Cât de des recomandaţi suplimentarea cu vitamină D în sarcină? Ce trebuie să ştie obstetricienii despre vitamina D şi sarcină
How often do you recommend vitamin D during pregnancy? What the obstetricians need to know about vitamin D and pregnancy
Abstract
Vitamin D (calciferol), measured by maternal serum 1,25-dihydroxyvitamin D, is important for the fetal-placental unit development. Decidua and trophoblast cells express vitamin D receptor and 1α-OHase, suggesting an autocrine or paracrine role for 1,25(OH)2D3 for fetal and placental development. During pregnancy, maternal circulating levels of 1,25(OH)2D3 double with the advancing gestation age, resulting in a concomitant increase in calcium uptake by the maternal intestine, with a concomitant decrease in calcium serum levels. In this narrative review, we want to highlight the current knowledge regarding vitamin D and pregnancy. A literature research was performed. The significant data were extracted and summarized in tables. It remains to validate whether the measurement of vitamin D levels and vitamin D supplementation (and calcium) during pregnancy should be recommended. Further studies are recommended to demonstrate any connection between the 25-OH-D level and prematurity, gestational diabetes and low birth weight, and, if present, to specify when and how vitamin D level should be dosed.Keywords
vitamin DcalciferolergocalciferolcholecalciferolpregnancyRezumat
Vitamina D (calciferolul), măsurată prin 1,25-dihidroxivitamina D în serul matern, este importantă pentru dezvoltarea unităţii fetoplacentare. Celulele deciduale şi trofoblastice exprimă receptorul vitaminei D şi 1α-OHază, sugerând un rol autocrin sau paracrin al acesteia pentru dezvoltarea fetală şi placentară. În timpul sarcinii, nivelurile circulante materne de 1,25(OH)2D3 se dublează odată cu creşterea termenului de gestaţie, rezultând o creştere concomitentă a absorbţiei calciului de către intestinul matern, cu o scădere concomitentă a nivelurilor serice de calciu. Am realizat acest review narativ pentru a evidenţia cunoştinţele actuale privind vitamina D şi sarcina. Am efectuat o căutare a articolelor relevante din literatură. Datele semnificative au fost extrase şi sintetizate în tabele. Studiul nostru abordează problema de a se verifica dacă trebuie recomandată măsurarea nivelurilor de vitamină D şi a suplimentelor cu vitamină D (şi calciu) în timpul sarcinii. Se recomandă efectuarea de studii suplimentare pentru a demonstra orice legătură între nivelul 25-OH-D şi prematuritate, diabet gestaţional şi greutatea redusă la naştere, iar dacă există, să se specifice termenul la care trebuie administrată şi doza de vitamină D.Cuvinte Cheie
vitamina DcalciferolergocalciferolcolecalciferolsarcinăVitamin D (calciferol) is a biologically inactive fat-soluble vitamin with immunomodulatory and antiproliferative characteristics. Vitamin D has two functional forms: D2 (ergocalciferol) and D3 (cholecalciferol), both prohormones. To obtain its active form, 1,25-dihydroxyvitamin D3 (1,25(OH)2D3), two successive hydroxylations, made with 1-alpha-hydroxylase (1a-OHase), are required: the first in the liver and the second in the kidneys. 1a-OHase level influences the local immune system and is present in large quantities in different tissues, including the placenta and decidual tissues, indicating the importance of 1,25(OH)2D3 production for the fetal-placental unit development. Numerous studies have demonstrated that placental synthesis of 1,25(OH)2D3 is essential in implantation, placentation and fetal growth. High levels of 1a-OHase protein and expression of 1a-OHase mRNA were found in the first-trimester and second-trimester placenta and decidua(1). Decidua and trophoblast cells express vitamin D receptor (VDR) as well as 1a-OHase, suggesting an autocrine or paracrine role for 1,25(OH)2D3 within these tissues(2). The active forms of vitamin D are of major importance in the metabolism of calcium and phosphor, which means that vitamin D receptors are expressed on almost all cells of the body(3-5). During pregnancy, maternal circulating levels of 1,25(OH)2D3 double with advancing gestation age, resulting in a concomitant increase in calcium uptake by the maternal intestine(6).
