Provocări în tratamentul multimodal adjuvant/neoadjuvant al cancerelor rectale avansate local. Prezentare de caz
Challenges in the neoadjuvant/adjuvant multimodal treatment in locally advanced rectal tumors. Case report
Abstract
The incidence of colorectal cancer in the European Union is in continuous growth and approximately 15% of the cases present with a hereditary component, the most frequently encountered associations being with the Lynch syndrome and familial adenomatous polyposis. Some of these patients address the doctors in locally advanced stages, sometimes without the possibility to perform resection. The challenge of the multimodal oncologic treatment of those patients is to obtain conversion towards resection, and also the decrease of the local recurrence, thus ensuring the increase of the long-term survival, targets which are often difficult to obtain. We present the case of a 54-year-old patient with locally advanced rectal cancer, who benefitted from multimodal treatment: neo-adjuvant chemotherapy and radiotherapy, and also from surgical intervention.Keywords
locally advanced rectal tumormultimodal treatmentneo-adjuvant treatmentRezumat
Incidenţa cancerului rectal în Uniunea Europeană este în continuă creştere, aproximativ 15% din cazuri prezentând o componentă ereditară, cele mai frecvente asocieri fiind cu sindromul Lynch şi polipoza adenomatoasă familială. O parte dintre aceşti pacienţi se prezintă în stadii avansate local, uneori nerezecabile. Provocarea tratamentului oncologic multimodal al acestor pacienţi este de a obţine conversia către rezecabilitate, precum şi scăderea incidenţei recurenţei locale, asigurând astfel creşterea supravieţuirii la distanţă, deziderate ce sunt adesea greu de obţinut. Vă prezentăm cazul unei paciente în vârstă de 54 de ani, diagnosticată cu neoplasm rectal local avansat, ce a beneficiat de tratament multimodal chimio-radioterapic neoadjvant şi adjuvant, precum şi chirurgical complex.Cuvinte Cheie
neoplasm rectal avansat locoregionaltratament multimodaltratament neoadjuvantIntroduction
The incidence of rectal cancer in the European Union is 15-25/100,000 per year (35% of the total colorectal cancer incidence)(1,2). The mortality has decreased with 35% due to prevention, early diagnosis and advances in the multimodal treatment of rectal cancer(1,2). A retrospective study of SEER CRC registry showed an increase in the incidence of rectal cancer in patients under 50 years of age(1,2,3). Approximately 15% of cases have a hereditary component. The most common disorders are Lynch syndrome and familial adenomatous polyposis(1,2).Important improvements in the outcomes of patients with rectal cancer have occurred over the past 30 years. Advances in surgical pathology, refinements in surgical techniques and instrumentation, new imaging modalities, and the widespread use of neoadjuvant therapy have all contributed to these improvements. Many new systemic treatment options have become available for locally advanced rectal cancers, including: additional chemotherapeutic agents and targeted therapies (vascular-endothelial growth factor and epidermal growth factor receptor inhibitors) which can be added to neoadjuvant and adjuvant regimens or given in combination with radiotherapy as radio-sensitizing agents. An important aim is to treat so that the risk of residual disease in the pelvis, frequently causing a disabling local recurrence, is very low. Neoadjuvant/adjuvant therapy of stage II (T3-4, node-negative disease with tumor penetration through the muscle wall) or stage III (node-positive disease without distant metastasis) rectal cancer often includes locoregional treatment due to the relatively high risk of locoregional recurrence(4,5,6,7,8,9,10). We report a case of a 54-year-old patient diagnosed with locally advanced rectal cancer and treated with a multimodal approach.


Case report
In November 2013, a 52-year-old female, smoker patient, presented at the primary care physician accusing rectal bleeding, pain and perianal abscess. A colonoscopy was performed and she was diagnosed through a biopsy with rectal adenocarcinoma. She was redirected to our department, at the “Prof. Dr. Al. Trestioreanu” Institute of Oncology, in Bucharest.
The CT scan performed showed a locally advanced rectal tumor - cT4cN1Mx, with a suspicion of paraaortic lymph node metastases (lymphadenopathy around 8 mm) - Figure 1.
Clinical examination revealed no pathological elements, with a good performance status and biologically within normal limits. The tumor board decided that the best treatment sequence was neoadjuvant chemo-radiotherapy and then surgery. A protective ileostomy was performed (Figure 2).
