Importanţa evaluării computer-tomografice în detecţia interesării tumorale limfomatoase cardio-pericardice
Value of computed tomography evaluation in the detection of cardio-pericardial lymphomatous involvement
Abstract
Leukemia and malignant lymphoma are most likely to involve the cardiac chambers and pericardium, often by contiguous direct extension from a mediastinal mass. Our study’s objective is to discuss and illustrate computed tomography (CT) findings in both cardiac and pericardial involvement in patients diagnosed with a hematologic malignancy and radiologic evidence of a mediastinal mass. We reviewed our database for a period of ten years (between January 2010 and March 2020) and we selected four patients with radiologic evidence of a mediastinal mass and tumoral extension in cardio-pericardial structures, in the context of a hematologic malignancy. All our patients have been investigated by CT and were diagnosed with non-Hodgkin lymphoma. In three cases, we found intraatrial extension of the tumoral mass, in one case with both atria affected. Tumoral encasement and obstruction of the superior pulmonary veins were noted in two cases, and CT signs of superior vena cava syndrome (SVCS) were noted in two cases with direct invasion and venous compression by the tumoral mass. CT is an investigation dedicated to the evaluation of cardio-pericardial tumoral extension in cases of malignant hematological disease, allowing to detect the extent of tumoral involvement or to assess thoracic emergency conditions (SVCS cardiac tamponade, pulmonary embolism).Keywords
pericardiummediastinal massCTlymphomaRezumat
Leucemiile şi limfoamele maligne interesează frecvent structurile cardio-pericardice, cel mai adesea prin extensie directă de la o masă mediastinală aflată în contiguitate cu acestea. Obiectivul studiului nostru a fost de a discuta şi ilustra aspectele computer-tomografice (CT) ale interesărilor tumorale simultane cardiace şi pericardice la pacienţii diagnosticaţi cu boli hematologice maligne şi cu aspect radioimagistic de masă tumorală mediastinală. Am revizuit baza noastră de date pe o perioadă de 10 ani (ianuarie 2010 – martie 2020) şi am selectat patru pacienţi cu afectare simultană atât a pericardului, cât şi a structurilor cardiace, în context de boală hematologică malignă şi aspect radioimagistic de masă mediastinală. Toţi pacienţii selecţionaţi au fost investigaţi CT şi au fost diagnosticaţi cu limfom malign non-Hodgkin. În trei cazuri a fost evidenţiată extensia tumorală intraatrială, unul dintre cazuri cu interesare biatrială. Obstrucţia şi înglobarea tumorală a venelor pulmonare superioare au fost evidenţiate în două cazuri, iar semne imagistice de sindrom de venă cavă superioară (SVCS) au fost identificate CT în alte două cazuri, cu obstrucţie şi infiltrare tumorală venoasă. Examinarea CT reprezintă o investigaţie dedicată evaluării extensiei tumorale cardio-pericardice în cazurile de boală hematologică malignă, identificând atât gradul extensiei tumorale, cât şi urgenţele medicale la nivel toracic (SVCS, tamponadă cardiacă, embolie pulmonară).Cuvinte Cheie
pericardmasă mediastinalăCTlimfomIntroduction
Any metastatic malignancy may involve the pericardium, but hematologic malignancies tend to involve the pericardium and cardiac structures more often than the others(1,2). Retrograde lymphatic, transvenous and contiguous direct extension, as well as hematogenous spread are the main pathways for secondary tumoral cardiac and pericardial involvement(1,3). Imaging findings in pericardial involvement typically include nodular or irregular pericardial thickening with enhancement and effusion(4), discrete pericardial nodules(2), pericardial effusion, more often hemorrhagic(5), masses arising or contiguous with the pericardium(6). The meticulous radiological investigation is therefore mandatory, an accurate and timely diagnosis having therapeutic consequences.