Vitamin D3 exerts an autocrine/intracrine effect and control via plasma membranes ion channels, via VDR genes located near autoimmune and cancer-associated genes over normal cellular metabolism and cellular immune function(7).
The body has been shown to make up to 25,000 IU of vitamin D3 a day in response to adequate sun exposure to UVB.
Nowadays, vitamin D deficiency has become of high interest, given the accelerated increase in its incidence. To compensate for the low intake of vitamin D from UVB radiation exposure, the general population needs to procure vitamin D from foods, which generally have a low percentage. Vitamin D deficiency is increasingly common in both the general population and pregnant women and newborns; between 18% and 84% of pregnant women suffer from vitamin D deficiency(8). Vitamin D deficiency during pregnancy can manifest in two distinct forms: (1) on the pregnant woman, which can lead to pregnancy-induced hypertension, preeclampsia(9-13), preterm birth(14,15), gestational diabetes mellitus(16), recurrent miscarriages(17); or (2) on the product of conception and the fetal appendages, which can cause: decidualization(18), defective implantation, abnormal development of the fetal skeleton, large, enlarged fountains(19), low birth weight (LBW) or small for gestational age (SGA) fetus, respiratory diseases such as asthma or bronchopulmonary dysplasia, aortic supravalvular stenosis, infections, autoimmune diseases.
It is well known that, during pregnancy, the level of 1,25-dihydroxyvitamin D3 increases to an extreme, and is particularly linked to DBP (vitamin D binding protein). Usually, the level of vitamin D is directly related to Ca, phosphates and PTH serum levels. However, during pregnancy, it has been shown that they are no longer interdependent. There is evidence that, in pregnant women, a significantly increased level of vitamin D does not lead to calcium and hypercalcemia, as it does in the general population(20).
The American Institute of Medicine (AIM) and the European Food Safety Authority (EFSA) state that the value of sufficiency blood levels of 25(OH)D is above 20 ng/mL (50 nmol/L), a similar level for pregnant and non-pregnant women(21). The Institute of Medicine and Health from Canada define the value of sufficiency blood levels of vitamin D as serum 25(OH)D)>30 nmol/L(22). Moreover, the optimal level of 25-OH-D during pregnancy is not precisely known. During pregnancy, physiological changes note an increase of 50-100% in serum concentrations of 1,25(OH)2D over the non-pregnant state during the second trimester and 100% during the third trimester(23,24). The mechanism underlying the increased serum of 1,25(OH)2D concentrations during pregnancy is not clear. Parathyroid hormone, the main stimulus for increased renal hydroxylation of 25(OH)D to 1,25(OH)2D, has not been shown to increase during pregnancy. In my practice (Dr. Anca A. Simionescu), last winter (in December), I saw, in 99% of all trimester pregnancies, a vitamin D level below 15 ng/mL, wondering if the cutoff during pregnancy shouldn’t be changed. Do we need to check the vitamin D levels of healthy pregnant women?
The Canadian Paediatric Society recommends regular vitamin D supplementation during pregnancy, ranging from 200 to 400 IU/day (5 to 10 µg/day)(25). Many vitamins, minerals and supplements in pregnancy have recently added vitamin D3.
The reported effects of vitamin D on the placenta are the following: angiogenesis(26), immune function(27), inflammation (antiinflammatory) and implantation. Immune adaptations are mandatory for the proper functioning of pregnancy, and vitamin D has a significant role in implantation through its function in the inflammation and immune process. Experiments have shown that after administering 1,25(OH)2D3 in rats, a more rapid decidualization happened, and the uterus’ mass increased significantly(18). Trophoblastic cell cultures that were created in an environment similar to that of antiphospholipid syndrome by the addition of antiphospholipid antibodies showed a reduced inflammatory response in the presence of vitamin D(28).
