Sindrom Lyell - consideraţii pe baza unui caz clinic
Lyell syndrome – considerations upon a clinical case
Abstract
Lyell syndrome – or toxic epidermal necrolysis – is a severe mucocutaneous reaction caused by the administration of a drug, and is characterized by extended lesions and systemic impairment. Cytokinic storm leads to multiorgan impairment and to metabolic disturbancies, which sometimes can determine the prognosis. There is no specific treatment and the evolution can be unpredictable. The authors present the case of a young girl with Lyell syndrome after the administration of neurologic medication.Keywords
Lyell syndrometoxic epidermal necrosischildRezumat
Sindromul Lyell – sau necroliza epidermică toxică – este o reacţie mucocutanată severă cauzată de administrarea unui medicament şi se caracterizează prin leziuni extinse şi atingere sistemică. Furtuna citokinică duce la afectarea mai multor organe şi la tulburări metabolice, care uneori pot determina prognosticul. Nu există un tratament specific, iar evoluţia poate fi imprevizibilă. Autorii prezintă cazul unei fetiţe diagnosticate cu sindrom Lyell după administrarea de medicaţie neurologică.Cuvinte Cheie
sindrom Lyellnecroză epidermică toxicăcopilLyell syndrome – or toxic epidermal necrolysis – is a severe mucocutaneous reaction caused by the administration of a drug, and is characterized by a rash of the epidermis that fuses rapidly and turns into a large dark erythema, with intense necrosis and scaling of the epidermis in the cloth, similar to skin lesions caused by burns. It is invariably accompanied by constitutional symptoms and systemic impairment(1,2,3,6).
Toxic epidermal necrolysis (TEN; Lyell syndrome) was first described in 1956 by dr. Alan Lyell in Scotland. He described four patients who “looked as though they had been scalded, but there was no history of any burn”. Lyell described this as an “exanthematic eruption followed by generalized exfoliation” and believed that it was caused by an unidentified toxin, causing necrosis and epidermolysis. Before this, similar exanthematous eruptions with blistering had not been specifically classified. It became apparent to Lyell that the original four cases represented different pathologic processes. He thereafter discussed the involvement of an yet unidentified staphylogenic toxin.
The term TEN was subclassified temporarily into staphylogenic TEN and drug-induced TEN. In the following years, Lyell along with the microbiologist John Arbuthnott unsuccessfully sought evidence of a staphylococcal toxin targeted at the epidermis using adult mouse skin. This serendipitous use of baby mice allowed the successful isolation of the toxin and demonstrated the pathogenesis of staphylococcal scalded skin syndrome (SSSS). Lyell wrote: “As a result of Melish and Glasgow’s work, the staphylococcal scalded skin syndrome had been born and John and I had been beaten to the post”. As time passed, more cases of TEN were reported in association with drugs, and TEN, SSSS and erythema multiforme were all described and classified according to cause and level of epidermal split. TEN is now considered as part of a spectrum with Stevens-Johnson syndrome (SJS). Anticonvulsants, sulfur drugs, nonsteroidal anti-inflammatory drugs and antibiotics are often involved. Although rare, the average mortality rate is about 30%, but can be higher depending on the patient’s age and the extent of epidermal loss. Alan Lyell worked in Glasgow Royal Infirmary from 1959 until retirement, in 1980. He foresaw a united Glasgow wide service and training rotation, which was realized in 2006 and was named in his honor.
Identifying and annihilating the offending agent can result in self-limiting illness. Toxic epidermal necrolysis is similar to Stevens-Johnson syndrome, but in this case the affected body area is smaller.
Chan et al. proposed in 1990 other criteria to define the clinical features and the differences between SJS and TEN, and recommend that SJS should be defined by five parameters: (i) involvement of at least two mucous membranes; (ii) the presence of target lesions; (iii) fever; (iv) skin biopsy compatible with erythema multiforme; (v) skin loss <20% of the total body surface area (TBSA). Toxic epidermal necrolysis was defined on the basis of the following: (i) involvement of at least two mucous membranes; (ii) loss of confluent sheets of epidermis, leaving an exposed dermis; (iii) fever; (iv) erosions of at least 20% of TBSA; (v) skin biopsy compatible with TEN(7).
