Studiu endoscopic şi imagistic în polipoza nazală
Endoscopic and imaging study in nasal polyposis
Abstract
Endoscopic and imaging analysis of nasal polyposis is part of modern, specific methods of exploration. The objective of the study. To carry out an efficient description of the endoscopic and imaging characteristics in nasal polyposis cases. Purpose of the study. Trying to highlight the importance of complex examination for obtaining the correct diagnosis based on scales using a grading system. Materials and method. We evaluated a group of patients with bilateral nasal polyposis hospitalized in the ENT clinic of the County Emergency Clinical Hospital of Craiova over a period of 5 years, which underwent nasal endoscopy. A part of them also underwent cranial CT scan. Results. Using the Lildholdt grading system and the Lund-Kennedy scale, the nasal polyposis was graded in stages. The preoperative Lund-Kennedy scale had a minimum score of 3 and a maximum of 14, and postoperatively a minimum score of 0 and a maximum of 6. The Lund-Mackay score, analyzing patients with nasal polyposis associated with chronic allergic rhinosinusitis, obtained on the left side a mean score of 8 and on the right side an average score of 7. Conclusions. The analysis of the endoscopic and imaging parameters both preoperatively and postoperatively provided very valuable information for assessing the surgical treatment effects.Keywords
nasal polyposisendoscopicLildholdt grading systemLund-Kennedy scaleLund-Mackay CT scaleRezumat
Analiza endoscopică şi imagistică a polipozei nazale face parte din metodele de explorare moderne, de actualitate. Obiectivul studiului. Realizarea descrierii eficiente a caracteristicilor endoscopice şi imagistice ale afecţiunii polipoase. Scopul studiului. Încercarea de a evidenţia importanţa examinării complexe pentru obţinerea diagnosticului corect pe baza unor scale utilizând un sistem de gradare. Materiale şi metodă. Am evaluat un grup de pacienţi cu polipoză nazală bilaterală internaţi în clinica ORL a Spitalului Judeţean de Urgenţă din Craiova, pe o perioadă de 5 ani, cărora li s-a efectuat endoscopie nazală. La o parte din ei s-a efectuat şi CT de craniu. Rezultate. Utilizând sistemul de gradare Lildholdt şi scala Lund-Kennedy, polipoza nazală a fost încadrată în stadii. Scala Lund-Kennedy efectuată preoperatoriu a prezentat un scor minim de 3 şi un scor maxim de 14; postoperatoriu, scorul minim a fost 0, iar cel maxim – 6. Scorul Lund-Mackay, analizând pacienţii cu polipoză nazală asociată cu rinosinuzita cronică alergoinfectată, a obţinut pe partea stângă un scor mediu de 8 şi pe partea dreaptă un scor mediu de 7. Concluzii. Analiza parametrilor endoscopici şi imagistici, atât preoperatoriu, cât şi postoperatoriu, a furnizat informaţii deosebit de valoroase pentru aprecierea efectelor tratamentului chirurgical.Cuvinte Cheie
polipoză nazalăendoscopieseveritate Lildholdtscala Lund-Kennedyscala CT Lund-MackayIntroduction
In the 21st century, when medicine is mandatory evidence-based, and technological evolution allows to overcome the subjective barriers practiced in the past due to the lack of appropriate methods and facilities, the use of diagnostic and treatment protocols, which have the advantage of facilitating the practitioner’s activity, it becomes essential, by standardization, to correctly quantify the results of research and to give patients the greatest chance of benefit from efficient and personalized treatment. These criteria are also applicable in the case of a complex pathology represented by nasal polyposis, rarely a self-contained entity, often associated with allergic, infectious diseases, or combinations thereof. Nasal polyposis, along with the main intricate pathologies, is analyzed by both endoscopic and imaging point of view. Endoscopy is necessary for undisputable evaluation of the treatment for nasal polyposis(1). Various systems of evaluation of nasal polyps have been stated, although it is not always easy to differentiate between the nasal polyps and the normal pituitary mucosa(1).
Materials and method
Endoscopic methods
One of the most widely used methods of exploration in nasal polyposis is rigid nasal endoscopy. For this research, we used a rigid Karl Storz 4.0 mm nasal endoscope with a 300 angulation optic (other practitioners prefer 00 angulation).
One of the most important aspects that we have pursued through this exploration were the aspects described in the Lund-Kennedy scale, used both preoperatively and postoperatively (Figure 1a).