Materials and method
We made a retrospective study for a period of 10 years (between January 2010 and March 2020), and we selected 101 patients with a hematologic malignancy and CT evidence of a mediastinal tumoral mass, four of them with pericardial and cardiac tumoral extension. All patients underwent CT investigation. CT examinations included one non-enhanced CT phase (NECT), in order to evaluate CT attenuation values of pericardial effusions and calcifications, respectively tumoral mass necrosis, fat, hemorrhage or calcifications, and two contrast-enhanced CT (CECT) in arterial and venous phase, in order to evaluate the tumoral mass, vascular and cardiac structures, and other associated anomalies. Before the CT exam, the allergic history and the serum creatinine level had been checked. The injection ratio was minimum 3 ml/s and the iodinated product was injected in a quantity of 1-1.5 ml/kg b.w. The patients were investigated on 16 or 64 multidetector (MD) CT scanners. The physical parameters used for CT consists in axial thickness slices of 5 mm with 1.25 or 1.5 mm reconstruction interval. CT acquisition was initiated at 25 seconds for the arterial phase and at 80-100 seconds for the venous phase. Different planes reconstructions (coronal, sagittal, oblique views) have been performed in order to have an optimal visualization of the pericardium and vascular structures.
Results
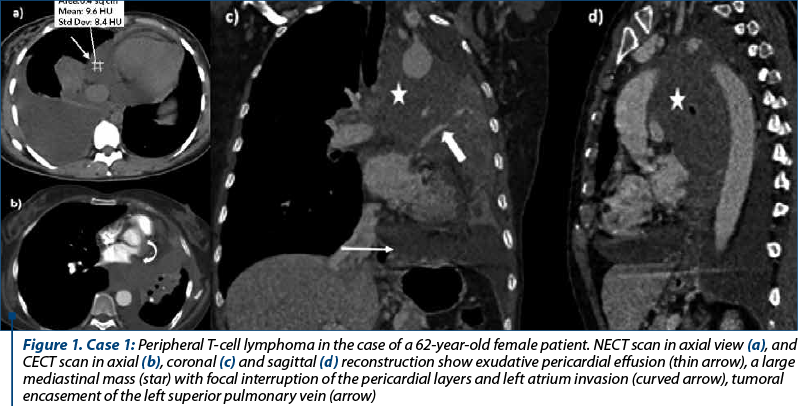
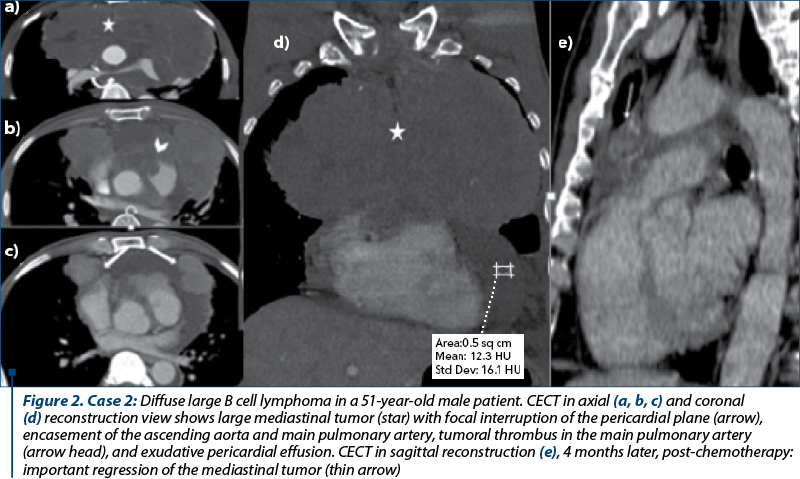
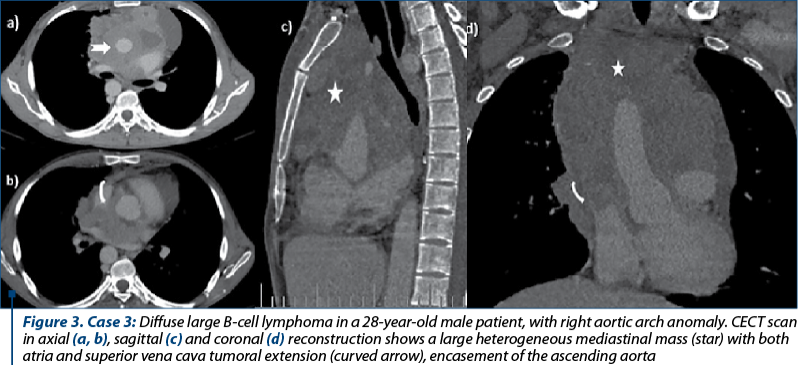
We selected four cases of patients diagnosed with malignant non-Hodgkin lymphoma, with radiological evidence of mediastinal tumors and cardio-pericardial tumoral invasion, three males and one female, with ages between 28 and 62 years old. All patients were investigated with MDCT, computed tomography investigation being able to define the correct extent of the cardio-pericardial tumoral involvement and the vascular permeability. The mediastinal tumors were located in one case in the middle and posterior (Case 1, Figure 1), respectively in the middle and anterior compartment in the second case (Case 2, Figure 2), and in all mediastinal compartments in the other two patients (Case 3, Figure 3). In all cases, CT examination showed bulky, infiltrative mass, with a median axial diameter of 11 cm, one of them with large axis of almost 21 cm, all tumoral masses contiguous with the pericardium. Tumoral invasion of the superior pulmonary veins was identified in two cases. Medium-large pericardial effusion was noted in two cases with mean attenuation values of 10 UH, with slight enhancement of the pericardial layers, but no clinical signs of cardiac tamponade present. Tumoral encasement of the ascending aorta and main pulmonary artery was identified in two cases, in one case with pulmonary artery thrombosis association. Tumoral obstruction of the superior vena cava was present in two cases, in one case with complete obliteration, azygos vein dilatation and collateral vessels in the anterior chest wall.
