Full zirconia single tooth fixed prosthetic restorations obtained through CAD/CAM technology – technological and practical aspects (Part II)
Aspecte tehnologice privind confecţionarea restaurărilor protetice fixe unidentare din zirconiu (full zirconia) prin metoda CAD/CAM – partea a II-a
Abstract
The CAD/CAM technology is an innovative alternative in dental prosthodontic that ensures a high quality for all types of prosthetic restorations, with a superior esthetic and functional result. The purpose of this study is to highlight the advantages that emerge from the use of this new technique, regarding precision and accuracy, and also the use of new materials and devices in the manufacture of full zirconia single tooth fixed prosthetic restorations.Keywords
single tooth prosthetic restorationsCAD/CAMfull zirconiaRezumat
Tehnologia CAD/CAM reprezintă o alternativă inovatoare în protetica dentară, ce asigură o calitate maximă pentru toate tipurile de tratamente protetice restaurative, cu un rezultat estetic şi funcţional superior. Acest articol are ca obiectiv principal evidenţierea avantajelor pe care le aduce folosirea acestei noi tehnici, precizia şi acurateţea realizării pieselor protetice, precum şi utilizarea de materiale şi aparate avansate în confecţionarea restaurărilor protetice fixe unidentare din zirconiu (full zirconia).Cuvinte Cheie
restaurări protetice fixe unidentareCAD/CAMfull zirconiaIntroduction
As mentioned in the first part of this material, CAD/CAM technology has become one of the most widely used techniques in dentistry. Practically, CAD/CAM technology represents the direction and orientation in dental practice of the future, both for dental office and for dental laboratory. Concretely, this article has as its main objective the highlighting of the advantages brought by the use of this new technique, the precision and accuracy of the production of prosthetic parts, as well as the use of advanced materials and devices in the manufacture of full zirconia single tooth fixed restorations (full zirconia)(1-4).
Single tooth fixed prosthetic restorations represent a long-term prosthetic therapeutic alternative which is recommended depending on a multitude of factors, such as the experience of the dental team (dentist and dental technician), clinical and technical equipment, general health status of the patients, but also their financial situation and availability. But one thing is certain about single tooth fixed prosthetic restorations: they offer patients who opt for this type of dental treatment a wide range of advantages, both in terms of functionality and comfort, as well as in terms of esthetics(1-4).
General data
Single tooth fixed prosthetic restorations are prosthetic works that morphologically and functionally restore a single tooth, partially or totally affected by volumetric, color or positioning changes(1-4). Specifically, the main properties of these types of prosthetic restorations are the following(1-4):
-
they are high-precision restorations obtained following a rigorous technological flow;
-
they are small prosthetic parts with a volume at most equal to that of the crown of a tooth or smaller;
-
they are made with the help of the dental laboratory;
-
they protect the underlying dental tissue, the marginal and supporting periodontium of the abutment tooth.
The technology for manufacturing these types of prosthetic restorations using the CAD/CAM method is not only a technology of the future, but also an innovative alternative in dental prosthodontics which ensures maximum quality for all types of restorative prosthetic treatments, with a superior esthetic and functional result(1-4).
In this second part of the article, two types of single tooth prosthetic restorations made of zirconia (full zirconia) will be presented, located in the transition region between the frontal and lateral region of the maxillary dental arch (a maxillary premolar), and in the lateral region of the dental arch (a mandibular molar), all prosthetic restorations being made using digital CAD/CAM technology.
Case presentations
Case 1
A 46-year-old male patient came to the dental office wishing to esthetically restore the upper first premolar 2.4 with the help of a full zirconia crown. The tooth suffered a coloristic change after a laborious endodontic treatment, losing its physiognomic appearance. The clinical stage of preparing the dental abutment was carried out by the dentist in the dental office, and later, in collaboration with the dental technician, all the necessary operations were carried out for the fabrication of fully physiognomic zirconia prosthetic restorations, made by CAD/CAM technology.
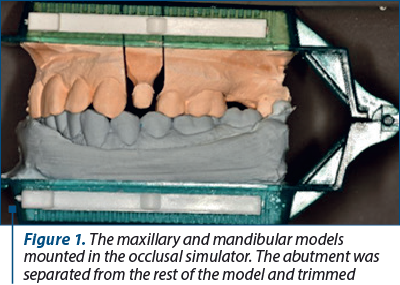
The impression of the abutment was made using condensation silicone in double consistency (putty and light body) in occlusion. The impression was sanitized and disinfected, following the protocol recommended by the manufacturers. Class IV die stone was used for casting the maxillary functional model, and class III die stone was used for casting the mandibular model, using a quadrant articulator. After the mounting, the maxillary model was sectioned and trimmed to highlight the abutment (Figure 1).