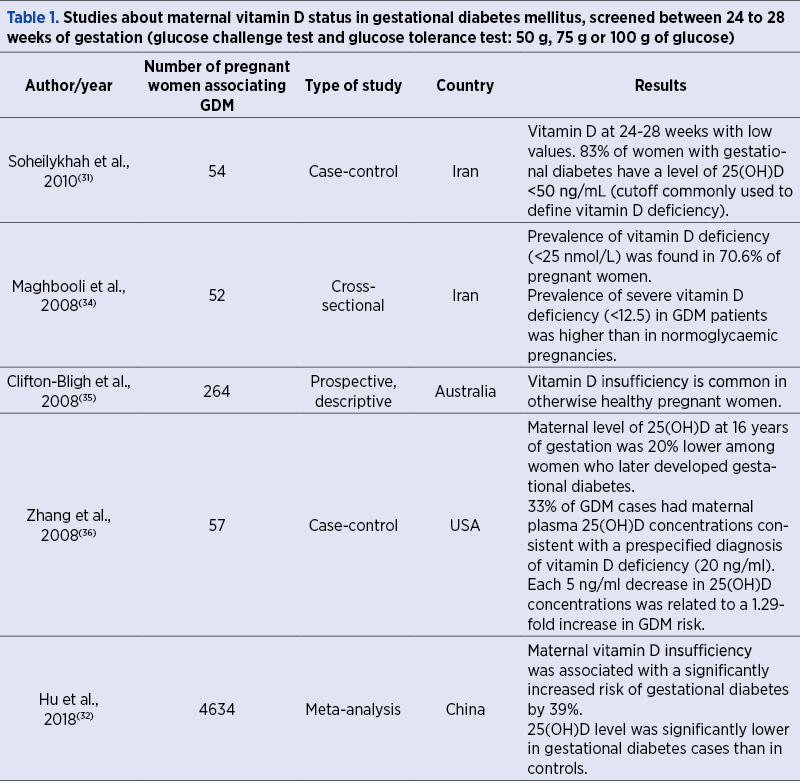
Gestational diabetes mellitus (GDM). As it was stated about 30 years ago, 1,25-dihydroxyvitamin D plays a role in regulating insulin secretion(29) and in maintaining the normal glucose homeostasis. During pregnancy, the prevalence of GDM increases simultaneously with the PTH stimulus for renal stimulation of 25-OH-D(30). Regarding the role of vitamin D deficiency in the occurrence of gestational diabetes mellitus, it has only been shown that vitamin D improves insulin sensitivity and glucose tolerance and that patients with gestational diabetes frequently experience low levels of vitamin D(31). However, it is not yet known whether taking vitamin D supplements may or may not prevent the gestational diabetes. Table 1 indicates some studies about maternal vitamin D status in diabetes mellitus, in different countries, with variable sunshine regimens. The studies demonstrate that vitamin D insufficiency is significantly associated with an increased risk of gestational diabetes(32,33).
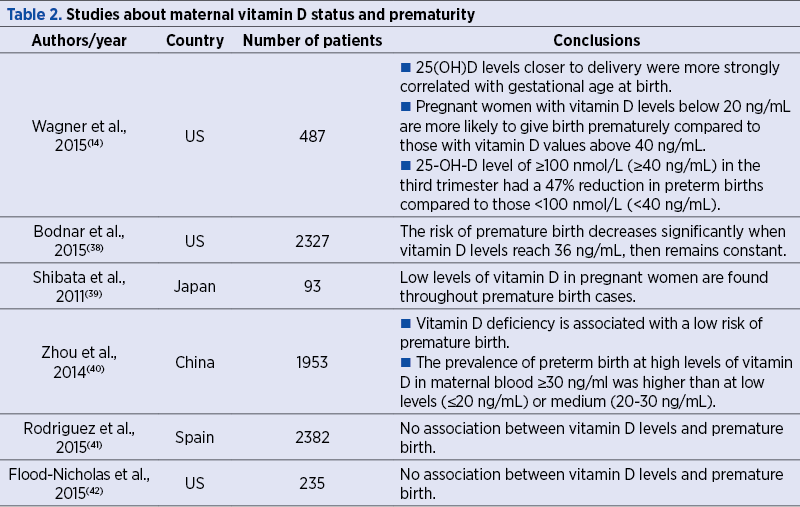
Preterm birth. While the results of the existing studies are contradictory regarding vitamin D deficiency and preterm birth or preterm birth risk, most studies conclude that there is a correlation between preterm birth and low vitamin D levels. Studies have suggested a relationship between the 25-OH-D level and the pregnancy outcome of prematurity(37); the authors have suggested a modifiable risk of prematurity through vitamin D repletion as late as the second trimester and even into the third trimester of pregnancy. The strongest association was found in twin pregnancies, where the risk of premature birth in a pregnant woman with vitamin D deficiency is stated as 60%(6).