Treatment
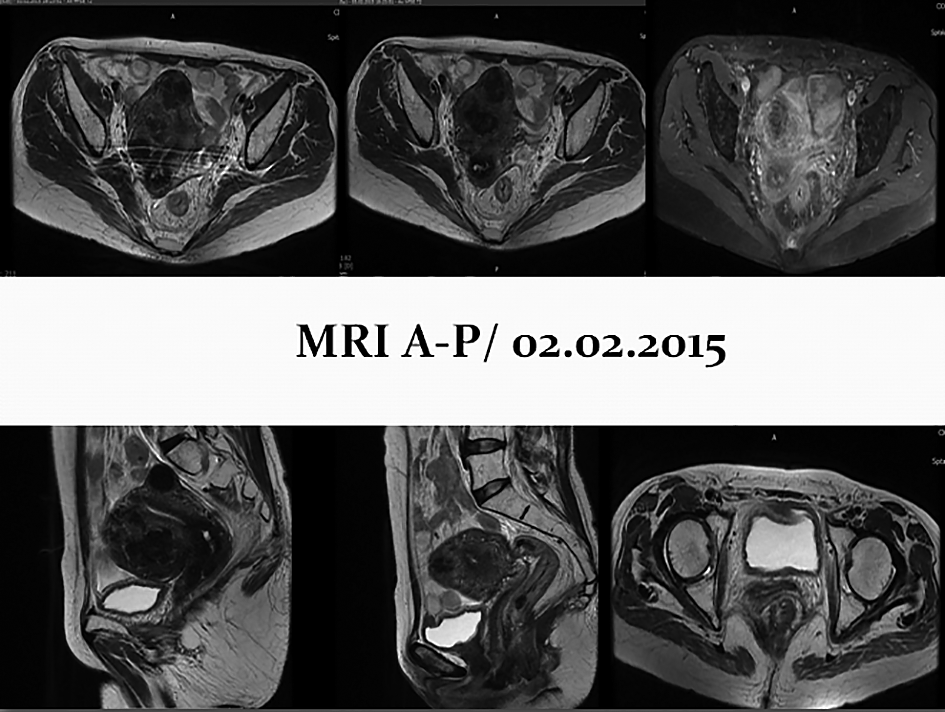
The patient started neoadjuvant chemo-radiotherapy in January 2014 (TD=45 Gy, 1.8 Gy per fraction/25 fractions + Capecitabine 1000 mg per day). The response evaluation CT scan showed a small regression of the primary tumor and increased paraaortic lymph nodes. So the patient was restaged: stage IV rectal adenocarcinoma - cT4N1M1a (LYM) - Figure 3.We evaluated the K-RAS status and the results showed that the patient had an exon 4 mutation in the K-RAS gene. Chemotherapy was continued with Cape Ox (Oxaliplatin 130 mg/m2 d1+ Capecitabine 1000 mg/m2, PO, twice daily, for 14 days, repeated every 3 weeks) + Bevacizumab (7.5 mg/kg, d1Q3) for 6 months. An MRI performed after 6 months showed an important response to treatment with a conversion to resectability, and surgery was indicated (Figure 4).
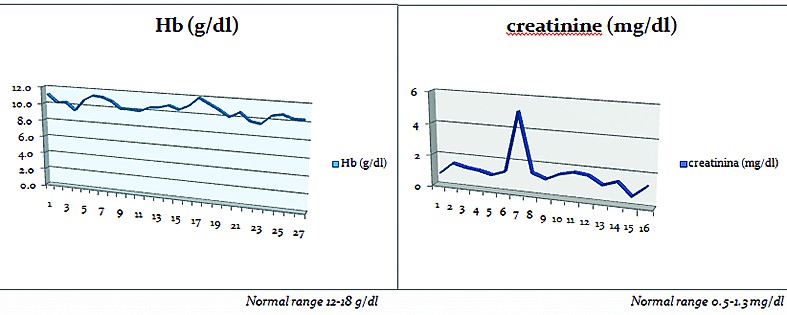
The patient underwent radical surgery in January 2015 (total hysterectomy with bilateral ovariectomy, rectum amputation and colpectomy). Subsequent chemotherapy was continued with Cape Ox (Oxaliplatin 130 mg/m2 d1+ Capecitabine 1000 mg/m2, PO, twice daily, for 14 days, repeated every 3 weeks) + Bevacizumab (7.5 mg/kg, d1Q3). During chemotherapy, mild gastrointestinal (nausea, vomiting, diarrhea) and hematological toxicity was observed and the patient experienced for a short period of time fatigue, asthenia, muscle weakness, numbness in limbs. The patient had an allergic reaction to Oxaliplatin, so the treatment was switched to FU/leucovorin+Bevacizumab. During this period the patient presented dysuria and her chemistry work-up revealed increased serum creatinine (5.1 mg/dl), hypocalcaemia, hypokalemia, hyponatremia. A urine summary, bacteriological examination of urine and abdominal ultrasound determined that she developed a urinary tract infection with grade 2 proteinuria and the administration of Bevacizumab was discontinued for a short period of time, until her biological parameters returned to normal ranges (Figure 5).
