myeloma. ECR. 2014; C-1257, doi:10.1594/ecr2014/C-1257.

Abstracts for National Conference of Medical Oncology – 19th edition
...
Obezitatea şi cancerul de sân
Iuliana Pantelimon, Tiberiu Tebeică
Această lucrare reprezintă o analiză a principalelor studii din literatura de specialitate privind mecanismele moleculare majore în ceea ce priveşte evoluţia neoplasmului mamar la pacienţii obezi. Astfel, mecanismele moleculare fundamentale descrise în literatura respectivă sunt descrise astfel: principalel...
Importanţa cunoştinţelor şi a comportamentului pacienţilor după diagnosticarea cancerului de sân
Alina Oana Rusu-Moldovan, Maria Iuliana Gruia, Dan Mihu
Cancerul mamar este neoplazia cu frecvenţa cea mai mare la sexul feminin, reprezentând aproximativ 26% din toate cancerele diagnosticate anual, fiind a doua cauză de deces după cancerul pulmonar...
Extramedullary hematopoiesis (review): typical thoracic imaging findings
Ioana G. Lupescu, Cristina A. Nicolae, Andreea Scheau, Mihnea Băilă, Sandra Moangă, Mugur C. Grasu
Scopul acestui articol este de a prezenta şi ilustra aspectele radioimagistice tipice înâlnite în hematopoieza extramedulară cu afectare toracică, aspecte care permit excluderea altor neoplasme sau ma...
Nontraumatic splenic emergencies in onco-hematological pathology: what is important to know in CT evaluation?
Ioana G. Lupescu, Cristian Anghel, Dumitru Radu-Lucian , Cristina Dumitrescu, Dijmărescu Adrian , Mugur C. Grasu
Scopul acestui articol este de a prezenta şi ilustra aspectele computer-tomografice (CT) înâlnite în urgenţele splenice – vascular...