Table 2 shows the conclusions of studies regarding the correlation between prematurity and low levels of 25-OH-D in maternal serum.
Preeclampsia. Low maternal 25-OH-D serum levels in the first trimester of pregnancy have been found in most patients developing preeclampsia. An infant born to mothers with preeclampsia has a two times higher risk of vitamin D deficiency than those born to mothers without this pathology(6,43). In these cases, the benefit to the mother, brought by the birth of the child, is weighted against the detriment of the child’s early birth and all the risks associated with premature birth.
Low birth weight (LBW) and small for gestational age (SGA). Attempts have been made to establish a relationship between LBW and SGA and vitamin D deficiency in pregnant women, but some studies have shown the opposite. Studies have shown a correlation between vitamin D treatment and the characteristics of the newborn. Khalessi et al. have found the head circumference at birth ≤33 cm associated with vitamin D deficiency, and also with LBW(44). Several studies in different populations have concluded that birth weight has not been influenced after vitamin D (and calcium) supplementation(20,45,46).
Infants level of 25-OH-D is correlated with maternal 25-OH-D level. Changes in the fetal skeleton measurements due to vitamin D deficiency may be observed around the age of 19 weeks of gestation(47). Craniotabes were associated with elevated alkaline phosphatase levels, normal PTH and with low levels of 25(OH)D. A recent systematic review and meta-analysis of randomised control trials on the effect of vitamin D supplementation on birth weight found that vitamin D supplementation alone significantly increased birth weight, but not on dose-dependent administration(48). Contradictory results were found regarding vitamin D administration and LBW or SGA babies.
The respiratory system changes are diverse, and vitamin D deficiency can lead to asthma, bronchopulmonary dysplasia (which is specific to premature infants) and respiratory infections. Bronchopulmonary dysplasia is characterized by an abnormal structure of the distal lung structures and can lead to the restriction of the development of alveoli and blood vessels that persists even after birth(49-50). In general, the interruption of physiological development occurs in the canalicular stage(51,52).
While the role of vitamin D in the normal development of the lungs has been scientifically proven(53-55), the link between vitamin D deficiency and bronchopulmonary dysplasia is still being studied. When it comes to deciding the optimal level of vitamin D for pregnant women, there are two opinions: 20 ng/ml indicated by the Institute of Medicine, while the Endocrine Society recommends around 30 ng/ml or more. These estimates were made after measuring vitamin D levels in a tribe from Africa where vitamin D levels reached 46 ng/ml and 60 ng/ml for pregnant women. After considering the different climatic conditions, Hollis et al. suggested a minimum normal value for the pregnancy rate of 40 ng/ml(20). Thus, the recommended daily doses are 4000-10,000 IU (National Institute for Health and Clinical Excellence, UK)(56).
In conclusion, it remains to validate whether the measurement of vitamin D levels and vitamin D supplementation (and calcium) during pregnancy should be recommended. Further studies are recommended to demonstrate if there is any connection between the 25-OH-D level and maternal and fetal complications, and to specify when and how vitamin D level should be dosed.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Zehnder D, Evans KN, Kilby MD, et al. The ontogeny of 25-hydroxyvitamin D(3) 1alpha-hydroxylase expression in human placenta and decidua. Am J Pathol. 2002;161(1):105-114. doi:10.1016/s0002-9440(10)64162-4.
- Diaz L, Sanchez I, Avila E, Halhali A, Vilchis F, Larrea F. Identification of a 25-hydroxyvitamin D3 1-α-hydroxylase gene transcription product in cultures of human syncytiotrophoblast. J Clin Endocrinol Metab. 2000;85:2543-2549.
