Îmbunătăţirea abilităţilor somatopsihice şi cognitive într-un caz postaccident vascular cerebral tratat cu factori neurotrofici
Improvement of somatopsychic and cognitive abilities in a post-stroke patient treated with neurotrophic factors
Abstract
We analyze the case of a patient with a long history of affective disorder who did not receive the proper treatment in the last two years, post-stroke. The patient manifests cognitive decline, behavioural changes, numerous somatizations and elements of negative hyperthymia. The evaluation took place in inpatient care by using psychometric instruments alongside daily clinical and paraclinical observation in order to fully evaluate both his initial status and his post-treatment status. Through neuroregenerative and neuroprotective mechanisms, Cerebrolysin® and other neurotrophics prove their clinical benefits in neurocognitive disorders.Keywords
neurotrophic factorspost-strokecognitive declinenegative hyperthymiaCerebrolysinRezumat
Prezentăm cazul unui pacient cu istoric lung de tulburare afectivă, neglijată terapeutic în ultimii doi ani, care, secundar unui accident vascular cerebral, manifestă clinic o patologie polimorfă cu elemente deteriorative cognitive, alterări de comportament şi acuze somatice cu elemente afective de hipertimie negativă. Evaluarea s-a realizat în dinamică, folosind instrumente psihometrice, alături de monitorizarea clinico-paraclinică atât pentru aprecierea statusului iniţial, cât şi a ameliorării simptomatologiei sub tratament. Prin mecanismele neuroregenerative şi neuroprotective, Cerebrolysin® şi alte substanţe cu rol neurotrofic îşi dovedesc eficacitatea clinică în tulburările neurocognitive.Cuvinte Cheie
factori neurotroficiaccident vascular cerebraldeteriorare cognitivăhipertimie negativăCerebrolysinIntroduction
Mood disorders along with cognitive decline are frequents symptoms in stroke survivors. These symptoms are worrying for both patients and their carers, with a negative influence on the patient’s quality of life.
In our case, we used the neurotrophic drug Cerebrolysin®, which is composed of low-molecular-weight peptides and amino acids, with proven neuroprotective and neuroplastic benefits. It has been reported that Cerebrolysin® promotes the recovery of motor functions in central nervous system disorders.
Patient’s description
Male, 72 years old.
Retired at the age of 65 years old.
He is married, living with his wife and their two daughters.
Reasons for hospital admission
Depressive mood, easy crying, hypomnesia, hypoprosexia, generalised anxiety, anhedonia, hypobulia, insomnia, multiple somatizations (pain, paresthesia).
Family’s description (wife)
“Now you see him sad, but he’s not always like that.”
“He has mood swings.”
“When I speak to him, he often seems absent.”
“He often forgets and cannot carry out the housework as he used to do. He forgets our relatives’ names and when he gets out of the house, he doesn’t recognize his acquaintances. When I remind him about them, he apologizes quickly and seems to wake up somehow, but he looks worried and realizes that something is wrong.”
“He sometimes behaves like a child, he cries, he gets upset quickly and he can become verbally aggressive.”
“I know how he used to be when he was depressive, but now he’s different.”
“I barely convinced him to come to the hospital.”
Disease history
Personal psychiatric antecedents:
Multiple hospitalizations in the last 10 years for depresive mood disorder.
There weren’t noticed psychotic elements at the moment of examination.
The patient was administered multiple antidepressant treatments, with or without mood stabilizers and anxiolytic drugs.
The evolution was mostly favorable, but with multiple relapses due to partial treatment adherence.
The last hospital admission was two years ago.
At the beginning, the cognitive decline was insidiuous, but due to the stroke, the patient has presented significant deteriorations in the last six months.
Personal pathological antecedents: essential arterial hypertension, dyslipidemia, stroke six months before the examination.
Heredocolateral antecedents: mother with cardiovascular pathology.
The patient doesn’t smoke and doesn’t use psychostimulant substances.
Mental state examination
General aspect: appropriate clothing for his age and status, maintained hygiene, hypermobile gestures.
The patient looks sad and anxious.
The psychic contact is easily established and maintained.
The patients is slightly temporally disoriented, but spatially oriented. We notice difficulties in concentration and in performing mathematical calculations. He initially makes mistakes, but he usually rectifies them.