Results/follow-up
The follow-up (clinical and bio-umoral evaluation, CT scan) showed no locoregional tumor relapse, no new metastases and a decrease in size of the paraaortic lymph nodes. The multimodal approach of the treatment (RT/CHT, surgery, CHT, targeted therapy) led to a good outcome in this case, with the conversion to resectability of the rectal tumor and no late important morbidity problems. Regarding prognostic factors in this case - stage IV rectal cancer, with a high risk of recurrence, paraaortic lymph nodes involvement, side effects of the treatment (grade 2 proteinuria) that can lead to discontinuation of Bevacizumab - we can establish a poor prognostic for this patient.
Discussions
The sequence is the most important multimodal therapy in rectal cancer. In this case, the choice of sequence radio-chemotherapy and targeted therapy resulted in partial remission and conversion to resectability of the tumor. In terms of outcome, patient falls in the category of high risk for locoregional recurrence, with a risk of 49% of recurrence in the low pelvic region and presacral regions, as Yu et al. reported in a single center study(1,2). Prevention from local failures with the severe morbidity which may accompany them is very important. The prognosis is also influenced by late effects of treatment toxicity and radio-chemotherapy, with the patient having gastrointestinal toxicity, hematologic and even proteinuria during treatment(1,2,4,7,10).In a retrospective study published in 2015 by Hsueh-Ju Lu, with a total of 4,527 newly diagnosed CRC patients who were enrolled, the authors aimed to assess the prognostic role of visible paraaortic lymph nodes (PALNs). An inferior overall survival was seen in patients with visible PALNs than in those without visible PALNs (5-year overall survival, 67% vs. 76%, P = 0.015). Lymph vascular invasion, nodal disease (pN+) status, high preoperative serum carcinoembryonic antigen (CEA) levels and visible PALNs ≥10 mm were independent prognostic factors for patients with visible PALNs. They concluded that a prognostic model, which included LVI, pN+ status, preoperative serum CEA level, and the size of visible PALNs, could effectively distinguish the outcome of patients with visible PALNs. Our patient had para-aortic lymph nodes visible on MRI around 1.4 cm and it should be taken in for discussion if radiotherapy of the para-aortic lymph nodes is indicated and what are its benefits for the patient, considering their localization and the toxicities of the radiotherapy treatment(13,14,15).
In 2010, a meta-analysis performed on 16 studies that included 12,268 patients with various malignancies evaluated the risk of developing proteinuria by the addition of Bevacizumab to chemotherapy. The study showed that Bevacizumab added to chemotherapy significantly increased the risk for high-grade proteinuria in patients with different types of cancer.
The risk is different with dosage of Bevacizumab and tumor type. The incidence of high-grade (grade 3 or 4) proteinuria with Bevacizumab was 2.2%. Compared with chemotherapy alone, Bevacizumab combined with chemotherapy significantly increased the risk for high-grade proteinuria and nephrotic syndrome. Bevacizumab administrated in high doses (10-15 mg/kg) was associated with increased risk for proteinuria.
The authors concluded that the addition of Bevacizumab to chemotherapy significantly increases the risk for high-grade proteinuria and nephrotic syndrome, with the possibility of developing renal failure and cardiovascular complications. Our patient developed grade 2 proteinuria and the administration of Bevacizumab was discontinued for a short period of time. At the moment, the patient has a normal biological profile, without any proteinuria and she is continuing her treatment in the adjuvant setting(1,2,9,12).
Conclusions
The neo-adjuvant chemotherapy and radiotherapy treatment have a special role in the management of locally advanced rectal cancer, by being able to provide conversion to the stage in which resection can be performed, even if this fact might imply a complex surgical intervention.The association of the adjuvant chemotherapy treatment may improve the results and the long-term perspectives of the patients, by decreasing the incidence of local recurrence.
