Analiza transnosografică a disfuncţiei executive – dimensiuni clinice, psihometrice şi terapeutice (II)
Transnosographic analysis of executive dysfunction – clinical, psychometric and therapeutic dimensions (II)
Abstract
Impairments in planning, selective attention, initiation of activities, interference control, inhibition of response, decreased self-control/self-monitoring, reduced cognitive flexibility, working memory, verbal fluency, difficulties in decision-making and abstract thinking in patients with psychiatric disorders are analyzed on four dimensions: 1) validity of psychometric assessments, 2) possible neurocognitive endophenotypes, 3) severity of the functional consequences, and 4) observed changes in cognitive functioning during treatment. The “theories of mind” abnormalities are associated with executive dysfunction, according to several studies, in the pathogenesis of autism spectrum disorders, substance use disorders and borderline personality disorder. This second section of the review explores the available evidence about the types of executive dysfunctions and their consequences in patients with anxiety disorders, personality disorders, substance use disorders, behavioral addictions, autism spectrum disorders, intellectual disability, or attention deficit/hyperactivity disorder. The inclusion of the cognitive dimension in the case management, with periodic, structured measurement (especially of the executive dysfunction), is considered to have a significant impact on achieving full recovery and/or on improving daily functionality and the quality of life in patients with mental disorders. However, more research is needed to determine the responsivity of executive dysfunction to existing therapeutic interventions, as well as to evaluate the most appropriate guideline for monitoring these dysfunctions in specific mental disorders.Keywords
executive functionsquality of lifetheories of mindanxiety disorderspersonality disordersautism spectrum disordersRezumat
Deficitele la nivelul planificării, atenţiei selective, iniţierii activităţilor, controlului interferenţelor şi inhibiţiei răspunsului, diminuarea autocontrolului şi automonitorizării, reducerea flexibilităţii cognitive, a memoriei de lucru, a fluenţei verbale, a capacităţii decizionale şi a gândirii abstracte, întâlnite la pacienţii cu tulburări psihice, sunt analizate într-un cadru sistematic, urmărindu-se patru dimensiuni: validitatea evaluărilor psihometrice, prezenţa unor endofenotipuri neurocognitive, impactul funcţional şi modificările funcţiilor cognitive sub tratament. Legătura dintre erorile observate la nivelul „teoriilor minţii” şi disfuncţia executivă este susţinută de unele cercetări în patogeneza tulburărilor de spectru autist, a dependenţelor de substanţă şi a tulburării de personalitate borderline. În această a doua parte a analizei sunt prezentate datele existente referitoare la tipurile de disfuncţii executive şi la consecinţele lor în cadrul tulburărilor de anxietate, tulburărilor de personalitate, tulburărilor legate de consumul de substanţe, adicţiilor comportamentale, tulburărilor de spectru autist, dizabilităţii intelectuale şi tulburării de hiperactivitate cu deficit de atenţie. Includerea în managementul de caz a dimensiunii cognitive, cu evaluarea periodică a acesteia (în special componenta de disfuncţie executivă), este considerată a avea un impact semnificativ asupra obţinerii recuperării complete şi/sau a îmbunătăţirii funcţionalităţii cotidiene şi a calităţii vieţii pacienţilor cu tulburări psihice. Mai multe cercetări sunt însă necesare pentru a stabili nivelul de răspuns al disfuncţiilor executive la intervenţiile terapeutice existente, precum şi pentru a determina cel mai adecvat protocol de monitorizare a acestor disfuncţii în funcţie de patologia psihică specifică.Cuvinte Cheie
funcţii executivecalitatea vieţiiteoriile minţiitulburări anxioasetulburări de personalitatetulburări de spectru autistIntroduction
In this second part of the review, executive dysfunction analysis is continued, with a special focus on anxiety disorders, substance and behavioral addictions, personality disorders, autism spectrum disorders, attention-deficits/hyperactivity disorder (both in children and adults), and intellectual disability. While the controversy about the real-world validity of the psychometrically-determined executive dysfunction still exists, evidence about the utility of actively searching for cognitive impairments and about their inclusion in therapeutic protocols is gathering.
Executive dysfunctions associated to specific psychiatric disorders
Anxiety disorders
Cognitive dysfunction in patients with anxiety disorder may be identified at several levels: attentional processes abnormalities, deficits in working, episodic or autobiographical memory, maladaptive cognitions and erroneous metacognitive strategies(1). Although all these domains have importance for pathogenesis and psychotherapy, the possibility to quantify their correlation with clinical symptoms or their associated impairments in daily life is very limited.