We also used an exploratory fiberscopy which is a repeatable, painless and minimally invasive procedure, available in both the ENT clinic and the outpatient department. Fiberscopy was also useful in allowing the follow-up of patients at 1, 3, 6 and 12 months, and then annually. The fiberscope we used was OPTOMIC OP-30, the technique being very similar to that described in the rigid nasal endoscopy (Figure 1b).

Lund-Kennedy scale (Lund-Kennedy Endoscopic Grading System – adapted from Önerci Metin T, 2010(2)) highlights the endoscopic findings:
-
Polyp, left side (0, 1, 2, 3)
-
Polyp, right side (0, 1, 2, 3)
-
Edema, left side (0, 1, 2)
-
Edema, right side (0, 1, 2)
-
Secretions, left side (0, 1, 2)
-
Secretions, the right side (0, 1, 2).
Starting from this system of scoring, we have also determined the Lund and Kennedy postoperative score to evaluate the final result, consisting in:
-
Scars, left side (0, 1, 2)
-
Scars, right side (0, 1, 2)
-
Crusts, left side (0, 1, 2)
-
Crusts, right side (0, 1, 2).
Total points
Polyps: 0 – absence of polyps, 1 – polyps only in the middle meatus, 2 – polyps that exceed the middle meatus but do not completely block the nasal fossa, 3 – polyps that completely obstruct the nasal fossa; Edema: 0 – absent, 1 – mild, 2 – severe; Secretions: 0 – no secretions, 1 – clear, aqueous secretions, 2 – thick, purulent secretions; Postoperative scars: 0 – absent; 1 – mild, 2 – severe; Crusts: 0 – absent, 1 – light, 2 – severe.
At the endoscopic exploration, we were able to apply the Lildholdt polyps grading system(1), of great help in determining the subsequent therapeutic conduct:
-
Grade 1 – small polyps that do not reach the upper edge of the inferior turbinate.
-
Grade 2 – polyps that are located between the upper edge and the lower edge of the lower turbinate.
-
Grade 3 – bulky polyps that extend beyond the lower edge of the inferior nasal turbinate.
Imaging methods
CT is the imaging exploration method of choice, because it is capable of providing the most important information regarding nasal polyposis. Thus, the main changes determined by this pathology are closely watched: influence of the bone architecture in the vicinity, extension of the disease, involvement of the papyrus lamina, the rhinobasis, the vascular report in the respective area and the consequences of strictures, establishing the differential diagnosis, the depth the polyps reached inside of the sinuses and how patients respond to treatment.
This medical-forensic imaging exploration has a capital value in choosing the therapeutic plan, especially from the surgical point of view.
Imaging exploration made possible the use of Lund-Mackay scoring system (adapted from Önerci Metin T., 2010(2)), which permitted granting characteristic scores for analyzing the changes produced by the nasal polyposis of each sinus. It consists in identifying the aspects of the paranasal sinuses on both right and left side:
-
Maxillary sinus (0, 1, 2)
-
Anterior ethmoidal sinus (0, 1, 2)
-
Posterior ethmoidal sinus (0, 1, 2)
-
Sphenoidal sinus (0, 1, 2)
-
Frontal sinus (0, 1, 2)
-
Osteo-meatal complex (0 or 2*).
-
Total
-
0 = no thickening of mucosa
-
1 = < total opacification
-
2 = total opacification.
* there is no value 1 score with regard to the osteomeatal complex
The final score thus obtained was computer analyzed with the purpose of obtaining statistical data and the most accurate orientation towards the complete and most efficient surgical treatment.
Results
1. The distribution of patients according to the Lildholdt grading system objectified by endoscopy had the following results, also shown in Figure 2.
Grade 1: small polyps that do not reach the upper edge of the inferior turbinate – 65 cases (17.42%).
Grade 2: polyps that are located between the upper edge and the lower edge of the lower turbinate – 89 cases (23.86%).
Grade 3: large polyps that extend beyond the lower edge of the inferior turbinate – 219 cases (58.71%).

