Tumorile neuroendocrine - diagnostic şi strategii terapeutice
Ioana Luca
24 Octombrie 2015NETs are rare diseases.
There is a lack of robust source data on epidemiology
Nothing exists to describe the overall European situation:
-
Only individual country data exists
-
ENETS in process of establishing a pan-European registry.
Rare locations:
-
Liver and biliary system (0.59%)
-
Gall bladder (0.31%)
-
Meckel’s diverticulum (0.27%)
-
Oesophagus (0.2%)
Lack of awareness frequently leads to misdiagnosis or no diagnosis
-
Higher incidence in African-American than Caucasian patients
-
Potential genetic factors influencing this are currently unknown.
Rectal NETs are more common in Asian/Pacific Islander, American Indian/Alaskan Native and African American patients(4).
Race predicts outcome in patients with well-differentiated to moderately differentiated NETs (P<0.001)(4).
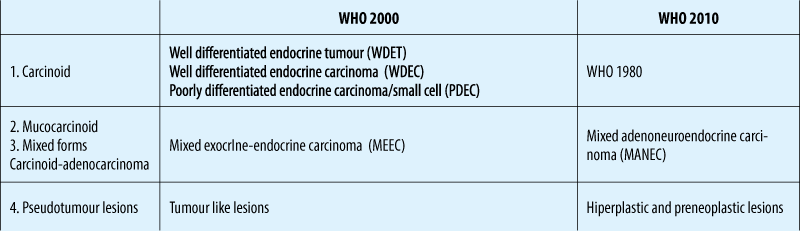
Tumor types and clasification
NENs -malignant tumours that arise from the diffuse neuroendocrine cell system.
May or may not show hypersecretion of peptides or amines causing hormonal symptoms.
Functional vs non-functional
The term NENs= the whole family of low, intermediate and high grade tumours:
-
NETs - low to intermediate grade neoplasms
-
NEC - only be used for high grade neoplasms.
Categorised according to their embryonic origin:
-
Foregut
-
Midgut
-
Hindgut.
Biologically relevant differences in tumours not distinguished:
Current practice describe GEP-NETS according to their location of primary origin:
-
e.g., pancreas, duodenum, small intestine etc.
-
e.g., gastrinoma, insulinoma, carcinoid syndrome etc.
WHO clasification
TNM staging (ENETS)
Grading (ENETS)
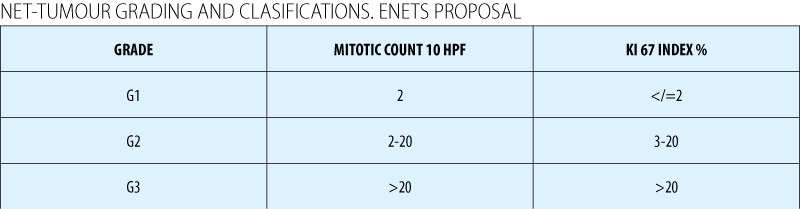
Assessment of mitotic rate: Ki67
In Europe - Ki67 is mandatory for all cases (ENETS and WHO 2010)(1)
Difficulties when:
-
There is insufficient biopsy material to differentiate between Grade 1 and 2 NETs
-
When a large amount of crush artefact present.
Cell cycle-dependent marker found in higher concentrations in dividing cells.
Immunohistochemistry methods:
-
An antibody called MIB1 can reveal Ki67, indicating the level of proliferation.
A high Ki67 index indicates a fast-growing tumour - the worse the prognosis.