Thus, according to the Bastuji-Garin clinical classification, when is affected less than 10% of the body surface, we speak of Stevens-Johnson syndrome; Stevens-Johnson/Lyell syndrome overlap syndrome is defined when the damage is between 10% and 30%; and in cases in which the condition exceeds 30% of the body surface, we define the Lyell syndrome or toxic epidermal necrolysis(4).
Drugs such as sulfonamides, anticonvulsivants (phenobarbital, phenytoin, carbamazepines), nonsteroidal anti-inflammatory drugs, antimalarials (chloroquine), antiretrovirals (nevirapine, protease inhibitors), antibiotics (cephalosporins, aminopenicillins, tetracycline, quinolones, imidazoles, antifungals) and allopurinol are supposed to have a role in triggering this disease. The confirmation of the precise drug that caused toxic epidermal necrosis is often difficult due to the simultaneous consumption of several drugs by the patient(1,2,6).
The pathogenesis is represented by extensive keratinocyte apoptosis. A drug-induced hypersensitivity reaction initially occurs, in which a major role is played by cytotoxic CD8+ T lymphocytes, suggesting that a major restrictive MHC class I histocompatibility complex will cause clonal expansion of cytotoxic CD8+ T lymphocytes, proving that they have a cytotoxic activity on keratinocytes. This cytotoxicity is mediated by granzyme B. The most important cytotoxic molecules responsible for disseminated keratinocyte apoptosis in Lyell syndrome are the molecules Fas-FasL, granulizine and TNF alpha(5,6).
Histologically, a dermoepidermal detachment occurs with confluent necrosis of keratinocytes. In the dermis, a scattered lymphocyte infiltration is commonly evidenced. Skin lesions may predominate in sun-exposed areas, and often begin symmetrically on the trunk, the proximal upper extremities and on the face, spreading to the neck. The legs and the distal part of the arms are relatively spared, except for palms and soles. Mucosal surface involvement is frequent and can include mouth and genital areas. A mucositis can also occur some days before skin lesions. Ocular regions are not spared and acute findings can show purulent conjunctivitis with resulting pseudomembrane formation. An important mucosal area involved in Lyell’s disease is the respiratory tract, with up to 30% of cases with bronchial epithelium sloughing and hypoxaemia. The gastrointestinal tract can be involved, with rectal bleeding and sloughing of intestinal mucosa, but also liver function exams abnormalities can occur, even though the etiopathology is still unknown. Septicaemia is the most frequent cause of death in patients with TEN and is usually due to Staphylococcus aureus or to Pseudomonas(9).
The differential diagnosis should be made with erythema multiforme, impetigo, systemic lupus erythematosus, linear IgA dermatosis, staphylococcal scalded skin syndrome (SSSS), pemphigus vulgaris, bullous pemphigoid, graft versus host disease and with thermal or chemical burns.
The complications that may occur are hypo-/hyperpigmentation of the affected skin, ophthalmic complications (entropion, ectropion, corneal opacity, synechiae), infectious complications or systemic complications, including esophageal, urethral, vaginal, bronchial and anal strictures(1,2,6).
Case presentation
We present the case of an 8-year-old female patient from the rural area, who at first went to the Botoşani County Clinical Hospital accusing a sudden onset of high fever (40°C), followed at 48 hours by an urticarial rash on the trunk and limbs, being diagnosed with drug erythroderma. The patient was discharged on parents’ request and then hospitalized at the Suceava County Clinical Hospital with prolonged febrile syndrome and observation of Kawasaki disease. She was transferred to the Second Pediatric Clinic of the “Sf. Maria” Emergency Clinical Hospital for Children, Iaşi, with prolonged febrile syndrome and erythematous plaques with generalized maculopapular elements, periorbital and limb edema, erosion of the oral and labial mucosa, apparently started three weeks after the initiation of lamotrigine therapy (for the treatment of myoclonic seizures).
From the hereditary antecedents, we retain that the mother, the father and the brother are apparently healthy and deny the contact with people with infectious-contagious diseases or tuberculosis.
The personal pathological history reveals a seizure in July 2018 and epilepsy with myoclonic absences in February 2019.