Discussion
Secondary cardiac and pericardial involvement by lymphoma is more common than primary cardiac lymphoma, at the autopsy being described in almost 18% of patients with non-Hodgkin lymphoma(7). Retrograde lymphatic, transvenous and contiguous direct extension, as well as hematogenous spread are the main pathways for secondary tumoral cardiac and pericardial involvement(1,3). CT imaging findings in primary cardiac lymphoma are resembling secondary involvement, typically seen as a bulky cardio-pericardial infiltrative tumoral mass(8). In our cases, we noted voluminous heterogenous mediastinal mass contiguous with the pericardial layers, with tumoral infiltration of the atrial cavities in three cases (Case 1 and Case 3) and of the pulmonary veins in two cases (Case 1). Intrapericardial tumoral nodular extension of the mediastinal mass was noted in one case (Case 2). Nodular or diffuse pericardial thickening and contiguous tumoral mass with the pericardial structure are considered important CT imaging signs of tumoral pericardial involvement(9). Also, tumoral obliteration of the superior pulmonary veins represents a reliable sign of intrapericardial tumoral extension(1), presented in two cases (Case 1). CT imaging findings of enlarged mediastinal lymphadenopathies, pericardial nodularity and haematic pericardial effusion are important predictors of malignant pericarditis(10). We found two cases with medium-large pericardial effusion, with mean attenuation value of 10 UH (Case 1 and Case 2). Although in literature the right atrium was mainly involved by lymphomatous tumors(8), in our patients we found left atrium involvement in three cases (Case 1 and Case 3). Thickening or nodularity of cardio-pericardial structures and intracardiac masses can mimic metastatic cardiac disease(1), but the identification of a tumoral encasement of the mediastinal vessels without evidence of invasion represents a sign of lymphomatous tumoral involvement(8). In our patients, ascending aorta and the main pulmonary artery tumoral encasement were identified in two cases (Case 2 and Case 3).
Conclusions
CT represents a reliable imaging technique to define the cardio-pericardial tumoral extension of an intrathoracic hematological mass and to assess vascular involvement or thoracic emergency conditions (SVCS, cardiac tamponade or pulmonary embolism).
