Învăţăminte desprinse din îngrijirea unui flegmon retroesofagian cervico-mediastinal superior tratat în echipă multidisciplinară chirurgicală
Lessons learned from the care of a retroesophageal cervical mediastinal phlegmon treated in the multidisciplinary surgical team
Abstract
The purpose of the paper work. To highlight the severe suppurative cervicomediastinal complications after perforating the cervical esophagus with a sharp foreign body.Objectives of the paper work. To underline the importance of clinical and imagistic diagnosis and the treatment of the cervical medial topographic region with multidisciplinary surgical team: ENT, thoracic surgeon, general surgeon and AIT physician.
Materials and method. A 72-year-old patient swallowed a fish bone while eating, with the immediate appearance of a cervical pain with stinging, dysphagia and sore odynophagia.
Results and discussion. The patient was hospitalized in emergency 24 hours after the ingestion of the sharp foreign body, presenting with cervical emphysema and leukocytosis 18.000/mm³. CT showed retroesophageal cervical and postero-superior mediastinal collection. The emergency surgical intervention under general anesthesia, with a mixed surgical team, evacuated the purulent collection by antero-inferior cervicotomy, with a drainage aspiration Redon tube, gastrostomy and massive antibiotic treatment for Klebsiella pneumoniae. Daily antiseptic lavage was performed on the aspiration tube for 4 weeks, which led to the suppression of gastrostomy after 6 weeks.
Conclusions. The emergency surgery, performed with a multidisciplinary, competent and professional team, has been associated with massive and targeted antibiotic treatment and cervical dressings, performed under septic conditions, and leading to the heal of the cervical mediastinal suppuration.
Keywords
cervicomediastinal phlegmonRedon aspiration drainagegastrostomyRezumat
Scopul lucrării. Evidenţierea complicaţiilor supurative grave cervico-mediastinale prin perforarea esofagului cervical de către un corp străin ascuţit.Obiectivele lucrării. Importanţa diagnosticului clinic şi imagistic şi al tratamentului regiunii topografice cervico-mediastinale cu implicare multidisciplinară chirurgicală: ORL-ist, chirurg toracic, chirurg generalist, radiolog şi medic ATI.
Materiale şi metodă. O pacientă de 72 de ani a înghiţit în timpul mesei un os de peşte, cu apariţia imediată a durerilor cervicale, cu înţepături, disfagie şi odinofagie.
Rezultate şi discuţii. Pacienta a fost internată de urgenţă la 24 de ore de la ingestia corpului străin ascuţit, cu emfizem cervical şi leucocitoză 18000/mm³. CT-ul a evidenţiat o colecţie retroesofagiană cervicală şi mediastinală postero-superioară. Intervenţia chirurgicală de urgenţă, sub anestezie generală, în echipă mixtă chirurgicală, a evacuat colecţia purulentă prin cervicotomie antero-inferioară, montare de dren aspirativ Redon, gastrostomă de alimentaţie şi tratament antibiotic masiv pentru Klebsiella pneumoniae. Lavajul zilnic cu substanţe antiseptice pe tubul aspirativ, timp de 4 săptămâni, a condus la suprimarea gastrostomei la 6 săptămâni.
Concluzii. Intervenţia chirurgicală de urgenţă, în echipă multidisciplinară, competentă, profesională, cu tratament antibiotic ţintit masiv şi pansamente cervicale efectuate în condiţii de asepsie maximă, a condus la vindecarea supuraţiei cervico-mediastinale.
Cuvinte Cheie
flegmon cervico-mediastinaldrenaj aspirativ Redongastrostomă de alimentaţieIntroduction
The esophagus, a food transit organ, has a 4-mm thick membranous muscular structure located in front of the vertebral bodies from C6 to T10-T11. At the esophagus level, trauma can occur due to accidental ingestion of the sharp foreign bodies, which escapes swallowing from the oral cavity. Foreign bodies can cause lesions of varying degrees, from mucosal involvement to hemorrhage due to bite of esophageal wall with perforation.
The symptomology of esophageal perforation is manifested by:
- cervical, retrosternal or epigastric pain of high intensity;
- dysphagia, marked with the impossibility of swallowing;
- subcutaneous cervicothoracic emphysema.