The background medication administered prior to hospitalization was represented by Depakine® and lamotrigine (discontinued at the Botoşani Clinical Hospital five days before the transfer to the clinic). At the Botoşani Clinical Hospital, she was treated with Isoprinosine®, gluconic calcium, vitamin C and corticotherapy, with an unfavorable evolution. During the hospitalization in the Suceava Clinical Hospital, antibiotic treatment, corticosteroid, antihistamine, Isoprinosine®, calcium gluconic and rehydration, with stationary evolution, were administered.
The clinical examination performed at hospitalization revealed a serious general condition, with a state of consciousness, height 145 cm, weight 82 kg, BMI 39 kg/m2, thus evidencing obesity. Skin presented with erythematous plaques with generalized maculopapular elements, periorbital edema and in the upper and lower limbs; erosions in the oral and labial mucosa. The respiratory system showed a normally conformed thorax, symmetrical costal excursions, physiological vesicular murmur, respiratory rate 22/min, and peripheral O2 saturation of 98%. The cardiovascular system showed apexian shock in the 5th left intercostal space on the medioclavicular line, rhythmic heart sounds, pulsating peripheral arteries, heart rate 102/min, and BP 88/61 mmHg. The digestive system showed a supple, depressed abdomen, mobile with respiratory movements, painless spontaneously or on superficial and deep palpation, with physiological intestinal transit.
Biologically, we detected the following: monocytosis, inflammatory syndrome present, hepatocytolysis syndrome, mild hypoproteinemia with hypoalbuminemia and hyperalphaglobulinemia, selective immune deficiency of IgG, conjunctival secretion (direct microscopic examination – rare destroyed cells, Staphylococcus-negative culture).


At 24 hours after hospitalization, the patient had an epileptic seizure with loss of consciousness, generalized cyanosis and clonias, therefore she was transferred to the intensive care unit. Later, after 72 hours, she was transferred to the 2nd Pediatric Clinic for monitoring and treatment.
Chest X-ray revealed discrete infiltrative appearance of the bilateral perihilar and hilio-basal interstitium, normal radiological heart, and clear costodiaphragmatic sinuses.
EKG showed physiological respiratory arrhythmia. Echocardiography revealed normal structural and functional heart, without fluid in the pericardium, and coronaries with normal caliber.
The ophthalmological consultation revealed blepharoconjunctivitis which improved under topical treatment.
Dermatological and plastic surgery consultation reviews for post-drug Lyell syndrome.
The neurological consultation reveals the diagnosis of myoclonic absence epilepsy. The genetic counseling recommends endocrinological monitoring (FT4, TSH – normal) and age-appropriate nutrition.
During the hospitalization, she received antibiotic treatment (ceftriaxone), intraocular topic, two administrations of gamma globulin, antihistamines and hepatoprotectives, the evolution being favorable.
The patient was discharged and it was recommended to avoid self-medication. The administration of lamotrigine was forbidden, being recommended age-appropriate diet (hypocaloric, hypoglycemic, hypolipidemic), treatment with levetiracetam 1 g/day in two doses, local applications with Dermatrofin® after washing the skin with Dermobacter®, and reevaluation.
The case is an exemplification of a rare disease – Lyell syndrome, which is generally rare, but it can have a severe evolution. At the same time, the differential diagnosis is important, because in this case the suspicion of Kawasaki disease or of allergies of different etiologies was taken into discussion.
Bibliografie
-
Dowd PM, Champion RH. Toxic epidermal necrolysis. In: Champion RH, Burton JL, Burns DA, et al., editors. Text book of dermatology, Vol 2, 6th ed. London: Blackwell Science, 1998: 2085–7.
-
Fritsch PO, Ruiz-Maldonado R. Erythema multiforme, Stevens Johnson syndrome and toxic epidermal necrolysis. In: Fitzpatrick IM, Eisen AZ, Wolff K, editors. Dermatology in General Medicine. 2011; 543–57.
-
Adzick NS, Kum SH, Bandoc CC, Quinby WC, Remensnyder JP. Management of toxic epidermal necrolysis in a pediatric burn centre. Am J Dis Child. 1985 May;139(5):499–502.
