Liver epithelioid hemangioendothelioma: are there CT and MRI specific criteria?
Hemangioendoteliomul epitelioid hepatic: există criterii CT şi IRM specifice?
Abstract
Hepatic epithelioid hemangioendothelioma (HEH) is a rare vascular tumor of endothelial origin which may present as a solitary nodule or, more frequently, as multifocal nodules that tend to coalesce into a diffuse lesion. CT and MR imaging are important to make a complete liver HEH involvement and to assess the presence of extrahepatic disease. The pathological exam remains the gold standard to confirm the diagnosis of HEH. In this case presentation, we discuss and illustrate the CT and MRI findings of HEH.Keywords
epithelioid hemangioendotheliomaCT and MRI criteriaRezumat
Hemangioendoteliomul epitelioid hepatic (HEH) este o tumoră vasculară rară cu origine endotelială, care se poate prezenta sub forma unui nodul solitar sau, mai frecvent, sub formă de noduli multipli care tind să se unească într-o leziune difuză. Imagistica prin CT şi rezonanţă magnetică (IRM) este importantă pentru a realiza o evaluare completă a ficatului în HEH şi pentru a evalua prezenţa bolii extrahepatice. Examenul morfopatologic rămâne standardul de aur pentru a confirma diagnosticul de HEH. În această prezentare de caz, vom discuta şi ilustra aspectele CT şi IRM întâlnite în HEH.Cuvinte Cheie
hemangioendoteliom epiteliodcriterii imagistice CT şi IRMIntroduction
Hepatic epithelioid hemangioendothelioma (HEH) is a vascular tumor of endothelial origin with low to intermediate grade malignancy. HEH may present as a solitary nodule or, more frequently, as multifocal nodules which tend to coalesce into diffuse lesions in the late stages of the disease. Nodules and diffuse liver mass may coexist. CT and MR imaging are important to make a complete liver evaluation of HEH involvement and to highlight the presence of extrahepatic disease. The pathological exam remains the gold standard to confirm the diagnostic of HEH.
Case presentation
The patient D.M., female, 63 years old, with anorexia and diffuse abdominal pain, was referred by the gastroenterologist for an abdominal ultrasound (US). The laboratory tests were without particularities. Because the US images reveled inhomogeneous hepatomegaly with steatosis areas, an MRI evaluation was performed. The patient was explored in the supine position with a surface phased-array coil. For the complete evaluation of liver lesions, breath-hold coronal T2-weighted short TE sequences were initially performed, followed by transverse T1-weighted dual-echo in-phase and out-phase sequences. Three-dimensional (3D) fat-saturated (FS) T1-weighted dynamic contrast-enhanced sequences were performed during suspended respiration (gadoxetic acid; 0.1 mmol/kg) injected intravenously at a rate of 1 ml/s. Dynamic contrast-enhanced MRI was performed in the transverse plane followed by the hepatic late arterial phase (after 35 s), portal venous (after 70 s) and delay phases (180 s). After dynamic contrast-enhanced 3D T1 FS weighted imaging, transverse respiratory-triggered diffusion-weighted (DWI) single-shot echo-planar imaging sequence was performed by using two b-values of 0 and 800 s/mm2, followed by T2 FS fast spin echo sequence. The hepatobiliary phase was performed 20 minutes after contrast material i.v. injection.
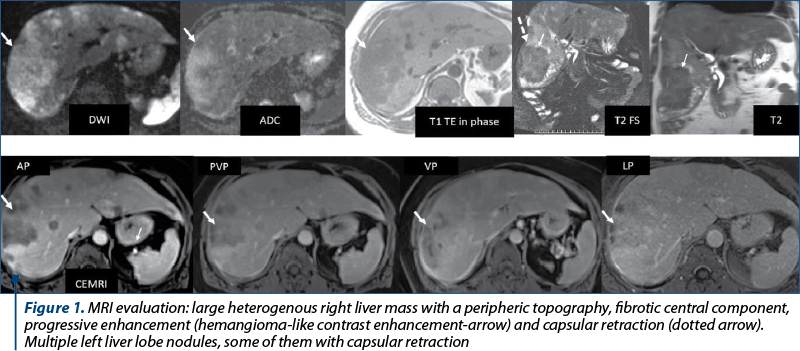
The MRI exam revealed tumoral left liver nodules and a large tumoral mass located at the periphery of the right liver lobe with extension to capsule, the presence of capsular retraction and a “target” sign appearance (Figure 1).