The positive diagnosis of esophagus perforation is established on the following elements:
- clinical elements revealed by anamnesis and mentioning the onset of symptoms during nutrition;
- objective exam given by subcutaneous emphysema;
- imagistic exam: the diagnosis is confirmed by the CT scan which highlights the subcutaneous cervical emphysema, mediastinal, pleural, or epigastric, as well as the presence of suppuration, depending on the perforation place.
The treatment of esophageal perforation is aimed at preventing complications by putting the esophagus into absolute fasting with general-wide antibiotic therapy. The appearance of post-perforation supurative collections benefits from emergency surgery evacuation and drainage with the help of the multidisciplinary team: ENT, thoracic surgeon, general surgeon, anesthesiologist and AIT physician.
We dealt with a case of esophageal perforation by a foreign body represented by a fish bone (carp) which led to the formation of a cervical and mediastinal retroesophageal collection, and we want to share some surgical and postoperative care items that led to the healing of the patient.
Clinical case presentation
A 72-year-old female patient, O.M., is urgently hospitalized on 9.03.2016 by transfer from Emergency Clinical Hospital of Slatina for dysphagia and odynophagia that occurred suddenly 24 hours ago after eating carp at lunch.
Esophagoscopy was performed in Slatina and the foreign body was not able to be visualized because of the massive bleeding. Emergency pulmonary radiography (967/9.03.2016) showed basal pulmonary fibrosis. Cord was within normal limits.
The esophagoscopy was also attempted in Craiova, under general anesthesia, but because of the important edema of the esophagus mucosal, accompanied by bleeding, it could not penetrate into the lumen of the esophagus. Antibiotic, antialgic, infusible and absolute esophageal diets were instituted. In the following hours, large cervical pains and subcutaneous cervical emphysema occurred, with gassing cracking on palpation.
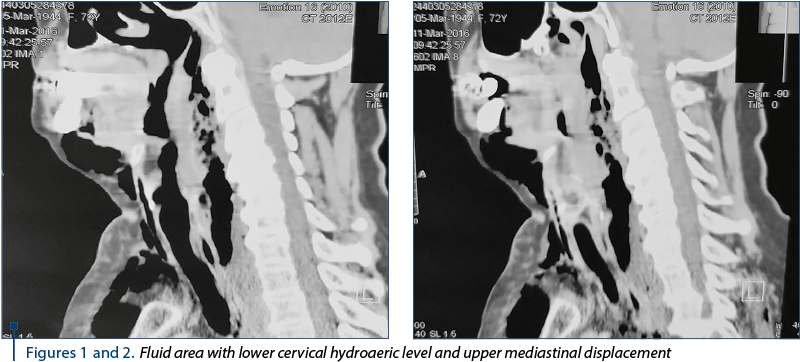
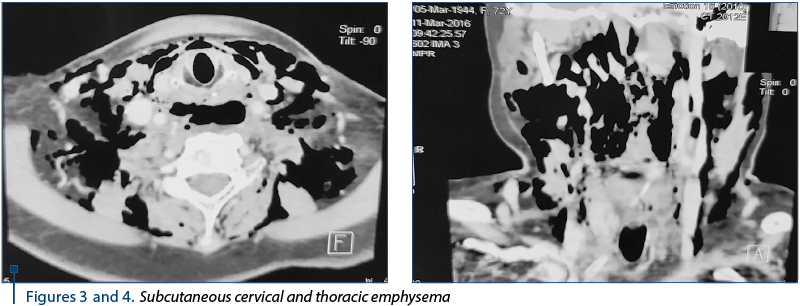
The urgent CT scan (2773/11.03.2016) revealed the diffuse thickening of the upper cervical and thoracic esophagus wall, with the delimitation of a fluid, inhomogeneous, diffusely delimited area with hydroaeric (Figures 1 and 2), cervical inferior and superior mediastinal visual (C5-T4) displayed posterolateral as it compressed the esophagus and partly the posterior wall of the trachea. Diffuse perilaryngeal infiltration with diminishing the laryngeal lumen, the infracentimetric hyper density zone of the suspected cervical inferior body (C7) anterolateral left in relation to esophageal wall; subcutaneous emphysema is marked on the cervical, thoracic and middles and posterior mediastinal level in the upper third (Figures 3 and 4). Bilateral pleural fluid. No changes in pulmonary transparency.
Laboratory examinations: the blood counts were 18.500/mm³ leukocytes and 30/55 mm VSH. With the diagnosis of cervical and thoracic retroesophageal phlegmon with supero-posterior mediastinitis, secondary to the perforation of the cervical esophagus through a sharp foreign body, surgical emergency was performed with the help of the multidisciplinary team (ENT, thoracic surgeon, general surgeon) under general anesthesia.