Diagnosis
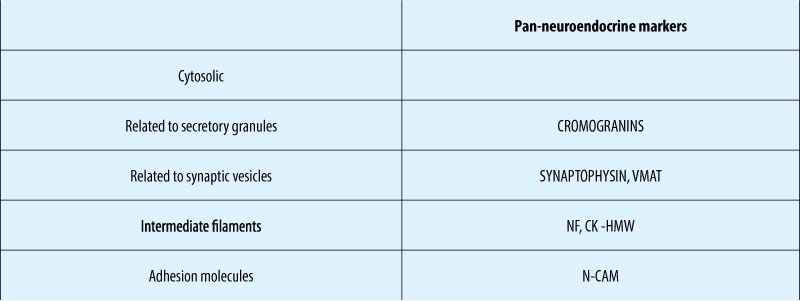
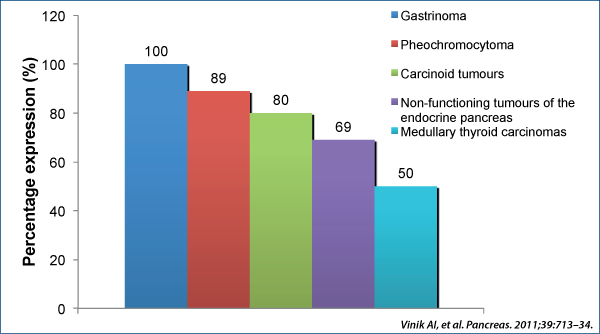
Immunohistochemical NE – markers
Non-functional pNETs
-
Can secrete pancreatic polypeptide, chromogranin A, neuron specific enolase, human chorionic gonadotrophin subunits, calcitonin, neurotensin or other peptides
-
Do not produce specific symptoms.
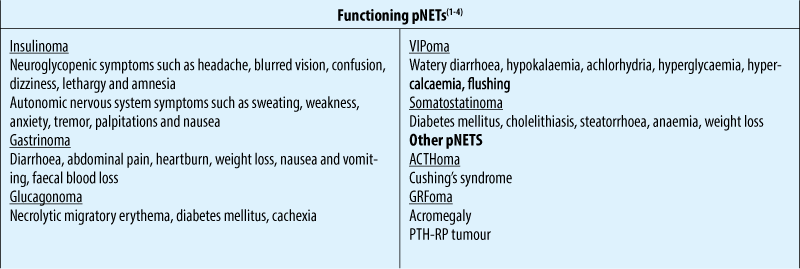
Functional pNETs
-
Are named based on the specific hormone they produce (i.e. insulin, gastrin, somatostatin, glucagon etc.)
-
Most common are insulinoma and gastrinoma (Zollinger-Ellison syndrome [ZES])
-
Other types of functional pNETs are grouped as rare functional pNETs (RFTs)
Chromogranin A (Cga)
Chromogranins A and B are protein precursors involved in the regulation of hormone secretion(1).
CgA is expressed in well-differentiated tumours(2). Can be expressed in less well-differentiated tumours that do not secrete known hormones(3).
NSE - in G3
Common conditions can increase the levels of CGA
-
Decreased renal function
-
Treatment with Proton Pump Inhibitors (PPIs)
-
Chronic gastritis
-
Essential hypertension.
Measurement of CgB as a complement to CgA has been suggested(1,2).
CgA blood levels vary according to tumour characteristics
-
Tumour mass -small tumours may be associated with normal CgA levels
-
Tumour burden
-
Progression and malignant nature of the tumour.

Many NETs of non-pancreatic origin release vasoactive peptides and amines into the systemic circulation and cause a characteristic set of symptoms called “carcinoid syndrome”(1):
-
e.g., serotonin and tachykinins.
It occurs in approximately 10% of patients with metastatic NETs(1)
Characterised in patients by:
-
Flushing (63-94%)
-
Diarrhoea (68-84%)
-
Abdominal pain (10-55%)
-
Telangiectasia (25%)
-
Bronchoconstriction (3-19%)
-
Carcinoid heart disease.