Memory: evocation hypomnesia with the lack of ability to recall recent events. He frequently forgets names and sometimes he lacks of ability to recall familiar persons.
Thinking: slow, poor vocabulary taking into consideration his educational level.
Aphasia.
Dysarthria.
Moderate difficulty in planning, organizing and the management of daily activities.
The patient presents depressive ideation, including thoughts of worthlessness, incurability and hypochondria.
Mood state: emotional lability.
Anhedonia.
Generalized anxiety, with a moderate decrease in mood spectrum.
Lack of interest regarding the surrounding world.
The patient also presents a lower self-esteem.
Modified circadian rhythm, with difficulties in falling asleep and awakening anxiety at 3:00 o’clock in the morning; superficial, unrefreshing sleep.
Loss of appetite.
Multiple somatizations: headaches, paraesthesia, cenesthopathy.
The disease insight is only partially present.
Clinical examination
Post-stroke sequelae, clinically manifested by concentration difficulties, along with attention and memory impairment.
Slighty diminished reflexes on the right side of the body.
Decreased sensitivity on the right side of the body.
Scarring lesions resulted from stroke.
Mixed aphasia, motor predominant.
Paraclinical examinations
Computed tomography: old hypodensities after left lateral periventricular stroke. Fluid spaces are mostly symmetrical, with a small increase on the left side compared to the right one. Leukoaraiosis on both sides, near the ventricles. Early cerebral atrophy.
Electroencephalogram: moderate bioelectrical modifications which suggest vascular lesions. A slow theta polymorphic activity is noticed. The irritating isolated modifications are also noticed in the form of short grouped polymorphic waves. There are noticed a decreased amplitude, inconstant alpha rhythm and barely represented.
ECG: sinusal rhythm.
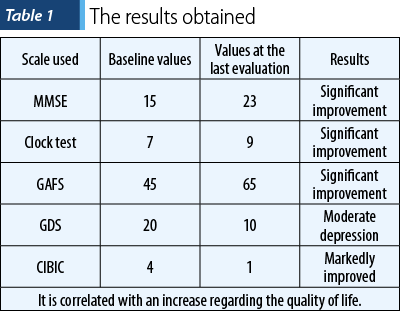
MMSE test: 18/30.
Clock drawing test: 7/10.
Reisberg Scale: 4/7.
GDS: 20 (major depression).
CIBIC: 4/7 (moderate).
SF-12: 24.
Positive diagnosis
Axis I: mixed dementia, recurrent depressive disorder, severe depressive episode without psychotic elements.
Axis II: without disharmonic personality traits.
Axis III: essential arterial hypertention, dislipidemia, stroke.
Axis IV: Without psychosocial problems
Axis V: GAFS score – 45/100.
Objectives
Slowing down the cognitive decline.
Stabilizing the mood disorder.
Slowing down the behavioral changes.
Preventing the agitation episodes.
Maintaining a high degree of independence for the patient.
Reducing the risks and costs associated to the disease.
Preventing the need for chronic hospitalization of the patient.
Treatment plan
Neuroprotection and neuroregeneration: neurotrophic factors – Cerebrolysin® 10 ml/day for 10 days/month, 6 consecutive months, Acutil® 2 tb/day, Cebrium® 1 tb/day.
Antidepressive: selective inhibitor of serotonin and norepinephrine reuptake – duloxetine 60 mg/day.
Mood stabilizer: gabapentinum 600 mg/day.
Measures for neurological rehabilitation and psychotherapy, antihypertensive medication, lowering-cholesterol drugs, along with natural supplements.
Expected results after the treatment
An increase in his cognitive status, decreasing the cognitive decline.
The control of non-cognitive symptoms.
A high tolerability and safety of the new treatment scheme.
An increase of the patient’s quality of life.
The long-term prognosis is reserved, taking into consideration the natural evolution of the disease and the associated risk factors.
Discussion
Depression must be closely supervised and promptly treated when we are dealing with elderly patients. One of the main reasons is the fact that depression may be an early sign of dementia, at the same time increasing the risk for an acute cerebral pathology when is associated with other disorders, such as metabolic syndrome or cardiovascular disease.