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357(3):266–281. doi.org/10.1056/ NEJMra070553.
- Jones G. Pharmacokinetics of vitamin D toxicity. Am J Clin Nutr. 2008;88(2):582s–6s. doi.org/ 10.1093/ajcn/88.2.582S.
- Wierzejska R, Jarosz M, Kleminska-Nowak M, Tomaszewska M, Sawicki W, Bachanek M, et al. Maternal and Cord Blood Vitamin D Status and Anthropometric Measurements in Term Newborns at Birth. Front Endocrinol (Lausanne). 2018;9:9. doi.org/10.3389/fendo.2018.00009.
- Whitehead M, Lane G, Young O, Campbell S, Abeyasekera G, Hillyard CJ, MacIntyre I, Phang KG, Stevenson JC. Interrelations of calcium-regulating hormones during normal pregnancy. Br Med J (Clin Res Ed). 1981;283(6283):10-12.
- McCullough PJ, Lehrer DS, Amend J. Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: Insights from a seven year experience. J Steroid Biochem Mol Biol. 2019;189:228-239. doi: 10.1016/j.jsbmb.2018.12.010.
- Dawodu A, Wagner CL. Mother-child vitamin D deficiency: an international perspective. Arch Dis Child. 2007;92(9):737–740. doi:10.1136/adc.2007.122689.
- Bodnar LM, Catov JM, Simhan HN, Holick MF, Powers RW, Roberts JM. Maternal vitamin D deficiency increases the risk of preeclampsia. J Clin Endocrinol Metab. 2007 Sep;92(9):3517-3522. doi:10.1210/jc.2007-0718.
- Haugen M, Brantsaeter AL, Trogstad L, Alexander J, Roth C, Magnus P, Meltzer HM. Vitamin D supplementation and reduced risk of preeclampsia in nulliparous women. Epidemiology. 2009;20(5):720-726. doi:10.1097/EDE.0b013e3181a70f08.
- Robinson CJ, Alanis MC, Wagner CL, Hollis BW, Johnson DD. Plasma 25-hydroxyvitamin D levels in early-onset severe preeclampsia. Am J Obstet Gynecol. 2010 Oct;203(4):366.e1-6. doi:10.1016/j.ajog.2010.06.036.
- Woodham PC, Brittain JE, Baker AM, et al. Midgestation maternal serum 25-hydroxyvitamin D level and soluble fms-like tyrosine kinase 1/placental growth factor ratio as predictors of severe preeclampsia. Hypertension. 2011;58(6):1120-1125. doi:10.1161/HYPERTENSIONAHA.111.
- Robinson CJ, Wagner CL, Hollis BW, Baatz JE, Johnson DD. Maternal vitamin D and fetal growth in early-onset severe preeclampsia. Am J Obstet Gynecol. 2011 Jun;204(6):556.e1-4. doi:10.1016/j.ajog.2011.03.022.
- Wagner CL, Baggerly C, McDonnell S, Baggerly KA, French CB, Baggerly L, Hamilton SA, Hollis BW. Post-hoc analysis of vitamin D status and reduced risk of preterm birth in two vitamin D pregnancy cohorts compared with South Carolina March of Dimes 2009-2011 rates. J Steroid Biochem Mol Biol. 2016 Jan;155(Pt B):245-251. doi:10.1016/j.jsbmb.2015.10.022.
- Qin LL, Lu FG, Yang SH, Xu HL, Luo BA. Does Maternal Vitamin D Deficiency Increase the Risk of Preterm Birth: A Meta-Analysis of Observational Studies. Nutrients. 2016;8(5):301. doi:10.3390/nu8050301.
- Burris HH, Camargo CA Jr. Vitamin D and gestational diabetes mellitus. Curr Diab Rep. 2014;14(1):451. doi:10.1007/s11892-013-0451-3.
- Ota K, Dambaeva S, Han AR, Beaman K, Gilman-Sachs A, Kwak-Kim J. Vitamin D deficiency may be a risk factor for recurrent pregnancy losses by increasing cellular immunity and autoimmunity. Hum Reprod. 2014;29:208219.