Because of the cervical swelling in the lower half of the neck, the incision was made in “U” starting from the antero-inferior margin of the sternocleidomastoidian right muscle, descending into the sternum fork and climbing to the left of the sternocleidomastoidian muscle.
The cervical musculoaponucleotide spaces of the air bubbles were dissected and debrided; the emphysema between the sternocleidomastoid muscle and the laryngeal tracheal duct made it easy to penetrate the vertebral column. Inspiration of digital dissection between the vertebral bodies C5 - C6 - C7 and the esophagus posterior wall revealed the purulent, yellowish cervical phlegmon collection, intensely fetid and aerated; pounds mixed with air bubbles. Pus was collected for bacteriological and antibiotic examination. The debridement of the retroesophageal space, both cervical and thoracic, was continued, from which 200 ml of large pus was discharged. On the posterior wall of the cervical esophagus and on the anterior face of the C6 - C7 vertebral bodies, the presence of fake membranes, blackish, puffy, odorless feathery, adherent, expanded and on the posterior side of the right sternocleidomastoid muscle, was found to be up to one third of herself. The retroesophageal cavity was disinfected with chlorhexine and betadine.
The cervical and thoracic retroesophageal cavity was drained with a silicon tube number 24 that was connected to the Redon aspiration device. The silicone tube was attached to the silk threaded flap. The cervical plexus was left open, being daily patented with local antibiotic (Sinerdol), disinfectant solutions and sterile compresses.
After cervical wound dressing with sterile compresses, Storz tube esophagoscopy was performed, which revealed the esophagus full of purulent secretions and false membranes that were aspirated.
On the posterior wall, about 1.5 cm from the mouth of the esophagus, the esophageal wall burglary with false membranes was observed to remove purulent secretions. The foreign body was not detected swiftly at the site of the esophagus or below. Surgery was continued by general surgeons who mounted the 40-piece Pezzer probe on the anterior face of the gastric body, and the patient would feed on gastrostomy.
The patient received postoperative antibiotic treatment according to Klebsiella sensitivity to meropenem, metronidazole and ciprofloxacin.
Local cervical wound care was performed daily (Figures 5, 6 and 7) following the strictest aseptic standards. This is how to dress the cervical wound: after removing the cervical dressing and dressing the edges of the cervical wound, isolate the wound with sterile fields. In addition to the adjacent silicone aspiration tube, a sterile probe was inserted into the mediastinum, instilled with antiseptics which were aspirated by means of a sterile syringe from the silicone tube and connected to another sterile aspiration device. The purulent aspiration secretion in the Redon device within 24 hours never deposited 10 ml and progressively decreased to a few drops on the silicone tube for 25 days.

The postoperative follow-up of the evolution of cervicomediastinal suppuration was made by leukocyte, VSH and DST values, that normalized, and implicitly the CT imaging.
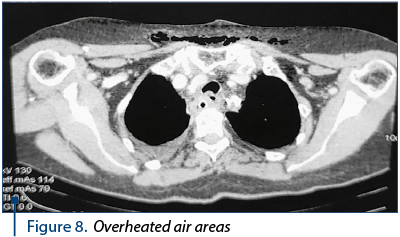
The CT scan 2944 performed on March 16, 2016, at five days postoperatively, consisted of the diffuse infiltration of the retrolaryngeal mass with a mass effect at the laryngeal level and the left anterolateral dislocated esophagus with diffuse parietal thickening; cervical posterior air areas with mediastinal-cervical drainage (Figure 8); posterior mediastinal infiltration zone in the upper and middle third adjacent to the esophagus. Bilateral pleural fluid. Gastrostomy present; subcutaneous emphysema of the cervical and thoracic region.
The evolution of the general condition of the cervical wound was favorable, but the persistence of secretion from the aspiration device required a reevaluation of the DST, which was sterile.
The CT scan (3296/25.03.2016) highlighted the airborne area, with irregular contour, posterior cervical posterior and posterior mediastinal adjacent to the esophagus and drainage tube, the diameter of the 2/1.2 cm centimeter posterior cervical with the burglary of the contrast substance administered orally at this level and minimal peripheral diffusion infiltration without fluid collections constituted cervicomediastinal. Infiltration of the anterolateral cervical soft parts adjacent to the drain tube. No suspect contrast sockets. No changes in pulmonary transparency. Bilateral pleural fluid blade.