The psychological symptoms may be directly correlated to the cerebral lesions, but they can also result from the development of the disability.
Without a multidisciplinary approach, the patient is at risk for aggravating the psychosomatic symptoms and for worsening his disability. In the absence of adequate measures, these modifications can become irredeemable.
Conclusions
Taking into account the socioeconomic burden, which is expected to grow even further due to the continuous increase of life expectancy and to the high proportion of elderly, it is important to prevent or reduce the complications related to stroke as soon as possible.
Although they aren’t always life-threatening, these can lead to delayed rehabilitation, long hospitalization periods, poor functional result and to an increase of health care costs.
Through its neuroregenerative and neuroprotective mechanisms, Cerebrolysin® demonstrates clinical benefits in neurocognitive disorders.
The associated psychotropic medication can be used for treating the psychosomatic symptoms and for slowing down the cognitive decline in post-stroke patients. The timely diagnosis of the cognitive symptoms associated to mood disorders requires an early complex therapeutic approach.
Bibliografie
-
Mureşanu DF, Heiss WD, Hoemberg V, Bajenaru O, Popescu CD, et al. Cerebrolysin® and recovery after stroke (CARS): A randomized, placebo-controlled, double-blind, multicenter trial. Stroke. 2016 Jan;47(1):151-9.
-
Ladurer G, Kavalch P, Moessler H, the Cerebrolysin® Study Group. Neuroprotective treatment with Cerebrolysin® in a patient with acute stroke: a randomized controlled trial. J Neural Transm (Vienna). 2005 Mar;112(3):415-428.
-
Mureşanu DF, et al. A retrospective, multi-center cohort study evaluating the severity-related effect of Cerebrolysin® treatment on clinical outcomes in traumatic brain injury. CNS Neurol Disord Drug Targets. 2015;14(5):587-99.
-
Chen CC, Wei ST, Tsaia SC, Chen XX, Cho DY. Cerebrolysin® enhances cognitive recovery of mild traumatic brain injury patients: double-blind, placebo-controlled, randomized study. British Journal of Neurosurgery. 2013 Dec; 27(6):803-7.
-
Gauthier S, Proano JV, Jia J, Froelich L, Vester JC, Doppler E. Cerebrolysin® in mild-to-moderate Alzheimer’s disease: a meta-analysis of randomized controlled clinical trials. Dementia and Geriatric Cognitive Disorders. 2015; 39(5‑6):332-47.
-
Konig P, Waanders R, Wirtzmann A, et al. Cerebrolysin® in traumatic brain injury – a pilot study of neurotrophic and neurogenic agent in the treatment of acute traumatic brain injury. J Neurol Neurochirurgie Psychiatrie. 2006;7(3):12-20.
-
Alvarez XA, et al. Positive effects of Cerebrolysin® on electroencephalogram slowing, cognition and clinical outcome in patients with postacute traumatic brain injury. Int Clin Psychopharmacology. 2003;18(5):271-278.

Virgil Enătescu şi Alexandru Dan Ilieş
...
Anxietatea – ce, cum, când şi de ce?
Andrei Buciuta
...
Retrospectiva 2020 a evenimentelor ştiinţifice în domeniul psihiatriei şi sănătăţii mintale din România
...
Eficacitatea factorilor neurotrofici în tratamentul cazurilor cu demenţă mixtă, vasculară şi Alzheimer, cu multiple comorbidităţi
Raluka Albu-Kalinovic, Mirabela Dinescu, Gabriela Vlad, Oana Neda-Stepan, Virgil Enătescu
The incidence of neurodegenerative diseases has increased as a direct result of the increasing life expectancy. .../factorii de risc pentru sanatatea mintala la lucratorii din domeniul transporturilor.webp)
Factori de risc pentru sănătatea mintală la lucrătorii din domeniul transporturilor
Roxana Stanciu, Delia Nicolai, Eva-Maria Ciobanu, Anca Buliman, Marius Iordache, Andrei Bondar, Brânduşa Ecaterina Focşeneanu, Gabriela Marian
Lucrătorii din domeniul transporturilor constituie un segment profesional expus unor solicitări fizice și psihologice cumulative, ...