NETS FUNCTIONING pNETS - SyMpTOMS AND SYNDROMES

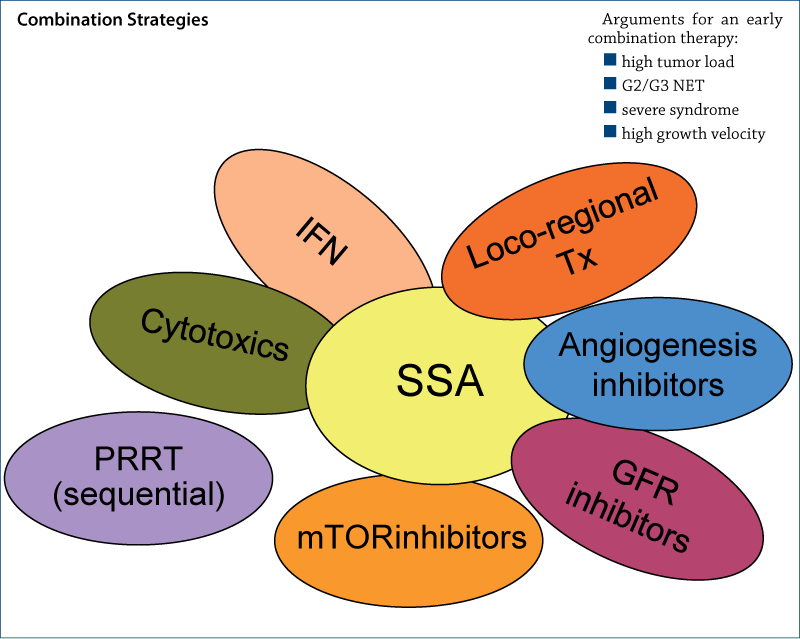
Treatment options
Management of locoregional unresectable or/and metastatic disease ases
Total tumor eradication
If total eradication not possible, then:
-
Symptomatic control
-
Prevention of complications related to the carcinoid syndrome( carcinoid heart disease, carcinoid crisis)
-
Inhibition of tumor growth/prolongation of survival.
Surgical Approaches - curative ablative
Debulking procedures
-
TACE, TAE, RFA, SIRT etc.
Medical therapy.
-
Biotherapy
·somatostatin analogues ( octreotide, lanreotide, pasireotide)
·a IFN.
-
Systemic chemotherapy
-
Molecular targeted therapies
·angiogenesis inhibitors: sunitinib, sorafenib, bevacizumab
·mTOR inhibitors: everolimus
·GF- rec inhibitors: EGF-R TKI etc.
Peptide Receptor Radionuclide Therapy (PRRT).

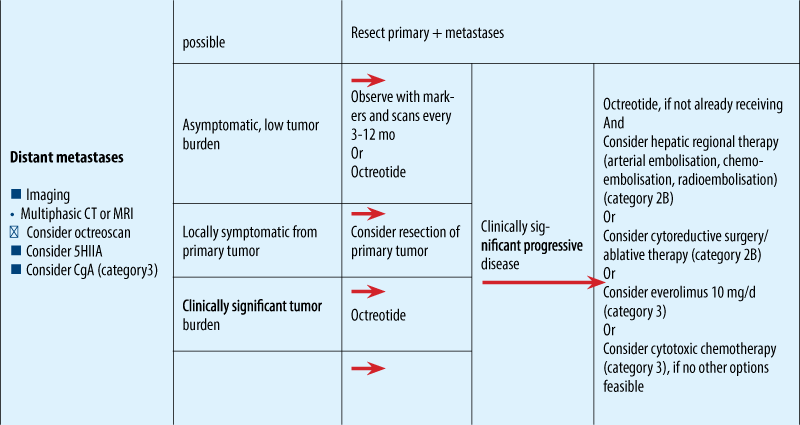
NCCN guidelines for metastatic NET
ESMO clinical guidelines

Treatment approach to liver MTS without ENETS Consensus Guidelines for LIVER MTS