- Halhali A, Acker GM, Garabedian M. 1,25-Dihydroxyvitamin D3 induces in vivo the decidualization of rat endometrial cells. J Reprod Fertil. 1991;91:59–64. doi:10.1530/jrf.0.0910059.
- Specker BL. Does vitamin D during pregnancy impact offspring growth and bone? Proc Nutr Soc. 2012;71:3845.
- Hollis BW, Johnson D, Hulsey TC, Ebeling M, Wagner CL. Vitamin D supplementation during pregnancy: Double-blind, randomized clinical trial of safety and effectiveness. J Bone Miner Res. 2011;26:2341257.
- EFSA panel on dietetic products, nutrition and allergies (NDA). Dietary reference values for vitamin D. EFSA J. 2016;14:e04547. doi:10.2903/j.efsa.2016.4547.
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al., editors. Dietary Reference Intakes for Calcium and Vitamin D. Washington (DC): National Academies Press (US); 2011. Available at: https://www.ncbi.nlm.nih.gov/books/NBK56070/ doi: 10.17226.
- Cross NA, Hillman LS, Allen SH, Krause GF, Vieira NE. Calcium homeostasis and bone metabolism during pregnancy, lactation, and postweaning: a longitudinal study. Am J Clin Nutr. 1995;61:514–523.
- Ritchie LD, Fung EB, Halloran BP, et al. A longitudinal study of calcium homeostasis during human pregnancy and lactation and after resumption of menses. Am J Clin Nutr. 1998;67:693–701.
- Canadian Paediatric Society First Nations, Inuit and Métis Health Committee. Vitamin D supplementation: recommendations for Canadian mothers and infants. Paediatr Child Health. 2007;12(7):583–598.
- Samuel S, Sitrin MD. Vitamin D’s role in cell proliferation and differentiation. Nutr Rev. 2008 Oct;66(10 Suppl 2):S116-124. doi:10.1111/j.1753-4887.2008.00094.x.
- Prietl B, Treiber G, Pieber TR, Amrein K. Vitamin D and immune function. Nutrients. 2013;5(7):2502-21. doi:10.3390/nu5072502.
- Gysler SM, Mulla MJ, Stuhlman M, Sfakianaki AK, Paidas MJ, Stanwood NL, Gariepy A, Brosens JJ, Chamley LW, Abrahams VM. Vitamin D reverses aPL-induced inflammation and LMWH-induced sFlt-1 release by human trophoblast. Am J Reprod Immunol. 2015 Mar;73(3):242-50. doi:10.1111/aji.12301.
- Johnson JA, Grande JP, Roche PC, Kumar R. Immunohistochemical localization of the 1,25(OH)2 D3 receptor and calbindin D28k in human and rat pancreas. Am J Physiol. 1994;267(3):E356-E360.
- Kramer CK, Swaminathan B, Hanley AJ, Connelly PW, Sermer M, Zinman B, Retnakaran R. Vitamin D and parathyroid hormone status in pregnancy: Effect on insulin sensitivity, beta-cell function, and gestational diabetes mellitus. J Clin Endocrinol Metab. 2014;99:4506–4513. doi:10.1210/jc.2014-2341.
- Soheilykhah S, Mojibian M, Rashidi M, et al. Maternal vitamin D status in gestational diabetes mellitus. Nutr Clin Pract. 2010;25:524–527.
- Hu L, Zhang Y, Wang X, You L, Xu P, Cui X, Zhu L, Ji C, Guo X, Wen J. Maternal Vitamin D Status and Risk of Gestational Diabetes: a Meta-Analysis. Cell Physiol Biochem. 2018;45(1):291-300. doi:10.1159/000486810.
- Wei SQ. Vitamin D and pregnancy outcomes. Curr Opin Obstet Gynecol. 2014 Dec;26(6):438-47. doi:10.1097/GCO.0000000000000117.
- Maghbooli Z, Hossein-Nezhad A, Karimi F, Shafaei AR, Larijani B. Correlation between vitamin D3 deficiency and insulin resistance in pregnancy. Diabetes Metab Res Rev. 2008;24(1):27-32. doi:10.1002/dmrr.737.