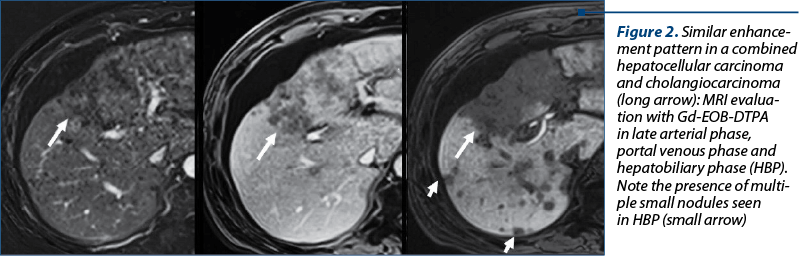
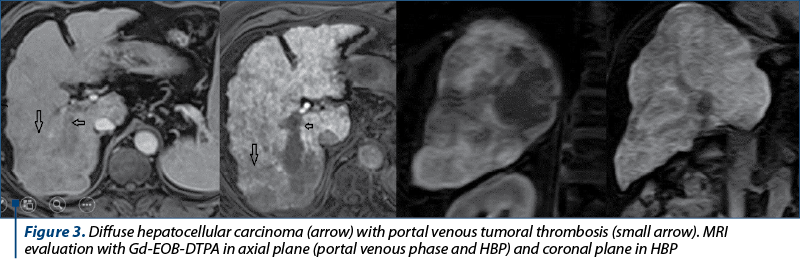
Into the list of possible diagnostics, there enter epithelioid hemangioendothelioma, angiosarcoma, intrahepatic cholangiocarcinoma, combined form of hepatocellular carcinoma and cholangiocarcinoma (Figure 2), diffuse hepatocellular carcinoma (Figure 3), treated liver malignancy, and confluent fibrosis. In order to have the final pathological diagnostic, a biopsy under CT was performed.
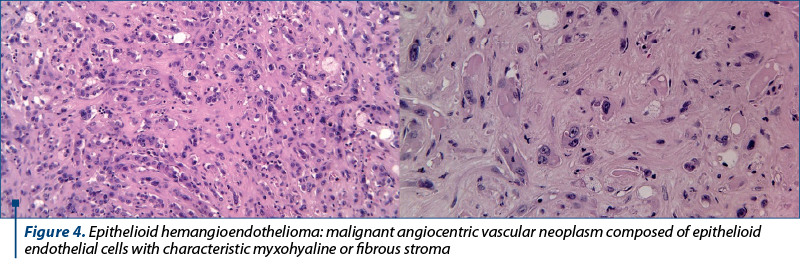
The histopathological exam (Figure 4) highlighted the pattern of epithelioid hemangioendothelioma based on malignant angiocentric vascular neoplasm composed of epithelioid endothelial cells with characteristic myxohyaline or fibrous stroma most commonly with WWTR1-CAMTA1 or YAP1-TFE3 fusion (courtesy to Dr. Mihaela Mihai).
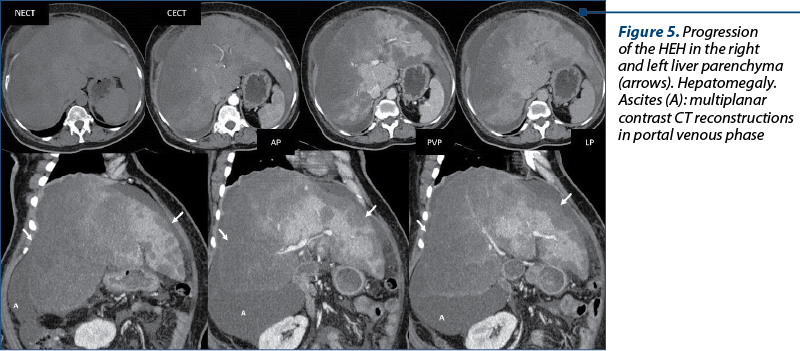
The multidisciplinary team decided, in this case, to performed an orthotopic liver transplant (OLT), but before the liver transplant, a CT was done. Non-contrast and three-phase dynamic contrast-enhancement CT scan were performed. The delay between the first MR evaluation and the CT exam was four months. The conclusion of the CT evaluation was in favor of HEH progression, with hepatomegaly and ascites (Figure 5).
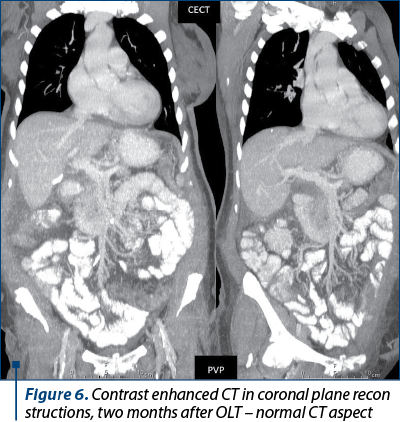
After the OLT, the clinical evolution was good, such as the imaging monitoring with normal ultrasound (US) and CT findings (Figure 6).