-
Sehgal VN, Srivastava G. Toxic epidermal necrolysis (TEN) Lyell’s syndrome. The Journal of Dermatological Treatment. 2005;16(5-6):278-86.
-
Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens Johnson syndrome and EM. Arch Dermatol. 1993 Jan;129(1):92–6.
-
Harr T, French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis. 2010;5:39
-
Chan HL, Stern RS, Arndt KA, Langlois J, Jick SS, Jick H, et al. The incidence of erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis. A population-based study with particular reference to reactions caused by drugs among outpatients. Arch Dermatol. 1990 Jan;126(1):43–7.
-
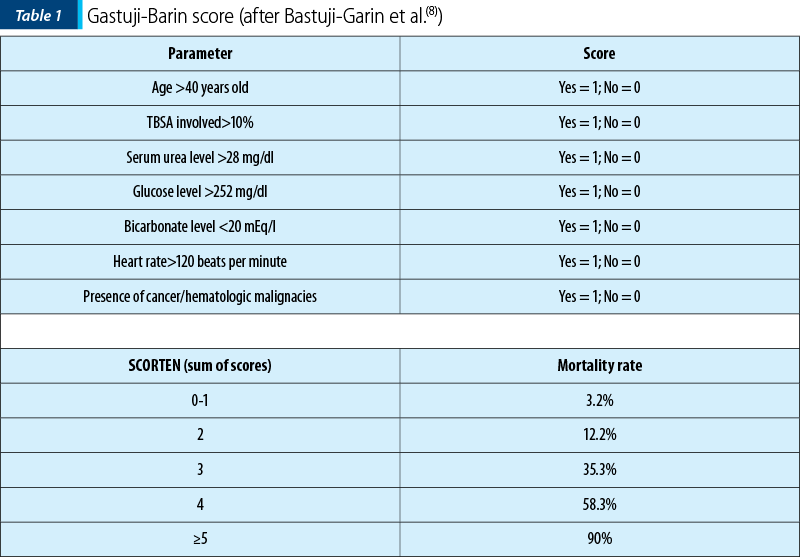
Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P, et al. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 2000 Aug;115(2):149–53.
-
Atiyeh BS, Dham R, Yassin MF, El-Musa KA. Treatment of toxic epidermal necrolysis with moisture-retentive ointment: a case report and review of the literature. Dermatol Surg. 2003 Feb;29(2):185–8.

Capcane de diagnostic în patologia pulmonară malformativă la copil
Alina Murgu, Bianca Bendoiu, Gianina Darie, Ionela Dobre, Flavia Hoşleag, Ioana Cernescu, Doina Nedelcu, Bogdan A. Stana
Bronchogenic cyst belongs to congenital non-vascular lung malformations....
Trisomia 18 – cauză rară de malformaţie cardiacă complexă
Mirela Silvia Iancu, Daniela Popeia, Varvara Toma, Ana Maria Daviţoiu, Victoria Hurduc, Doina Anca Pleşca
Trisomy 18 (Edwards syndrome), a rare genetic condition, recognized since 1960, is the second most common autosomal trisomy, after trisomy 21....
Deficitul de alfa-1 antitripsină – discuţie pe marginea unui caz cu genotip Pi*SZ
Daniela Pop, Dorin Farcău
Alpha-1 antitrypsin deficiency is a hereditary disorder, characterized by a low serum level or alpha-1 antitrypsin function....
Capcane de diagnostic în patologia pulmonară malformativă la copil
Alina Murgu, Bianca Bendoiu, Gianina Darie, Ionela Dobre, Flavia Hoşleag, Ioana Cernescu, Doina Nedelcu, Bogdan A. Stana
Bronchogenic cyst belongs to congenital non-vascular lung malformations....
Trisomia 18 – cauză rară de malformaţie cardiacă complexă
Mirela Silvia Iancu, Daniela Popeia, Varvara Toma, Ana Maria Daviţoiu, Victoria Hurduc, Doina Anca Pleşca
Trisomy 18 (Edwards syndrome), a rare genetic condition, recognized since 1960, is the second most common autosomal trisomy, after trisomy 21....