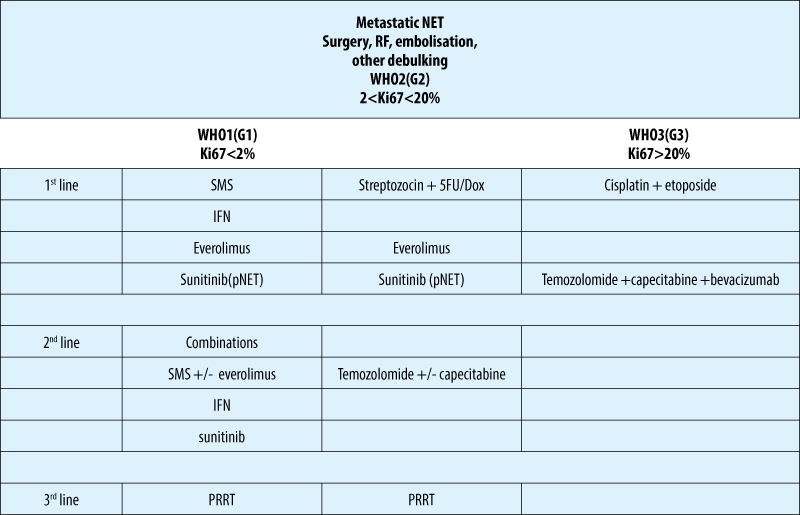
Treatment algoritm NET - based on classification
Biotherapy - somatostatin analogues
-
the use of SSA is the standard therapy in functioning NETs of any site
-
octreotide and lanreotide are considered equally effective for syndrome control (70-90% of cases)
-
a standard dose of long-acting formulations is octreotide 20-30 mg/4 weeks i.m. and lanreotide autogel 90-120mg/4 weeks s.c.
-
doses are adapted to the individual needs and depend on tumor burden
-
preventive SSA therapy prior to surgery or use of locoregional therapies ( s.c. bolus and/or i.v. 50-100 µg/h perfusion) is usually effective.
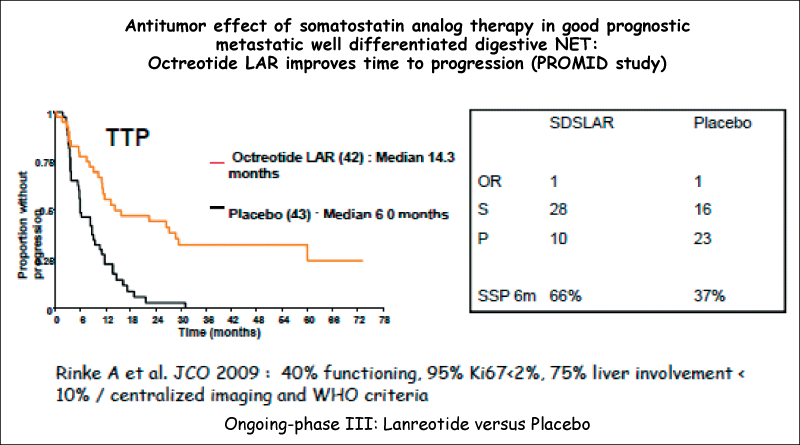
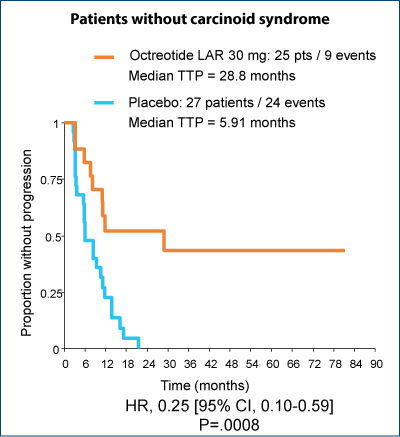
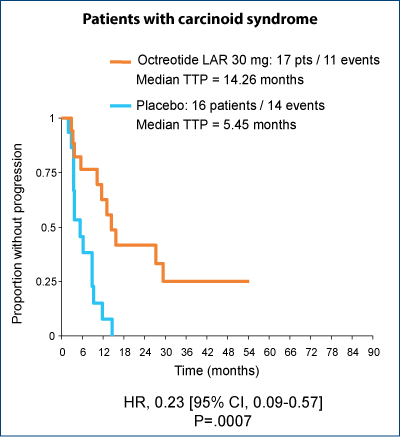
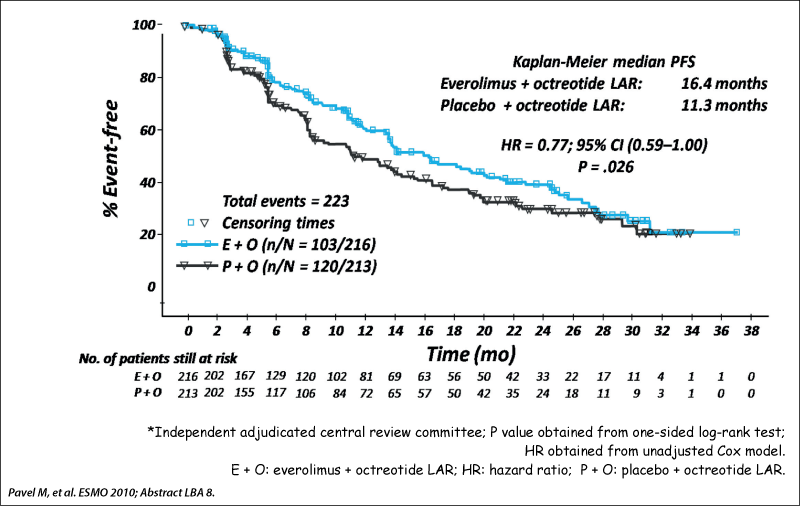
Significant improvement in TTP regardless of the presence of carcinoid syndrome
Biotherapy - IFN
-
may also be considered for symptom control, if SSA are not well tolerated
-
symptomatic remission - 30-70%
-