According to a meta-analysis, patients with obsessive-compulsive disorder (OCD) were significantly impaired in tasks which measured visuospatial memory, executive function, verbal memory and verbal fluency, whereas auditory attention was preserved(2). The largest effect size was calculated for the capacity to recall complex visual stimuli(2). The same analysis reported effect sizes for executive function, verbal memory and verbal fluency in the small-to-medium range(2).
In a cohort study (N=82,360 community-dwelling people), the presence of an anxiety disorder (panic disorder ± agoraphobia, agoraphobia, social phobia) was associated with worse performance on the Ruff Figural Fluency Test (RFTT), independent of comorbid depression(3). No dose-relationship with the number of anxiety disorders was found in this cohort(3). Agoraphobia was associated with worse executive functioning, which suggests the importance of evaluating this aspect during the treatment of specific anxiety disorders(3).
In a longitudinal study, initial poor inhibition, set-shifting, working memory updating, inductive reasoning and global cognition anticipated more severe generalized anxiety symptoms at the nine-year follow-up visit(4). The same analysis did not find predictive value for processing speed, verbal working memory, verbal fluency and episodic memory(4).
The neuropsychological assessment of patients diagnosed with social anxiety disorder (N=30), using Wisconsin Card Sorting Test (WCST), the Trail-making test, the Word Fluency test and the Auditory Verbal Learning test, found several differences versus healthy controls(5). Patients showed lower performance on WCST, and the Liebowitz Social Anxiety Scale score correlated significantly with the number of perseverative errors of the WCST(5). Therefore, executive functioning of patients with social anxiety disorder may be lower than in healthy individuals, and it may require a specific therapeutic approach.
Comorbid anxiety in hospitalized patients with unipolar depression (N=22) was associated with worse memory function than in controls, evaluated on a broad battery of neuropsychological tests(6). Although the patients with major depression without comorbid anxiety had this type of memory dysfunction too, the comorbid anxiety group also had more impaired scores then either the non-anxious depressed group or the control group(6). The co-occurrence of anxiety was associated with psychomotor slowing, beside the memory deficits(6).
Searching for neurocognitive endophenotypes in anxiety disorders has involved executive function components of decision-making, planning, response inhibition, behavioral reversal/alternation, reversal learning and set-shifting/cognitive flexibility as possible candidates for OCD(7). Relatives of patients diagnosed with OCD performed poorer at Iowa Gambling Test, Tower of Hanoi and WCST, when compared to healthy controls and their relatives(8).
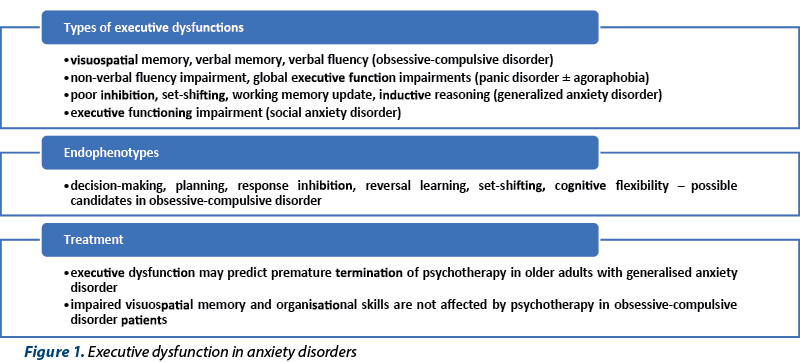
Executive dysfunction may be used as a predictor of premature termination of the cognitive-behavioral therapy in older adults diagnosed with generalized anxiety disorder(9). Homework compliance and quality of these tasks but also indices of cognitive restructuring are predicted by executive dysfunction in this population(9). Patients who improved their executive skills during psychotherapy also responded best in term of worry reduction(9).
In a group of patients diagnosed with OCD (N=39), memory and executive functions could not predict the outcome of the cognitive-behavioral therapy, but the level of social functioning could have such a predictive value(10). Therefore, the evaluation of baseline executive functioning could not help in determining which patients may benefit from cognitive-behavioral therapy(10). No memory or executive function changes have been reported during psychotherapy for OCD in the same group of patients(11). The persistence of poor Rey complex figure test scores suggests impaired visuospatial memory and organizational skills that may be trait related, not state-dependent(11). These performances were worse than in healthy controls both before and after the cognitive-behavioral therapy(11).
Personality disorders
Impairments of the executive functioning in individuals with personality disorders (PD) are inconsistent when compared to matched controls(12). Significant deficits have been reported in decision-making, working memory, inhibition and flexibility, but the existing data are limited to borderline, obsessive-compulsive, antisocial, narcissistic and schizotypal PD(12).