- Clifton-Bligh RJ, McElduff P, McElduff A. Maternal vitamin D deficiency, ethnicity and gestational diabetes. Diabet Med. 2008;25(6):678-84. doi:10.1111/j.1464-5491.2008.02422.x.
- Zhang C, Qiu C, Hu FB, et al. Maternal plasma 25-hydroxyvitamin D concentrations and the risk for gestational diabetes mellitus. PLoS One. 2008;3:e3753.
- Bodnar LM, Klebanoff MA, Gernand AD, Platt RW, Parks WT, Catov JM, Simhan HN. Maternal vitamin D status and spontaneous preterm birth by placental histology in the US Collaborative Perinatal Project. Am J Epidemiol. 2014;179(2):168–176. doi:10.1093/aje/kwt237.
- Bodnar LM, Platt RW, Simhan HN. Early-pregnancy vitamin D deficiency and risk of preterm birth subtypes. Obstet Gynecol. 2015 ;125(2):439-447. doi:10.1097/AOG.0000000000000621.
- Shibata M, Suzuki A, Sekiya T, Sekiguchi S, Asano S, Udagawa Y, Itoh M. High prevalence of hypovitaminosis D in pregnant Japanese women with threatened premature delivery. J Bone Miner Metab. 2011;29(5):615-620. doi:10.1007/s00774-011-0264-x.
- Zhou J, Su L, Liu M, Liu Y, Cao X, Wang Z, Xiao H. Associations between 25-hydroxyvitamin D levels and pregnancy outcomes: a prospective observational study in southern China. Eur J Clin Nutr. 2014 Aug;68(8):925-30. doi:10.1038/ejcn.2014.99.
- Rodriguez A, García-Esteban R, Basterretxea M, Lertxundi A, Rodríguez-Bernal C, Iñiguez C, Rodriguez-Dehli C, Tardón A, Espada M, Sunyer J, Morales E. Associations of maternal circulating 25-hydroxyvitamin D3 concentration with pregnancy and birth outcomes. BJOG. 2015;122(12):1695-1704. doi:10.1111/1471-0528.13074.
- Flood-Nichols SK, Tinnemore D, Huang RR, Napolitano PG, Ippolito DL. Vitamin D Deficiency in Early Pregnancy. PLoS One. 2015;10(4): e0123763. doi.org/10.1371/journal.pone.0123763.
- Achkar M, Dodds L, Giguère Y, Forest JC, Armson BA, Woolcott C, Agellon S, Spencer A, Weiler HA. Vitamin D status in early pregnancy and risk of preeclampsia. Am J Obstet Gynecol. 2015 Apr;212(4):511.e1-7. doi:10.1016/j.ajog.2014.11.009.
- Khalessi N, Kalani M, Araghi M, Farahani Z. The Relationship between Maternal Vitamin D Deficiency and Low Birth Weight Neonates. J Family Reprod Health. 2015;9(3):113-117.
- Mohammad-Alizadeh-Charandabi S, Mirghafourvand M, Mansouri A, Najafi M, Khodabande F. The Effect of Vitamin D and Calcium plus Vitamin D during Pregnancy on Pregnancy and Birth Outcomes: a Randomized Controlled Trial. J Caring Sci. 2015;4(1):35-44. doi:10.5681/jcs.2015.004.
- Thorne-Lyman A, Fawzi WW. Vitamin D during pregnancy and maternal, neonatal and infant health outcomes: a systematic review and meta-analysis. Paediatr Perinat Epidemiol. 2012;26 Suppl 1(0 1):75-90. doi:10.1111/j.1365-3016.2012.01283.x.
- Mahon P, Harvey N, Crozier S, Inskip H, Robinson S, Arden N, Swaminathan R, Cooper C, Godfrey K; SWS Study Group. Low maternal vitamin D status and fetal bone development: cohort study. J Bone Miner Res. 2010;25(1):14-9. doi:10.1359/jbmr.090701.
- Maugeri A, Barchitta M, Blanco I, Agodi A. Effects of Vitamin D Supplementation During Pregnancy on Birth Size: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2019;11(2):442. doi:10.3390/nu11020442.