stabilisation/remission of tumor markers - 40%
-
tumor PR/SD - 10%
-
onset of response is more delayed than with SSA
-
recommended dose of 3-5 milion units 3 times per week
-
pegylated IFN may be considered for better tolerability ( 80-150 µg once weekly).
CHEMOTHERAPY
Few data to support the use of any existing cytotoxic chemotherapy agents.
Result are poor in patients with well-differentiated tumors, with RR of 15% in the largest published study
Option exclusively in advanced intestinal NET after failure to previous treatment lines.
Chemotherapy is the first-line therapy in NEC G3.
No clear cut-off value for Ki67 for indication of chemotherapy.
In cases of liver MTS from NEC G3, regardless of the site of the primary tumor combination chemotherapy - CISPLATIN + ETOPOSIDE is recommended early.
There is no established second line for G3 NEC
-
Temozolomide + capecitabine +/- bevacizumab;
-
CAPOX/FOLFOX/FOLFIRI.
Molecular targeted therapies
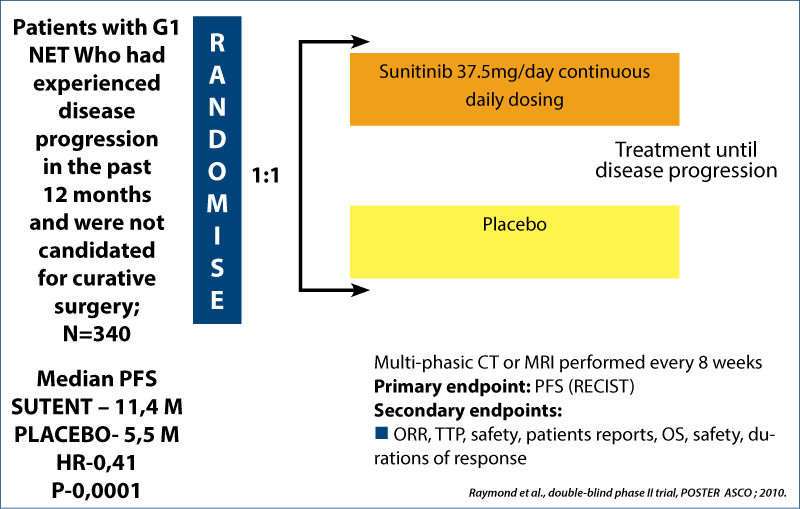
Angiogenesis inhibitors: sunitinib, sorafenib, bevacizumab.