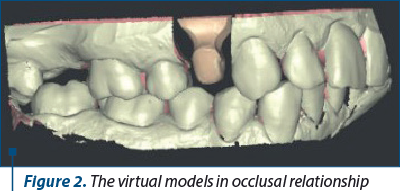
The models were scanned first individually and then together positioned in occlusal relationship. The two virtual models were obtained and also the correct spatial positioning. Thus, the computer has a clear image of prosthetic field and can design a highly accurate pattern of the prosthetic restoration (Figure 2).
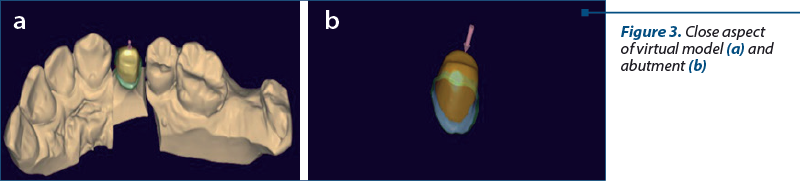
The virtual model was processed to highlight the edge of the preparation, which is necessary to create a correctly marginally fitted pattern (Figure 3 a and b).
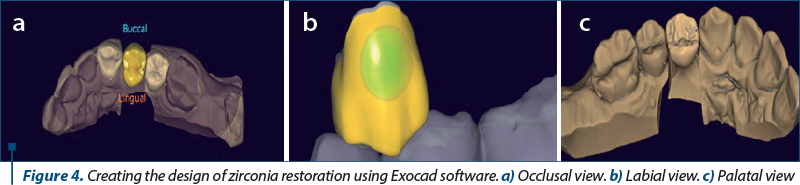
Once the margins of the preparation were established, the design of the restoration was made; the main areas of interest were occlusal surface and contact points with neighboring teeth (Figure 4 a, b and c).
At the end of design stage, the virtual pattern was placed on the virtual image of zirconia disk and all the data were sent to the milling machine to obtain the raw prosthetic restoration (Figure 5 a and b).
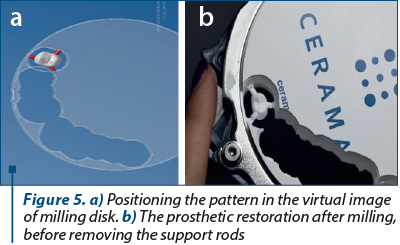
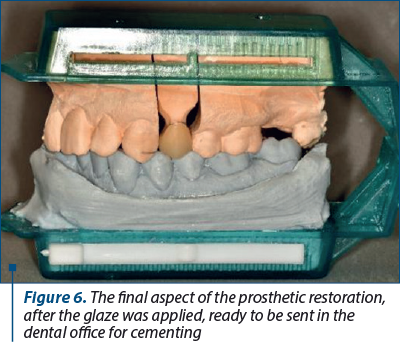
The raw restoration obtained from the milling process is trimmed, adapted on the physical model and color adjusted. The glaze layer is applied before sending the restoration to the dental office (Figure 6).
Case 2
A 42-year-old male patient presented to the dental office for prosthetic rehabilitation at the level of tooth 3.6. Thus, the dentist, in full agreement with the patient, decided to carry out an endodontic treatment at the level of tooth 3.6 and then to make a single tooth prosthetic restoration, a fully physiognomic crown made of zirconia, for a correct esthetic and functional result.
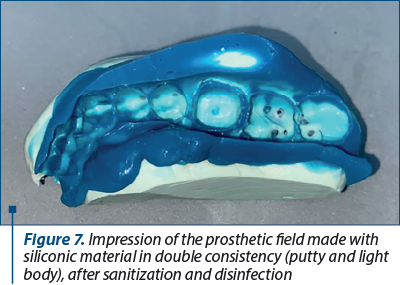
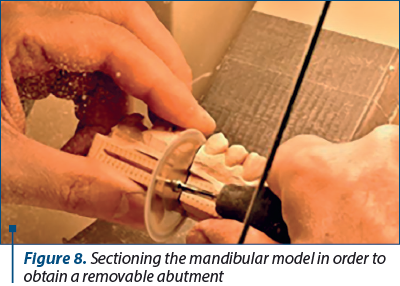
The impression of the prosthetic field was made using condensation silicone in double consistency (putty and light body), using the dual arch impression technique (Figure 7). Following the protocol recommended by the manufacturers, the impression was sanitized and disinfected. The mandibular model was cast using type 4 die stone, while for the maxillary model, type 3 die stone was used. The models were mounted in a quadrant articulator, and the mandibular model was sectioned and trimmed. Thus, the abutment was well highlighted, especially the marginal area (Figure 8).