Discussion
Epithelioid hemangioendothelioma is a locally aggressive vascular neoplasm originating from vascular endothelial or pre-endothelial cells. It can arise anywhere in the body and can metastasize to the viscera, bones and soft tissue. The most common sites of involvement are the liver, bone and lung(1,2).
The clinical presentation of EHE is nonspecific and usually consists of signs and symptoms related to the involvement of local organs by the primary tumor or metastases. Approximately 28% of the patients with EHE have no symptoms, and their tumor is discovered incidentally(2).
HEH appears to have a clinical course between benign hemangioma and angiosarcoma. The World Health Organization classifies HEH as a malignant tumor(10). In the majority of patients, both lobes of the liver are involved, and lung, peritoneum, lymph nodes and bone are the most common sites of simultaneous extrahepatic involvement(1,3). HEH predominantly occurs in adult females. The etiology of HEH remains unknown; however, it may be associated with oral contraceptive use, exposure to polyethylene, trauma or viral hepatitis(3).
The imaging findings of hepatic HEH vary according to the stage of the disease, and two patterns have been reported: a nodular pattern, which is seen in the early stage of the disease, and a diffuse pattern, which is typically seen in advanced stages, appearing as confluent coalescent masses that can be associated with hepatic vascular invasion. Commonly, liver nodules are multifocal, distributed in the periphery of the liver, and may be accompanied by capsular retraction(4-7).
Imaging plays a major role in determining the sites of involvement, which has an important prognostic significance and it also can help guide US or CT biopsy and to monitor the response to treatment. On unenhanced CT, lesions are iso- or hypo-attenuated to the liver parenchyma. Small foci of calcification may be present. The enhancement characteristics show in general peripheral enhancement in the arterial phase in association with stronger enhancement in portal and late phase manifesting as a target sign(1,6-9).
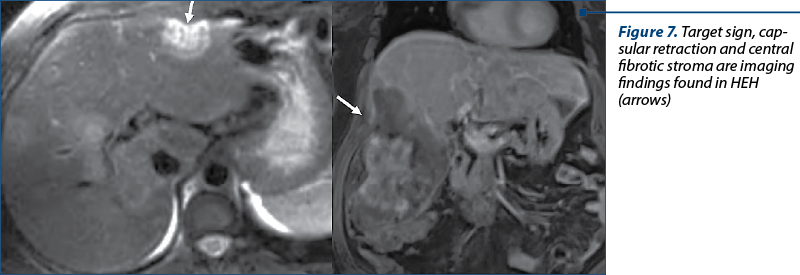
On MRI, most HEH lesions are T1 hypointense and heterogeneously T2 hyperintense relative to uninvolved liver parenchyma. Some lesions may have a concentric zonal or targetoid appearance (black or white) on T2 and contrast-enhanced T1-weighted images. Black target-like sign corresponds to a central T2 hypointensity and a reduced enhancement after contrast injection due to areas of avascular stroma, hemorrhage, necrosis and calcification; peripheral hyperintensity and increased enhancement correspond to edematous connective tissue and viable tumor(9-11). The periphery of the tumor shows markedly hyperintensity on DWI, representing hypercellular tumor, whereas central regions show hypointensity on high-b value images as a result of relatively hypocellular, myxoid and fibrous stroma(11). Liver capsular retraction may be present in most patients with HEH (Figure 7).
More seldom, nodular enhancement along the central vessels (“lollipop” sign) can be found in HEH.
The natural prognosis of HEH depends on the primary site of involvement, the grade of the tumor, the presence of invasion of critical structures, and the presence of metastases(1-11).
Liver transplant (LT) can be curative for patients with HEH in which complete surgical resection is not possible. Limited extrahepatic extension is not a contraindication for LT(12). Recurrent HEH is seen in approximately 25% of patients after liver transplant(12).
Conclusions
The imaging findings of HEH vary in correlation to the stage of the disease. Lesions are commonly multifocal, distributed into the periphery of the hepatic parenchyma, with a target sign pattern, and may be accompanied by capsular retraction. Because also other types of primary and metastatic liver tumors can have theses aspects, intratumoral biopsy with pathological exam offers the final positive diagnostic.
Conflict of interest: none declared.
Financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Jang JK, Thomas R, Braschi-Amirfarzan M, Jagannathan JP. A Review of the Spectrum of Imaging Manifestations of Epithelioid Hemangioendothelioma. AJR Am J Roentgenol. 2020;215(5):1290-1298.
-
Lau K, Massad M, Pollak C, et al. Clinical patterns and outcome in epithelioid hemangioendothelioma with or without pulmonary involvement: insights from an internet registry in the study of a rare cancer. Chest. 2011;140(5):1312-1318.
-
Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: A clinicopathologic study of 137 cases. Cancer. 1999;85(3):562-582.
-
Furui S, Itai Y, Ohtomo K, et al. Hepatic epithelioid hemangioendothelioma: report of five cases. Radiology. 1989;171(1):63–68
-
Gan LU, Chang R, Jin H, Yang LI. Typical CT and MRI signs of hepatic epithelioid hemangioendothelioma. Oncol Lett. 2016;11(3):1699-1706.
-
Chen Y, Yu RS, Qiu LL, Jiang DY, Tan YB, Fu YB. Contrast-enhanced multiple-phase imaging features in hepatic epithelioid hemangioendothelioma. World J Gastroenterol. 2011;17(30):3544-3553.
-
Van Beers B, Roche A, Mathieu D, Menu Y, Delos M, Otte JB, Lalonde L, Pringot J. Epithelioid hemangioendothelioma of the liver: MR and CT findings. J Comput Assist Tomogr. 1992;16(3):420424.
-
Kim EH, Rha SE, Lee YJ, Yoo IR, Jung ES, Byun JY. CT and MR imaging findings of hepatic epithelioid hemangioendotheliomas: Emphasis on single nodular type. Abdom Imaging. 2015;40(3):500-509.
-
Gam L, Chang R, Jib H, Yang L. Typical CT and MRI signs of hepatic epithelioid hemangioendothelioma. Oncology Letters. 2016;11(3):1699-1706.
-
Liu X, Yu H, Zhang Z, et al. MRI appearances of hepatic epithelioid hemangioendothelioma: a retrospective study of 57 patients. Insights into Imaging. 2022;13(1):65.
-
Bruegel M, Muenzel D, Waldt S, Specht K, Rummeny EJ. Hepatic epithelioid hemangioendothelioma: Findings at CT and MRI including preliminary observations at diffusion-weighted echoplanar imaging. Abdom Imaging. 2011;36(4):415-424.
-
Remiszewski P, Szczerba E, Kalinowski P, Gierej B, Dudek K, Grodzicki M, Kotulski M, Paluszkiewicz R, Patkowski W, Zieniewicz K, Krawczyk M. Epithelioid hemangioendothelioma of the liver as a rare indication for liver transplantation. World J Gastroenterol. 2014;20(32):11333-11339.

Acute myeloid leukemia cells in microscopic images
Stejara Nicoleta Mihai, Cristina Enache, Cristina Mambet, Ana Maria Vlădăreanu
Representative images of microscopic examination of May-Grünwald-Giemsa-stained bone marrow aspirate smears from patients with acute myeloid leukemia at diagnosis...
New changes in the classification of acute myeloid leukemia proposed by WHO 2022
Silvia Badea, Emilia Severin, Diana Cîşleanu, Cristina Mambet, Claudiu Dragoş Popescu, Ana Maria Vlădăreanu
Noua revizuire a clasificării OMS (Organizaţia Mondială a Sănătăţii) din 2022 a leucemiilor acute mieloide (LAM) are ca scop evidenţierea noilor date obţinute în ultimii ani cu privire la patogeneza b...
Some important trials regarding the digestive cancers presented at ASCO and ESMO congresses with impact in current medical practice
Alexandru C. Grigorescu
Acest scurt review se referă la principalele studii prezentate la congresele ASCO şi ESMO din 2023, având ca subiect cancerele digestive. Din analiza acestor studii rezultă că chimioterapia, în specia...
Aspecte imagistice în fracturile vertebrale tumorale versus osteoporotice
Alexandra Vlăduțu, Anca Filip-Flintoacă, Ioana G. Lupescu
Tasările vertebrale osteoporotice după o traumă minoră la pacienții vârstnici pot fi greu de diferențiat de fracturile tumorale vertebrale....
Importanţa rezultatului computer-tomografic structurat pentru diagnosticul şi managementul adenocarcinomului ductal pancreatic
Ioana G. Lupescu, Alexandru-Ştefan Băicoianu-Niţescu, Robert Enache
Adenocarcinomul ductal pancreatic este un neoplasm extrem de agresiv....