mTOR inhibitors: everolimus.
GF–rec inhibitors: EGF-R TKI etc.
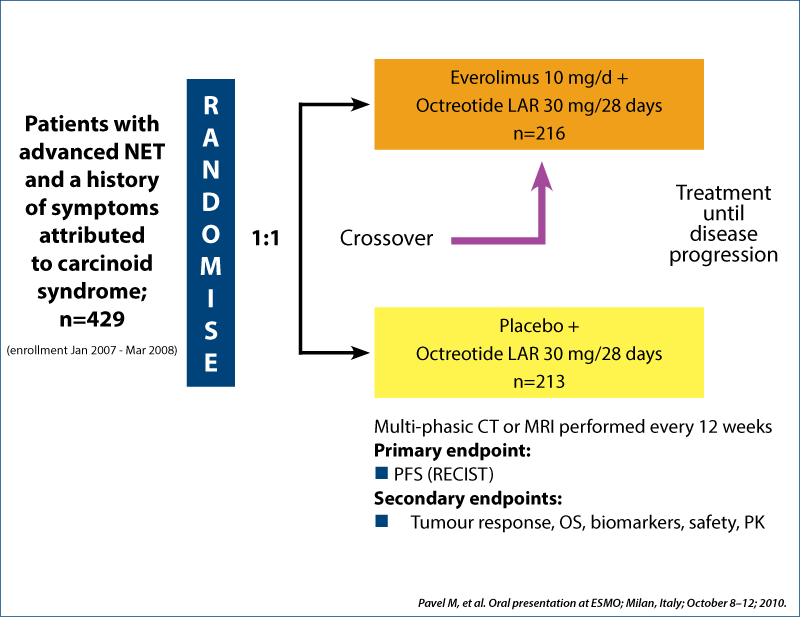
RADIANT-2 study design
Phase III double-blind placebo-controlled trial
Sunitininb in net
Phase III double-blind placebo-controlled trial
Pazonet study - pazopanib in pretreated advanced neuroendocrine tumors - a phase II, open-label trial of the Spanish task Foirce Group for NETs
Results
44 patients
Prior treatment- multitarget therapy( sunitinib)
-
mTOR inhibitors
-
both agents
Treatment- pazopanib 800 mg/zi, 28 days, +/- SSA
25 patients - was progression free at 6 m/mPFS - 9.5 months
21 patients -SD
· 73% for patients treated with multitarget inhibitor.
· 60% for patients treated with mTOR inhibitor.
· 25% -for patients treated with both agents.
Evaluated pazopanib as single agent in advanced NETs after failure of the other systemic treatments
-
Pazopanib - multitargeted for:
·Vascular endothelial growth factor receptor 1, 2, 3 VEGFR
·Platelet derived growth factor receptor alfa and beta PDGFR
· Proto-oncogene c Kit.
Primary end point - CLINICAL BENEFIT RATE (CR +PR+SD) at 6 months
-
Was evaluated translational corelation of radiology response and PFS with circulating and tissue biomarkers.
Results - biomarkers
Non-significant increase of PFS was observed in patients presenting:
lower baseline circulating tumor cell
decreased levels of soluble VEGFR 2
VEGFR 3 GENE polimorphisms.