2. The results according to the Lund-Kennedy scale performed preoperatively and postoperatively on the left side, respectively on the right side
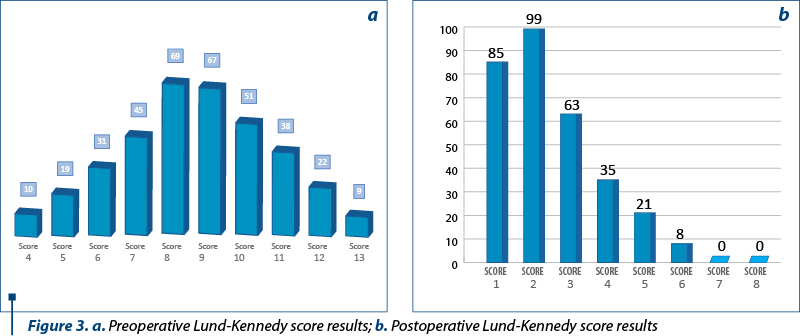
The minimum preoperative Lund-Kennedy score was 3 in a patient with nasal polyposis. This score consisted in the sum of value 1, determined by the presence of a polyp in the middle meat, unilaterally right or left, accompanied by moderate unilateral edema and clear aqueous secretions unilaterally, both being located on the same side, the latter receiving the value 1. We identified 7 cases by calculating the Lund-Kennedy score. The maximum preoperative Lund-Kennedy score was 14, found in 5 cases by summing the maximum values at each parameter analyzed bilaterally (polyp, edema, secretions). For each intermediate score (between 3 and 14) we highlighted the results in Figure 3a.
The postoperative Lund-Kennedy score was obtained by endoscopy performed at approximately 30 days in the outpatient setting and had a 0 value in 62 patients, with scabs and scars absent bilaterally. The rest of the patients scores are detailed in Figure 3b.
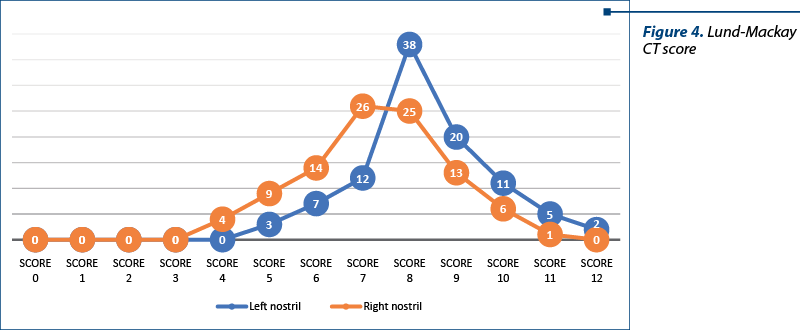
3. The results obtained by the Lund-Mackay score for paranasal sinuses CT imaging on the right side and the left side
This grading system was used for the purpose of evaluating patients with chronic rhinosinusitis allergic-infected and other cases with nasal polyposis in the cohort of 373 patients, on which CT was accessible. The most frequent score obtained in cases with chronic rhinosinusitis allergic-infected was 8 on the left side, 7 on the right side, and in patients with nasal polyposis without chronic rhinosinusitis the most frequent value was 4 (much lower in number – 53 cases), which means that nasal polyposis appears in cases with chronic rhinosinusitis background in a large number of patients that may be insufficiently evaluated from the imaging (CT) point of view (Figure 4).
Discussion
1. The endoscopic Lildholdt scale shows that the majority of patients presented in the last stage of nasal polyposis, characterized by complete nasal obstruction. It is important to carry out this type of evaluation because only this way we can select the most effective therapeutic methods. In the international literature, the most common are patients who correspond to the 2nd and 3rd grades, according to Lildholdt staging by nasal fiberscopy, the same with the preoperative radiological staging(3). The essential explanation given for the patients with grade 3 Lildholdt (58.71% of cases) is that the standard of living, education and level of intelligence leads to a reduction in adherence to medical services and to a real reluctance to medical advice, leading to delayed diagnosis and treatment of nasal polyposis often in advanced stages.
2. The Lund-Kennedy scale was used both preoperatively and postoperatively on endoscopic evaluation to objectify the initial endonasal situation, but also to dynamically observe the postsurgical effects on both nostrils. As a result, the polyps were observed bilaterally, and their benign nature was confirmed at their 1-month postoperative follow-up in all analyzed cases. However, a unilateral nasal polyp should always be suspected of malignancy until proven otherwise, especially in elderly patients with a history of exposure to sawdust(4).
3. The Lund-Mackay grading system by imaging methods (CT) categorically establishes the approach in any case by choosing the best surgical techniques in order to cover all affected territories to obtain the best postsurgical results. This study proved, as well as similar published studies, that a high Lund-Mackey CT score correlates with a high preoperative SNOT-22 score and with very good postoperative results, with a significant improvement in the quality of life(5), meaning a significant decrease in postoperative symptomatology.
4. The Lund-Mackay score increased as the degree of nasal polyposis increased(6). The Lund-Mackay score is widely used for the assessment of chronic rhinosinusitis(6).