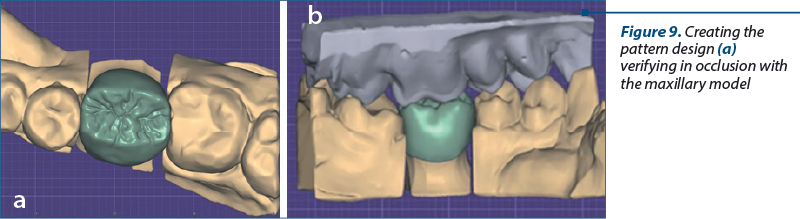
The models were scanned, individually and in occlusion, to obtain the virtual models in a correct spatial position. The virtual pattern design was conceived and adjusted in accordance with the maxillary model (Figure 9 a and b).
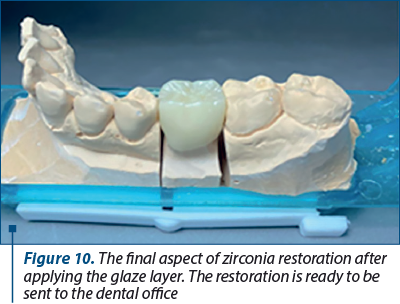
Once the desired design is achieved, the data are sent to the milling machine in order to obtain the raw shape of the restoration. The restoration was processed and obtained the final shape. A final check was made on the physical model before sending to dental office (Figure 10).
Discussion
The use of zirconia in dentistry appeared with the development of CAD/CAM technologies which allowed the use of a wider range of materials for creating prosthetic restorations. The main advantage of zirconia is the matte appearance, which can cancel out the unsightly color of the dental abutments, natural or as metallic cast post and core or metal abutments for implant supported restorations(5). The esthetic appearance made zirconia restorations to be used predominantly in the frontal area in the form of crowns or veneers.
Expanding the research, the dimensions necessary for the safe use of zirconia in the lateral area were established(6), thus expanding the range of clinical recommendations for fixed prosthetic restorations made of zirconia(5). Whether it is the transition area between the frontal and the lateral area, or the lateral area, zirconia restorations can be used safely, offering at the same time mechanical strength and esthetics(7).
The esthetics in the case of monolithic zirconia is obtained mainly by the basic shade of the disc used, but also with small corrections that can be made using the glaze layer(5,7-9). The mechanical strength is given by the thickness used for this type of restorations but, nevertheless, there is a risk when they are used in the lateral area, represented by microfractures that occur with chipping of the restorations(9-12). This can be avoided by a rounded edge design and proper occlusal balancing(13).
Conclusions
CAD/CAM technology offers many advantages to the dental laboratory, by automating manufacturing procedures with an increased quality, in a shorter period of time.
This technique is in continuous evolution, and its goals are precise and of real help in the field of dental medicine, by increasing the efficiency of dental treatment, standardizing prosthetic restorations, developing new groups of materials and new concepts of dental treatment.
Prosthetic restorations on zirconia infrastructure are easier, in contrast to prosthetic restorations made on a metal support, and the adaptation to the new prosthetic work is faster.
Acknowledgement. Viorel Ştefan Perieanu and Manuela Popescu are the corresponding authors and have an equal contribution with the first author.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Bereşescu G. Dinţii umani permanenţi. Editura University Press, Târgu-Mureş, 2011.
-
Nelson SJ, Ash MM. Wheeler’s Dental Anatomy, Physiology and Occlusion. 9th Edition. St. Louis: Saunders Elsevier, 2010.
-
Bratu D, Nussbaum R. Bazele clinice şi tehnice ale protezării fixe. Ediţia a 3-a. Ed. Medicală, Bucureşti, 2011.
-
Forna N, de Baat C, Bratu D, Mercut V, Petre A, Popşor S, et al. Protetică dentară. Ediţia I. Vol. II. Ed. Enciclopedică, Bucureşti, 2011.
-
Tabatabaian F. Color in Zirconia-Based Restorations and Related Factors: A Literature Review. J Prosthodont. 2018;27(2):201-211. doi:10.1111/jopr.12740.
-
Dal Piva AMO, Tribst JPM, Benalcázar Jalkh EB, Anami LC, Bonfante EA, Bottino MA. Minimal tooth preparation for posterior monolithic ceramic crowns: Effect on the mechanical behavior, reliability and translucency. Dent Mater. 2021;37(3):e140-e150. doi:10.1016/j.dental.2020.11.001.