Thirty days of medical care and five days of stopping the drains on the drainage tube are performed, with radiological exploration by oral contrast agent administration. The cervical esophagus of normal appearance, without fistulous traits, was noticed. Minimum stasis in the right pyrimiform sinus. Thoracic esophagus with tertiary contractions in the lower third. Stomach – hypotonic, hypokinetic, with faces, curves and folds of normal appearance.
At 30 days postoperatively, the silicone cervical mucous membrane tube was suppressed, and the gastrostomy probe was removed at 40 days.
Discussion
The presentation of the retroesophageal cervicomediastinal phlegmon case with the diagnosis assessment and the established therapeutic attitude reveals that the esophageal primate suppuration is very serious. The gravity of the suppression comes from the flora rich in germs with esophageal location. Being aware of the gravity of the esophageal supine, we consulted with those involved in the otorhinolaryngology - thoracic surgery - general surgery pathology. From the presentation of this case, every surgical specialty involved had to learn from the other.
We worked in a multidisciplinary team, where everyone has solved his affected organ: the otorhinolaryngologist incised the cervical region to reach the retroesophageal collection that was evacuated. Applying the silicone drain to the upper mediastinum, as well as the daily lavage route adjacent to the tube belonged to the chest surgeon. General surgeons were responsible for making gastrostomy for feeding complex food principles and tracking the progression of abdominal wounds.
The dressing of the cervical region was given to the otorhinolaryngologist, and the maintenance of asepsis caused the cervical plague, including drainage, to evolve favorably.
The cervical lump has gradually scarred from top to bottom; when removing the silicone tube, it resumed its place, completely covering the underlying cervical region. No suture was required per second, strip sterile strips were applied to the lower pole of the cervical flap.
The mode of aspiration of cervical mediastinal secretion and the detachment of the tube connected to the Redon aspiration drainage device were performed according to the suggestion of the thoracic surgeon.
In these maneuvers, all the doctors involved in the operation participated, even though the patient was hospitalized successively in the clinics: ENT, thoracic surgery and later general surgery. Interdisciplinary collaboration was carried out in full professional respect, with conscientiousness, competence, following rigorously the rules of asepsis, sterile collection of cervical and diastolic secretion and application of sterile cervical dressing. Paying attention to a serious illness through interdisciplinary involvement led to the clinical and surgical healing.
Concomitantly with the patient’s surgical care, she was treated by the reanimation anesthesia physician for cardiac, hepatic, renal, antibiotic complex, as long-term antithrombotic therapy had no repercussions.
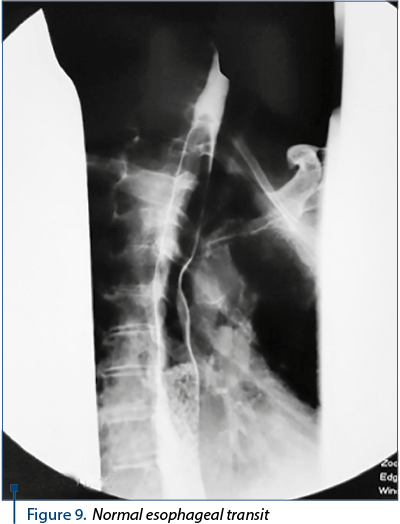
The success we had with the healing of this serious case has led us to consider the condition of the esophagus and the way of eating naturally within 6 months. The esophageal contrast-transient study revealed the lumen of the esophagus, without the stenosis area, with preserved morphology (Figure 9).
The biological constants were within normal limits, and cervical and abdominal postoperative scars healed (Figures 10 and 11). The gravity of the esophageal and pharyngeal suppurations with mediastinal extension is presented by Romanian authors (1,7,8,10,11) and foreign authors(2,3,4,5,6,9) in various articles published, including a monograph.

Conclusions
- The ingestion of a sharp esophageal foreign body exhibits severe suppurative complications.
- The esophageal food stop is the first step in the case of ingestion of sharp bodies, as well as antibiotic treatment.
- The perforation of the esophageal wall exposes to severe cervical, mediastinal or abdominal coughing.
- The interest of the cervical and mediastinal regions requires the involvement of several surgical and reanimation specialties.
- Surgical intervention in suppurative esophageal complications has an urgent indication.