- Husain AN, Siddiqui NH, Stocker JT. Pathology of arrested acinar development in postsurfactant bronchopulmonary dysplasia. Human Pathology. 1998;29(7):710-717.
- Jobe AH. The new bronchopulmonary dysplasia. Curr Opin Pediatr. 2011;23(2):167–72. https://doi.org/10.1097/MOP.0b013e3283423e6b.
- Thebaud B, Abman SH. Bronchopulmonary dysplasia: Where have all the vessels gone? Roles of angiogenic growth factors in chronic lung disease. American Journal of Respiratory and Critical Care Medicine. 2007 May 15;175(10):978-85.
- Baker CD, Alvira CM. Disrupted lung development and bronchopulmonary dysplasia: opportunities for lung repair and regeneration. Curr Opin Pediatr. 2014;26(3):306–14. https://doi.org/10.1097/MOP. 0000000000000095.
- Mandell E, Seedorf GJ, Ryan S, Gien J, Cramer SD, Abman SH. Antenatal endotoxin disrupts lung vitamin D receptor and 25-hydroxyvitamin D 1-alpha-hydroxylase expression in the developing rat. Am J Physiol Lung Cell Mol Physiol. 2015; 309(9):L1018–26. https://doi.org/10.1152/ajplung.00253.2015.
- Serce Pehlevan O, Karatekin G, Koksal V, Benzer D, Gursoy T, Yavuz T, et al. Association of vitamin D binding protein polymorphisms with bronchopulmonary dysplasia: a case-control study of Gc globulin and bronchopulmonary dysplasia. J Perinatol. 2015;35(9):763–7. https://doi.org/10.1038/jp.2015.58.
- Koroglu OA, Onay H, Cakmak B, Bilgin B, Yalaz M, Tunc S, et al. Association of vitamin D receptor gene polymorphisms and bronchopulmonary dysplasia. Pediatr Res. 2014;76(2):171–6. https://doi.org/ 10.1038/pr.2014.63.
- NICE. Antenatal care. Available at: http://www.nice.org.uk.

Reconsiderarea strategiei pentru pacientele cu răspuns ovarian scăzut. Ce ştim acum? La ce ne putem aştepta în viitor?
Mihai Surcel, Iulia Neamţiu, Georgiana Nemeti, Alina Surcel, Iulian Goidescu, Daniel Mureşan, Dan Axente
Stabilirea strategiei pentru pacientele „poor responders” continuă să rămână o mare provocare pentru clinicieni. Prezenţa unui num...
Managementul rezultatelor anormale în urma screeningului pentru cancer de col uterin în timpul sarcinii
Ioana Cristina Rotar, Suzana Mariam Chaikh-Sulaiman, Antonia Mihaela Levai, Monica-Mihaela Cîrstoiu, Daniel Mureşan
În prezent, s-a înregistrat o tendinţă de creştere a detectării cancerelor ginecologice în cursul sarcinii, în principal din cauza...
Impactul fibroamelor asupra ratei fertilităţii. Management chirurgical şi rezultate obstetricale
Andreea Elena Dumitru, Tamara Maria Pătraş, Nicolae Gică, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu
Fibroamele uterine sunt cea mai frecventă tumoră benignă la femeile de vârstă reproductivă. Atunci când sunt simptomatice, se mani...
Reconsiderarea strategiei pentru pacientele cu răspuns ovarian scăzut. Ce ştim acum? La ce ne putem aştepta în viitor?
Mihai Surcel, Iulia Neamţiu, Georgiana Nemeti, Alina Surcel, Iulian Goidescu, Daniel Mureşan, Dan Axente
Stabilirea strategiei pentru pacientele „poor responders” continuă să rămână o mare provocare pentru clinicieni. Prezenţa unui num...
Managementul rezultatelor anormale în urma screeningului pentru cancer de col uterin în timpul sarcinii
Ioana Cristina Rotar, Suzana Mariam Chaikh-Sulaiman, Antonia Mihaela Levai, Monica-Mihaela Cîrstoiu, Daniel Mureşan
În prezent, s-a înregistrat o tendinţă de creştere a detectării cancerelor ginecologice în cursul sarcinii, în principal din cauza...