(Potential biomarkers for selecting patients for pazopanib)
![177Lu-DOTATATE:177Lu-1,4,7,10-tetraazacyclododecane-N,N',N'',N'''-tetraacetic acid0 (DOTA), Tyr3-octreotate; 90Y DOTATOC: [90Y-DOTA]-D-Phe1-Tyr3-octreotide. 1. Kwekkeboom DJ et al. J Clin Oncol. 2008;26:2124-2130. 2. Waldherr C et al. Ann Oncol. 2001;12:941-944.](/image/15036/0/asset_1_15036.png)
Peptide Receptor Radiotherapy (PRRT)
Systemic radiotherapy targeting somatostatin receptors
Compounds vary by isotope and carrier molecule
177Lu DOTATATE(1) and 90Y DOTATOC(2) more frequently used
RR (0-37%) is higher in pNET compared to midgut NET.
The use of PRRT is after failing the first line medical therapy.
The presence of expression of SSRT2 is a prerequisite for the use of PRRT.
A better effect is reported with increasing SSTR expression according to SRS.
Serious side effects: severe bone marrow disease, kidney failure, liver failure.
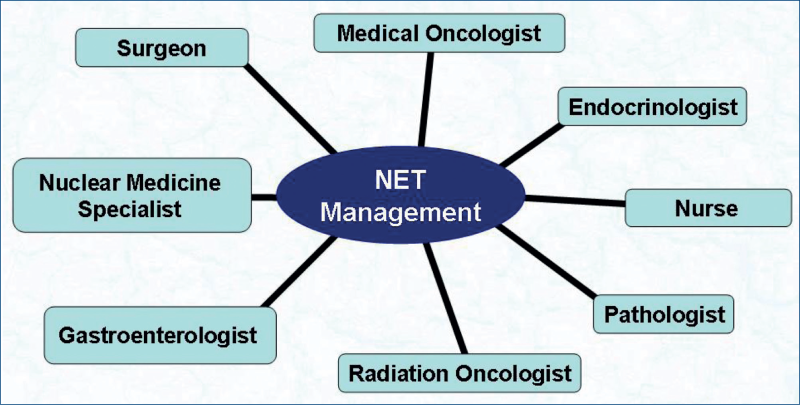
Multidisciplinary approach in the management of NETs

Cancerul şi obezitatea - implicaţii etiopatogenice, clinico-evolutive şi terapeutice
Ciprian Cirimbei, Elena Chitoran, Oana Păvăleanu, V. Rotaru, D. Straja
Obezitatea constituie un factor cu impact major în dezvoltarea unor cancere genitale şi digestive, cu mecanisme etiopatogenice parţial elucidate, dar implică totodată şi o diagnoză uneori mai dificilă, precum şi un parcu...
Cancerul, o problemă nerezolvată
Doru Paul
Pornind de la ideea că eşecul nostru de a vindeca cancerul vine din lipsa noastră de a înţelege complexitatea sa, ştiinţa contemporană priveşte trei modele principale pentru înţelegerea cancerului: 1. xenobiontul, 2. simbiontul, 3. oncobiontul. Fiecare prototip va fi detaliat cu suişuri, aşteptări şi nereuş...
Cele mai importante toxicităţi ale chimioterapicelor folosite în tratamentul tumorilor solide
Alexandru Grigorescu
Principalele toxicităţi induse de chimioterapia tumorilor solide sunt: toxicitatea hematologică (anemia, leucopenia, trombopenia) şi cea nonhematologică (cardiotoxicitatea, neurotoxicitatea, toxicitatea digestivă). Acest...
Advancements of immunotherapy in gastrointestinal cancers: a review of clinical evidence
Alexandra Pușcașu, Ioana Luca, Alexandru Grigorescu
Imunoterapia a revoluționat tratamentul cancerelor gastrointestinale, inhibitorii punctelor de control imun (ICI) jucând un rol crucial în îmbunătățirea supraviețuirii în diverse malignități....