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Chiles C, et al. Metastatic involvement of the heart and pericardium: CT and MR Imaging. Radiographics. 2001; 21:439-449.
-
Peebles CR, et al. Pericardial disease – anatomy and function. The British Journal of Radiology. 2011; 84, S324-S337.
-
Bussani R, et al. Cardiac Metastases. J Clin Pathol. 2007 Jan; 60(1): 27-34.
-
Czum JM. Evaluation of the Pericardium with CT and MRI. ISRN Cardiol. 2014; 174098.
-
Sun JS, et al. CT findings in patients with pericardial effusion: differentiation of malignant and benign disease. Am J Roentgenol. 2010; 194:W489-W494.
-
Restrepo CS, et al. Imaging findings in cardiac tamponade with emphasis on CT. Radiographics. 2007; 27:1595-1610.
-
O’Mahony D, et al. Cardiac involvement with lymphoma: a review of the literature. Clin Lymphoma Myeloma. 2008 Aug; 8(4):249-252.
-
Bligh MP, et al. Spectrum of CT findings in thoracic extranodal non-Hodgkin lymphoma. Radiographics. 2017; 37:439-461.
-
Ünal E, et al. The imaging appearances of various pericardial disease. Insights into Imaging. 2019; 10:42.
-
Pawlak CA, et al. Diagnosis of malignant pericarditis: a single centre experience. Kardiol Pol. 2012; 70(11):1147-53.
-
Jeudi J, et al. Cardiac lymphoma: radiologic-pathologic correlation. Radiographics. 2012; 32:1369-1380.

Predispoziţia la transformare din sindrom mielodisplazic în leucemie acută – prezentare de caz
Iuliana-Maria Nicorescu, Minodora Onisâi, Mihaela Găman, Iuliana Iordan, Lidia Felicia Mihai, Andreea Crăciunescu, Mihai Ciochinaru, Ana Maria Vlădăreanu
Sindroamele mielodisplazice (SMD) sunt un grup de boli clonale ale celulei stem hematopoietice, caracterizate de mielodisplazie şi...
Etiopatogenia şi manifestările clinice ale limfoamelor asociate infecţiei cu HIV
Andreea-Daniela Gheorghe, Andra-Iulia Suceveanu, Adrian-Paul Suceveanu, Laura Mazilu
Infecţia cu virusul imunodeficienţei umane (HIV) este asociată cu dereglări ale imunităţii celulare, care predispun la apariţia neoplaziilor, inclusiv a limfoamelor. Speranţa de viaţă a persoanelor diagnosticate cu HI...
Managementul tratamentului şi urmărirea pacienţilor cu melanom malign în perioada pandemiei de COVID-19
Daniela Zob, Cornelia Niţipir, Laura Mazilu, Gabriela Niculai, Alina Moldovan, Lidia Kajanto, Andra-Iulia Suceveanu, Radu Florin, Silviu VOINEA, Viorel Savin, Amalia Constantinescu, Alexandru Grigorescu, Raluca Ioana Mihăilă, Dana Lucia Stănculeanu
Melanomul este o problemă de sănătate publică, prin incidenţa sa în creştere şi prin vârsta mică la diagnostic. Există trei sub...
Aspecte imagistice în sindroamele compresive pericardice – tamponada cardiacă în patologia oncologică
Anca Flintoacă-Filip, Elena Apostol, Simina Apostol, Ioana G. Lupescu
Tamponada cardiacă reprezintă alterarea statusului hemodinamic, produsă prin compresia cardiacă determinată de o varietate de factori şi afecţiuni, inclusiv pericardita tumorală şi compresia tumora...
Aspecte imagistice în fracturile vertebrale tumorale versus osteoporotice
Alexandra Vlăduțu, Anca Filip-Flintoacă, Ioana G. Lupescu
Tasările vertebrale osteoporotice după o traumă minoră la pacienții vârstnici pot fi greu de diferențiat de fracturile tumorale vertebrale....