-
Lawson NC, Frazier K, Bedran-Russo AK, et al. Zirconia restorations: An American Dental Association Clinical Evaluators Panel survey. J Am Dent Assoc. 2021;152(1):80-81.e2. doi:10.1016/j.adaj.2020.10.012.
-
Laumbacher H, Strasser T, Knüttel H, Rosentritt M. Long-term clinical performance and complications of zirconia-based tooth- and implant-supported fixed prosthodontic restorations: A summary of systematic reviews. J Dent. 2021;111:103723. doi:10.1016/j.jdent.2021.103723.
-
Tang Z, Zhao X, Wang H, Liu B. Clinical evaluation of monolithic zirconia crowns for posterior teeth restorations. Medicine (Baltimore). 2019;98(40):e17385. doi: 10.1097/MD.0000000000017385.
-
Miyazaki T, Nakamura T, Matsumura H, Ban S, Kobayashi T. Current status of zirconia restoration. J Prosthodont Res. 2013;57(4):236-261. doi:10.1016/j.jpor.2013.09.001.
-
Çömlekoğlu ME, Tekeroğlu F, Dündar Çömlekoğlu M, Özcan M, Türkün LŞ, Paken G. Clinical wear and quality assessment of monolithic and lithium disilicate layered zirconia restorations. Aust Dent J. 2021;66(4):413-422. doi:10.1111/adj.12869.
-
Sulaiman TA, Abdulmajeed AA, Donovan TE, Cooper LF, Walter R. Fracture rate of monolithic zirconia restorations up to 5 years: A dental laboratory survey [published correction appears in J Prosthet Dent. 2017 Jan;117(1):195]. J Prosthet Dent. 2016;116(3):436-439. doi:10.1016/j.prosdent.2016.01.033.
-
Abdulmajeed AA, Donovan TE, Cooper LF, Walter R, Sulaiman TA. Fracture of layered zirconia restorations at 5 years: A dental laboratory survey. J Prosthet Dent. 2017;118(3):353-356. doi:10.1016/j.prosdent.2016.11.009.

Laureaţii primei ediţii a Galei Elitelor Medicale în Otorinolaringologia Românească
Două evenimente de excepţie în domeniul otorinolaringologiei au avut loc, în data de 21 aprilie, la Cluj-Napoca. Este vorba despre Forumul „Progrese şi Excelenţă în Otorinolaringologie” şi Gala Elitelor Medicale în Otorinolaringologia Românească, ambele desfăşurate sub egida Societăţii Române de Foniatrie. ...
Technological aspects in the reconstruction of the dental abutment with post and core restoration using the indirect method: modern versus digital
Camelia Ionescu, Andreea-Elena Vrabie, Radu Cătălin Costea, Viorel Ştefan Perieanu, Manuela Popescu, Mădălina Violeta Perieanu, Liliana Burlibaşa, Ileana Ionescu, Mihai Burlibaşa
Pierderea unei cantităţi semnificative de ţesuturi dure dentare de la nivel coronar impune utilizarea unui dispozitiv coronor...
Rare clinical features in non-Hodgkin lymphomas of the head and neck
Anca-Ionela Cîrstea, Daniela Vrînceanu, Raluca Grigore, Dumitru Mihai, Maria Dana Gheorghiev, Miruna Bratiloveanu, Nicoleta Măru
Limfomul este cel de-al doilea diagnostic malign, după carcinomul scuamos, cu localizare la nivelul capului şi gâtului. Cea mai frecventă formă de manifestare a limfoamelor din sfera ORL este cea...
Technological aspects in the reconstruction of the dental abutment with post and core restoration using the indirect method: modern versus digital
Camelia Ionescu, Andreea-Elena Vrabie, Radu Cătălin Costea, Viorel Ştefan Perieanu, Manuela Popescu, Mădălina Violeta Perieanu, Liliana Burlibaşa, Ileana Ionescu, Mihai Burlibaşa
Pierderea unei cantităţi semnificative de ţesuturi dure dentare de la nivel coronar impune utilizarea unui dispozitiv coronor...
Veneering with ceramic masses of single tooth prosthetic restorations in lateral areas (Part II)
Mihai David, Valentin-Dănuţ Albu, Viorel Ştefan Perieanu, Cristina-Maria Şerbănescu, Mircea Popescu, Florentina Căminişteanu, Oana Elena Amza, Maria Antonia Şteţiu, Mihai-Alexandru Stoica, Mihai Burlibaşa, Mihaela Chirilă
Scopul acestui material este de a expune faptul că, prin utilizarea maselor ceramice, se obţin rezultate deosebite în realizare...