Increase understanding of Palliative Care services.
State three basic focuses of Palliative Care.
Promote collaboration between primary teams and Palliative Care.
Increase understanding of varied use of Palliative Care.
Discuss varied use of palliative care: YOU DON’T HAVE TO BE DYING.
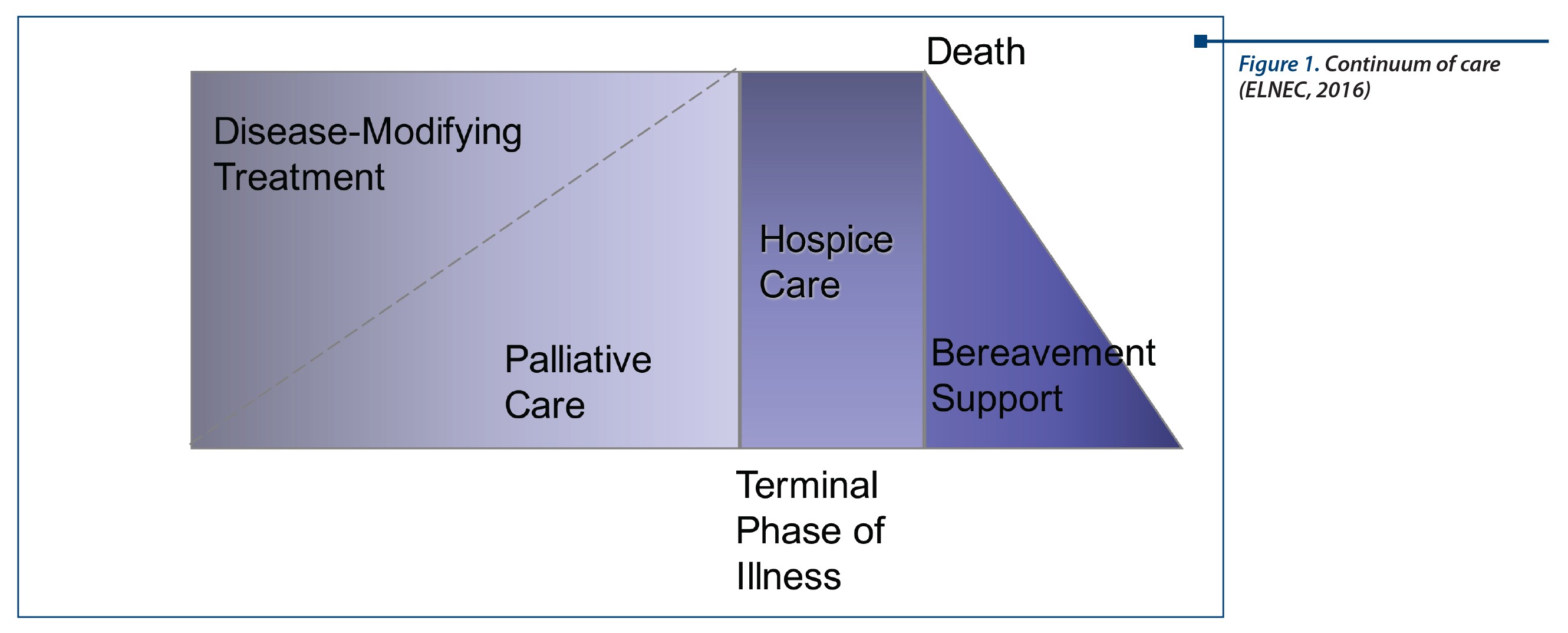
Figure 1. Continuum of care (ELNEC, 2016)
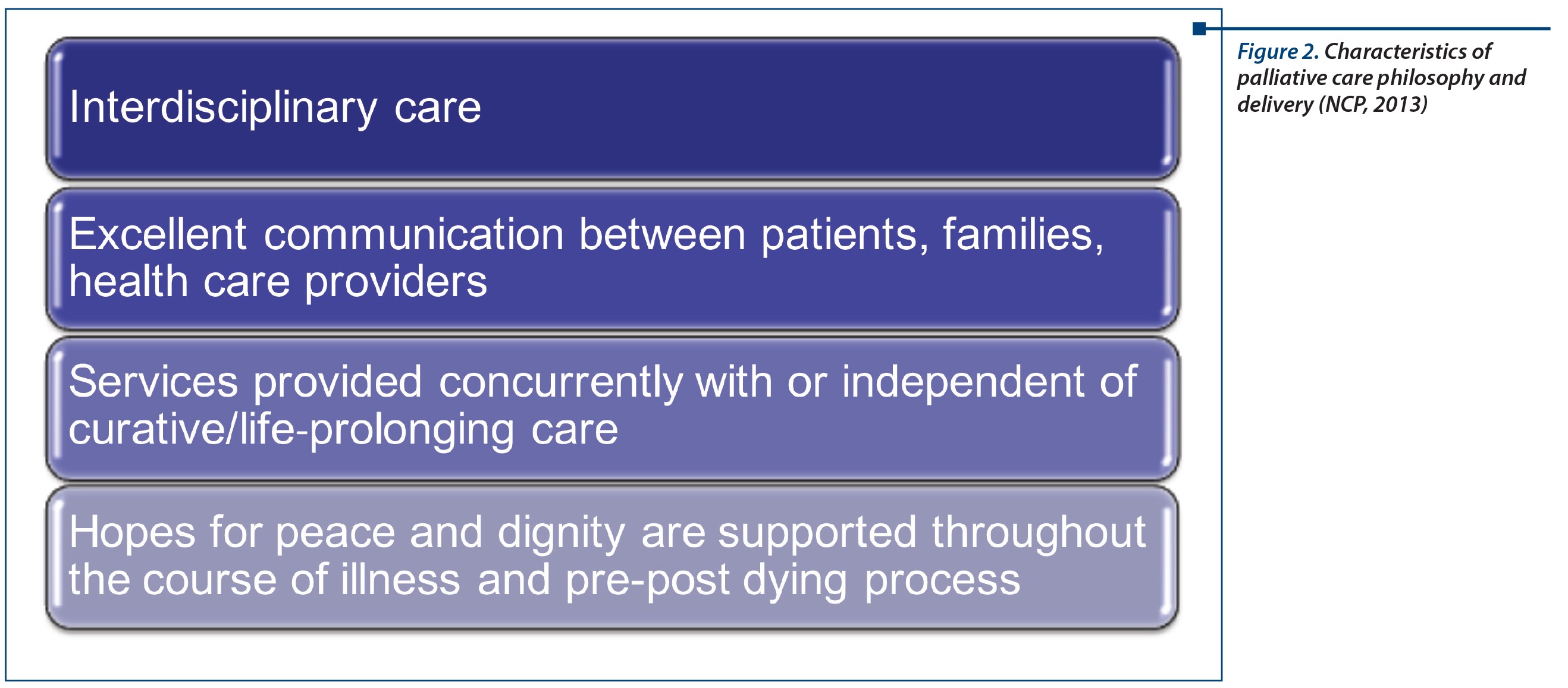
Figure 2. Characteristics of palliative care philosophy and delivery (NCP, 2013)
Figure 3. Maintaining hope
Palliative care focuses on(5):
Reliving suffering.
Achieving best possible quality of life.
Patients and family needs.
Assessment and treatment of symptoms.
Support for decision making.
Assistance with matching treatment with goals of care.
Mobilization of resources.
Collaboration with care providers.
Maintaining goals of care especially when curative treatments are no longer beneficial.
Supportive care when burdens of treatment exceed benefits.
Providing compassionate comfort care in the last months to weeks of life.
Palliative care teams(4)
Physician, social worker, nurse practitioner, dedicated chaplain, psychiatrist, nurses, pharmacist, and volunteers.
No real “team” may have one dedicated employee.
Physician or nurse practitioner only.
Set consult team brought in for GOC and EOL.
Large department with multiple rounding teams.
Large department with all essential members under one umbrella.
No palliative care team, consult hospice for in-patient care.
Common symptom management requests:
Pain management
Constipation
Nausea and vomiting
Anxiety/depression
Establishing goals of care
End of life care.
Benefits of palliative care(4):
Improved home care, leading to less ER visits.
Improved patient, family, physician satisfaction.
54% fewer hospital admissions.
80% reduction in ICU days.
26% reduction in inpatient LOS (2 days).
52% decrease in clinic visits, 60% increase in hospice enrollment.
Result: saving>$700 per member/month.