Neurocognitive deficits – and especially executive function impairments – have been considered by several authors as the core to the development of borderline personality disorder (BPD)(13). This perspective is supported by the high comorbidity rate between BPD and disorders characterized by poor executive functioning(13). BPD patients showed deficits in planning in comparison with bipolar disorder patients and healthy controls, based on the CANTAB administration results(14). BPD was also associated with deficits in problem-solving when compared to healthy controls(14). The same personality disorder was associated with deficient executive functioning in another trial where patients were compared to healthy controls, healthy unaffected parents of patients and their age-matched controls (27, 29, 20 and 22 individuals)(15). Cognitive planning, sustained attention and working memory were affected in BPD patients as compared to healthy controls, and both patients and their parents showed reduced latency to initiate the first move on the planning task in the Tower of London test(15). In yet another trial, working memory tasks were affected in BPD patients (N-back test), but problem-solving times were shorter and the quality of task-solving was comparable with that of healthy controls(16).
Individual differences in executive function and emotion recognition may explain the theory of mind variability in BPD(17). Tasks involving real-life social scenarios and contextual cues are more sensitive to detect theory of mind deficits in BPD patients, and they helped correlating these deficits with difficulties in integrating cues from face, prosody, gesture and social context to identify emotions and others’ belief(17).
Because PD are often comorbid with other psychiatric disorders, questions have been raised about the possibility of executive dysfunction misattribution. As a consequence, the existing data have been analyzed from this perspective, and deficits of executive function may be considered a common vulnerability for both BPD and the disorders with which it is frequently comorbid(13). Evidence that these deficits are uniquely associated with BPD, independent of comorbid conditions, is limited(13).
The exploration of possible endophenotypes of personality disorders based on neurocognitive variables led to the observation that BPD patients had lower response inhibition than their first-degree biological relatives(18). Both lower interference resolution and response inhibition discriminated probands from relatives and controls, while a combination of less efficient problem solving and difficulty manipulating mental information differentiated probands and relatives from controls(18). A stronger response inhibition and more developed abstract reasoning abilities despite less efficient problem solving were associated in a subset of healthy relatives with resilience to psychiatric morbidity(18).
In patients with antisocial personality disorder (N=85), CANTAB results showed deficits regarding the executive functions, attention, visual short-term and working memory versus controls(19). Deficits in inhibitory control and working memory appear to distinguish antisocial from other personality disorders(19).
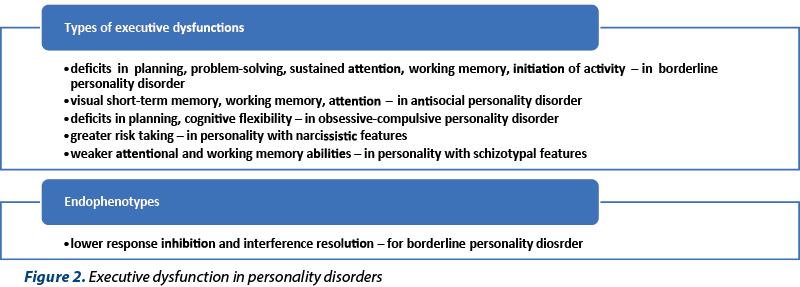
Obsessive-compulsive personality disorder (OCPD) has been correlated with impaired cognitive flexibility and planning ability compared to healthy controls, and there are some differences between the neuropsychological profile of this disorder and OCD(20). While both types of disorders were associated with more perseverative errors on the WCST than controls, the OCD patients completed significantly fewer categories than the controls(20). Both groups of patients required significantly more moves than control subjects to complete the Tower of London test, and those with OCD required longer time than patients with OCPD and than healthy controls to complete the task(20). In another trial, the presence of obsessive-compulsive personality traits correlated with different performances on the Spatial Working Memory tasks, Intradimensional/Extradimensional tasks, Stockings of Cambridge, and the Dysexecutive Questionnaire, when compared to controls(21). Executive dysfunctions are present in people with prominent obsessive-compulsive features, and there is a high convergence between clinical and ecological determinants of executive functions in this population(21).
The investigation of the relation between narcissistic personality features and behavioral decision making in three studies (N=380, 244 and 312 participants, respectively) has led to the conclusion that grandiose and pathological narcissism could not predict decision making regardless of whether or not decision making included immediate feedback(22). The narcissistic trait of grandiosity (an inflated sense of self-importance) was associated with greater risk taking on the Columbia Card Task when immediate feedback was required, while the entitlement was associated with greater risk taking on the Iowa Gambling Test(22).
In patients with high schizotypal personality traits (N=400), weaker attentional abilities and working memory were detected than in individuals with low schizotypal features(23). Poorer overall executive functioning (reflected in the number of executive errors) was also reported in this population with high schizotypy(23). The investigations used in this trial to assess executive function were WCST, Stroop word-color test, Wechsler Digit Span test, and step-by-step listening sequence(23).