5. Despite the initially published success rate, approximately 10-15% of patients with nasal polyposis will require reinterventions(7).
6. Chronic rhinosinusitis with nasal polyposis is a nasal pathology with a high tendency of recurrence(8).
7. The Lund-Mackay score measures a different aspect of the disease from the subjective symptom scores(6).
Conclusions
1. Even though the scores of Lund-Kennedy, Lund-Mackay and the Lildholdt grading system are validated in the international literature, none of them can predict the evolution of nasal polyposis or anticipate the recurrences. Their usefulness has been demonstrated by diagnosing and tracking cases from a subjective and objective point of view.
2. The essential role of endoscopic and imaging methods is establishing the most effective therapeutic algorithm according to the interpretation of information provided in each individual case.
3. By analyzing these methods we can interpret the severity of nasal polyposis, respectively the postoperative effects.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
-
Johansson L, Akerlund A, Holmberg K, Melén I, Stierna P, Bende M. Evaluation of methods for endoscopic staging of nasal polyposis. Acta Otolaryngol. 2000; 120:72–76.
-
Seethala RR, Pant H. Pathology of nasal polyps. In: Önerci TM, Ferguson BJ (Eds): Nasal polyposis. Springer. 2010; Heidelberg, 105.
-
Cabrera-Ramírez MS, Domínguez-Sosa MS, Borkoski-Barreiro SA, Falcón-González JC, Ramos-Macías Á. Análisis y resultados de la cirugía endoscópica nasosinusal en rinosinusitis crónica con pólipos. Acta Otorrinolaringológica Española. 2017; 68(2), 80–85.
-
Ta NH. Will we ever cure nasal polyps? The Annals of The Royal College of Surgeons of England. 2019 Jan; 101(1): 35–39.
-
Brooks SG, Trope M, Blasetti M, Doghramji L, Parasher A, Glicksman JT, Kennedy DW, Thaler ER, Cohen NA, Palmer JN, Adappa ND. Preoperative Lund-Mackay computed tomography score is associated with preoperative symptom severity and predicts quality-of-life outcome trajectories after sinus surgery. International Forum of Allergy and Rhinology. 2018 Jun; 8(6): 668–675.
-
Hopkins C, Browne JP, Slack R, Lund V, Brown P. The Lund-Mackay staging system for chronic rhinosinusitis: How is it used and what does it predict? Otolaryngology - Head and Neck Surgery. 2007; 137(4), 555–561.
-
Baban MIA, Mirza B, Castelnuovo P. Radiological and endoscopic findings in patients undergoing revision endoscopic sinus surgery. Surg Radiol Anat. 2020; 44(2):s00276-020-02427-5.
-
Meng Y, Zhang L, Lou H, Wang C. Predictive value of computed tomography in the recurrence of chronic rhinosinusitis with nasal polyps. International Forum of Allergy & Rhinology. 2019 Nov; 9(11):1236-1243.

Forum ORL.ro abstracts
Madjid Samii
...
Tulburările de limbaj oral şi scris/citit – abordare holistică
Carolina Bodea Haţegan, Dorina Talaş
Lucrarea abordează problematica tulburărilor de limbaj oral şi scris/citit, având în prim-plan descrierea unui studiu de caz. Sunt prezentate tulburările de limbaj citit/scris după modelul structuralist-integrat, din p...
Metode de evaluare a vocii în fonochirurgie
Silviu Crăc, Alexandra Gheorghe, Tudor Ionescu, Loredana Ghiuzan, Cristian Ioniţă, Vlad Andrei Budu
În societatea modernă se constată o creştere a necesităţii comunicării verbale la multe categorii profesionale, în care vocea trebuie să fie clară, estetică şi adecvat de puternică. Se estimează că o voce corespun...
Consideraţii clinice şi terapeutice în sindromul Woakes
Mihai Tușaliu, Iulia Tiţă, Diana Tuas, Ruxandra Ranete, Cristina-Maria Goanţă
Sindromul Woakes este o afecţiune rară, fiind definit ca o polipoză nazală recurentă severă, care, prin presiunea continuă exercitată de inflamaţia cronică şi de creşterea extensivă a polipilor nazali în cavitatea...
Papilom inversat malignizat cu origine sfenoidală – management terapeutic
Mihai Tușaliu, Iulia Tiţă, Andreea Ghioca
Papilomul inversat este o formă de tumoră benignă nazosinusală, având drept caracteristici evoluţia locală agresivă, tendinţa la recidivă şi un risc important de transformare malignă. Originea tumorii este, în cel...