Promoting self-care(3)
Additional focus is on each other
Help to re-frame hope
Help to not view death as a failure
Acknowledge existence of professional grief
Educate on difference between a normal dying process and suffering
Staying in the present
Give up thinking you have control over how a patient’s body will respond, instead focus on what you can do to make their remaining time compassionate and comfortable
Focus on the Journey.
It’s all about the Journey
We cannot change the fact a patient will become terminally ill or die, but we have everything to say about THE JOURNEY(3).
Be pro-active and anticipate.
Request palliative care consults.
Celebrate the person - they are not their disease.
Bibliografie
1. Cotter, V.T. & Foxwell, A.M. (2015). The meaning of hope in the dying. (Ch. 5) In B. Ferrell (Ed.) HPNA Palliative Nursing Manuals: Spiritual, Religious, and Cultural Aspects of Care. New York: Oxford University Press. Pp. 91-114.
2. End of Life Nursing Education Consortium (ELNEC) (2016). Palliative nursing care. (Module 1). Core Curriculum for End of Life Nursing Education Consortium Program. Sponsored by City of Hope/AACN: Continuing Education Provider (City of Hope/Beckman Research Institute) approved by the California Board of Registered Nursing, Provider Number CEP 13380.
3. Freeman, B. (2015). Compassionate Person Centered Care of the Dying: An Evidence-Based Palliative Care Guide for Nurses. New York: Springer Publishers.
4. Hughes, M.T. & Smith, A.M. (2014). The growth pf palliative care in the United States. Annual Review of Public Health, (35), 459-75. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/24641562
5. Kelly, A.S. (2010). Palliative care - a shifting paradigm. New England Journal of Medicine, 363(8), p.781-782.
6. National Consensus Project for Palliative Care (NCP), (2013). Clinical Practice Guidelines for Quality Palliative Care (3rd ed.) Retrieved from: http://www.nationalcoalitionhpc.org/ncp-guidelines-2013/