Bibliografie
1. NCCN guidelines version 3.2015-rectal cancer (http://www.nccn.org)
2. B. Glimelius et al. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up, Annals of Oncology 24 (Supplement 6): vi81–vi88, 2013, doi:10.1093/annonc/mdt240
3. http://www.ascopost.com/issues/april-10,-2015/colorectal-cancer-is-significantly-increasing-among-younger-adults-and-being-diagnosed-at-later-stages.aspx
4. http://www.ascopost.com/issues/march-25,-2015/optimal-timing-of-rectal-surgery-60-days-or-less-post-chemoradiation-therapy.aspx
5. http://www.ascopost.com/issues/january-25,-2015/colorectal-cancer-2015.aspx
6. http://www.ascopost.com/issues/july-25,-2014/benefit-confirmed-for-adjuvant-oxaliplatin-in-rectal-cancer.aspx
7. Ciara R Huntington, et al. Optimal timing of surgical resection after radiation therapy in locally advanced rectal adenocarcinoma: An analysis of the National Cancer Database (NCDB), J Clin Oncol 33, 2015 (suppl 3; abstr 510).
8. Yanhong Deng, et al. A multi-center randomized controlled trial of mFOLFOX6 with or without radiation in neoadjuvant treatment of local advanced rectal cancer (FOWARC study): Preliminary results, J Clin Oncol 33, 2015 (suppl; abstr 3500).
9. Joshua Smith et al. Advances and Challenges in Treatment of Locally Advanced Rectal Cancer, April 27, 2015, doi: 10.1200/JCO.2014.60.1054.
10. Chau et al. Neoadjuvant capecitabine and oxaliplatin followed by synchronous chemoradiation and total mesorectal excision in magnetic resonance imaging-defined poor-risk rectal cancer, J Clin Oncol. 2006 Feb 1; 24(4):668-74.
11. M. Wasif Saif. Managing Bevacizumab-Related Toxicities in Patients with Colorectal Cancer, MD, J Support Oncol 2009; 7:245–251.
12. Shenhong Wu et al. Bevacizumab Increases Risk for Severe Proteinuria in Cancer Patients, J Am Soc Nephrol. 2010 Aug; 21(8): 1381–1389.
13. Ju HJ, Lin JK, Chen WS, Jiang JK, Yang SH, et al. The Prognostic Role of Para-Aortic Lymph Nodes in Patients with Colorectal Cancer: Is It Regional or Distant Disease, (2015). PLoS ONE 10(6): e0130345. doi:10.1371/journal.pone.0130345.
14. G Cserni et al. Nodal staging of colorectal carcinomas and sentinel nodes, J Clin Pathol. 2003 May; 56(5): 327–335.
15. Tomonori M. et al., Complete Response of Isolated Para-aortic Lymph Node Recurrence from Rectosigmoid Cancer Treated by Chemoradiation Therapy with Capecitabine/Oxaliplatin plus Bevacizumab: A Case Report, Case Rep Oncol. 2012 May-Aug; 5(2): 216–221.

UMFCD dă startul înscrierilor pentru examenul de admitere, sesiunea iulie 2026
Cristina Ghioca
În perioada 6-17 iulie, la Universitatea de Medicină și Farmacie „Carol Davila”( UMFCD) din București au loc înscrierile pentru concursul de admitere la programele de studii universitare de licență.
...
Agoniștii GLP-1 pentru slăbit, utili și în ameliorarea bolilor de piele
Cristina Ghioca
Studii recente arată că medicamentele pentru slăbit din clasa GLP-1 au efecte benefice și în cazul afecțiunilor dermatologice.
....jpg)
Centru de diagnosticare a vertijului la SCJU Bihor
Cristina Ghioca
Spitalul Clinic Județean de Urgență Bihor a achiziționat echipamente moderne pentru diagnosticul afecțiunilor vestibulare și al sindroamelor vertiginoase, devenind astfel primul centru din județul Bihor care are astfel de aparatură.
...
UMFCD dă startul înscrierilor pentru examenul de admitere, sesiunea iulie 2026
Cristina Ghioca
În perioada 6-17 iulie, la Universitatea de Medicină și Farmacie „Carol Davila”( UMFCD) din București au loc înscrierile pentru concursul de admitere la programele de studii universitare de licență.
...
Agoniștii GLP-1 pentru slăbit, utili și în ameliorarea bolilor de piele
Cristina Ghioca
Studii recente arată că medicamentele pentru slăbit din clasa GLP-1 au efecte benefice și în cazul afecțiunilor dermatologice.
...
Centru de diagnosticare a vertijului la SCJU Bihor
Cristina Ghioca
Spitalul Clinic Județean de Urgență Bihor a achiziționat echipamente moderne pentru diagnosticul afecțiunilor vestibulare și al sindroamelor vertiginoase, devenind astfel primul centru din județul Bihor care are astfel de aparatură.
...