- Postoperative care, done with competence, professionalism and medical dedication, leads to therapeutic success.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Costinescu V, Stegaru C. Cervical and cervical-mediastinal suppurations – Monograph. "Gr.T. Popa" Publishing House. UMF Iaşi 2007.
- Gehanno P. Extensive cervical-mediastinal cellulite. The ENT Notebooks. 1996. T. XXXIII no 6. 303.
- Herman P, Kici S, Portier F. Extensive cervical cellulitis. Emergencies in ENT. Report of the French Congress. 2002. p. 163–169.
- Herman P, Kici S. Necrotizing mediastinitis of dental and/or pharyngeal origin - ENT emergencies. Report of the French Congress. 2002. p. 171–174.
- Nagy M, Pizzuto M, Backstrom J, Brodsky L. Deep neck infections in children: a new approach to diagnosis and treatment. Laryngoscope. 1997. 107: 1627–1634.
- Portier F, Herman P. Adenitis and adenophlegmon - ENT emergencies. French Report Congress. 2002. p. 155-162.
- Costinescu VN. Optimization of treatment in serious cervical and cervical-mediastinal disorders. ORL.ro. 2008. "Cervical and Facial Pathology", 1st year, no. 1, November 2008. p 14-18.
- Stegaru G, Costinescu V. Particular clinical and therapeutic aspects of cervical-mediastinal suppuration. Clinica. 1998. vol. III nr.1, p 25-26.
- Wetmore RF, Mahboubi S, Soyupak SY. Computed tomography in the evaluation of pediatric neck infections. Otolaryngol Head Neck Surg. 1998. 119: 624-627.
- Obreja S, Ioniţă E, Ioniţă I, Mitroi M. Perforaţia esofagului, In: "Lexicon al diagnosticului în ORL", vol II. Ed. Didactică şi Pedagogică. 1998. p 193–196.
- Obreja S, Ioniţă E, Ioniţă I, Mitroi M. Corpi străini esofagieni, In: "Lexicon al diagnosticului în ORL", vol I. Ed. Didactică şi Pedagogică. 1998. p. 273–276.

Lista rezumatelor lucrărilor susţinute in cadul celei de-a X-a ediţii a Forumului ORL.ro 2018
Lista rezumatelor lucrărilor susţinute in cadul celei de-a X-a ediţii a Forumului ORL.ro 2018...
Vertijul paroxistic poziţional benign (VPPB)
Mădălina Georgescu
Ameţeala reprezintă un simptom foarte frecvent întâlnit în practica generală (5% din consultaţiile de medicină generală, conform datelor Organizaţiei Mondiale a Sănătăţii). Etiologia acestei simptomatologii este extrem de variată. De aceea, abordarea pacientului cu ameţeală trebuie făcută cu multă atenţie, an...
Sindromul Moebius sau „frozen face“
Mihaela Fotescu Zamfir, Andreea Lumpan
În acest articol ne propunem să facem o descriere a specificităţii sindromului Moebius, prezentând date generale şi un tablou clinic al pacientului cu acest sindrom, insistându-se asupra întârzierii în dezvoltarea globală şi punând accent pe tulburările de limbaj consecutive. Se prezintă un protocol de ab...
Histopathological and immunohistochemical aspects of the oropharyngeal neoplasm in the ENT Clinic, Craiova
Ioana-Cristina Oprişcan, Elena Ioniță, Carmen-Aurelia Mogoanţă, Florin Anghelina, Mircea-Sorin Ciolofan, Mihaela Mitroi, Alina-Nicoleta Căpitănescu, Iulică Ioniță, Irina Enache, Carmen Sîrbuleţ, Eduard-Andrei Gheorghe
Introducere. Cancerele capului şi gâtului ce includ neoplaziile ORL sau ale căilor aeriene şi digestive superioare reprezin...
The clinical-epidemiological study of oropharyngeal neoplasm – work carried out in the ENT Clinic of the Craiova County Emergency Clinical Hospital
Ioana-Cristina Oprişcan, Elena Ioniță, Carmen-Aurelia Mogoanţă, Florin Anghelina, Mircea-Sorin Ciolofan, Mihaela Mitroi, Alina-Nicoleta Căpitănescu, Iulică Ioniță, Irina Enache, Carmen Sîrbuleţ, Eduard-Andrei Gheorghe
Introducere. Neoplasmul orofaringian reprezintă în prezent una dintre principalele cauze de morbiditate la nivel mondial, iar pa...