Substance use disorders and behavioral addictions
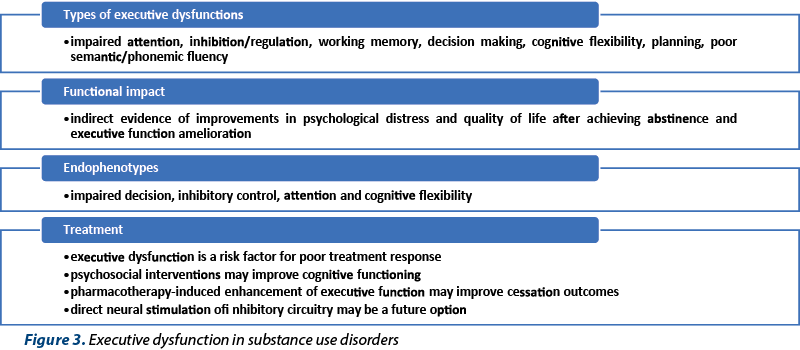
Both substance and behavioral addictions deserve a place in any analysis of executive dysfunction, with a special focus on their negative consequences over the quality of life, general functioning and risk of psychiatric complications(24,25). Altered cognitive functioning can be considered one of the core features of the substance use disorders (SUD), with the most frequently affected domains being attention, inhibition/regulation, working memory and decision making(26). Changes in the top-down mechanisms that regulate the motivational processes (appetitive or aversive) are important elements to consider when planning a therapeutic intervention(26). Pre-cognition (interoception, implicit processes), executive function and social cognition (metacognition, theory of mind) are all affected in patients with SUD(26). For each of these domains, there is evidence suggesting possible phenotypes and potential targets for treatment(26).
The tendency to discount delayed rewards was positively correlated with alcohol addiction severity (self-reported) and impulsivity(27). Cognitive impulsivity was the only significantly different variable in the choice tendency analysis between abstinent alcoholics patients and healthy controls (N=28)(27).
One year of abstinence in patients with polysubstance use disorder (N=115) was associated with improvements on executive functions, psychological distress and quality of life(28). This conclusion suggests that SUD treatment should be initially focused on stabilizing the patient and achieving abstinence, while more cognitively-demanding treatments should be added later in the therapeutic process(28).
In gambling disorder, the response inhibition is impaired, as reflected by the scores at Stop-Signal Task and Stop-Signal Task(29). Cognitive flexibility is also impaired in these patients, as reflected by their abilities during WCST completion(29). Performances at phonemic and semantic-fluency tasks have been significantly worse than in healthy controls, but not all the evidence supports this observation(29). Planning and decision-making have also been investigated in patients with gambling disorder, with most of the data supporting significant impairments(29). An evaluation of the executive functioning prior to decide what therapy would be more efficient in pathological gambling patients may increase the risk of therapeutic success(30). Food addiction and obesity may also have executive dysfunction underpinning, as the majority of behavioral addictions, although they are less explored than SUD(24).
Regarding the possible neurocognitive endophenotypes in SUD, impaired decision, inhibitory control, attention and cognitive flexibility have been suggested as possible vulnerability markers(31).
Executive dysfunction is considered a contributor to poor treatment adherence, worse clinical outcomes and relapse in SUD(32,33). Drug-induced deficits in executive function may hinder the ability of the patients to refrain from drug use, therefore treatment methods focused on the cognitive components in substance use disorders need to be extensively explored(34).
Lower Stroop interference scores predicted increased involvement in treatment for patients with opioid use disorder (longer length of stay within the therapeutic framework)(35). Scores on auditory verbal learning test and group intervention predicted the number of positive urine tests during a three-month follow-up(35). Working memory and inhibitory control could be predictors of treatment for patients with opioid use disorder(35).
From a therapeutic perspective, interventions focused on executive dysfunction correction should be carefully considered(36). Attentional bias modification training could be used to decrease the drug use, by targeting one dimension of the executive dysfunction in SUD(26). So far, the results are modest, but research is still ongoing(26). An approach for improving executive function in addiction is cognitive training, especially working memory training and inhibitory control training(32). These cognitive therapies were associated with reduced drug use in methadone-treated patients and problem drinkers compared to control conditions(32,37). Mindfulness improved self-control abilities in emotion regulation in both smokers and non-smokers, and positive changes were related to increased anterior cingulate cortex/medial prefrontal cortex activity (ACC/mPFC)(38). Smokers presented reduced ACC/mPFC activity in the self-control network before mindfulness training, but non-smokers did not have these initial problems(38). Executive function impairment detected in a sample of substance users did not directly predict worse addiction outcomes, nor difficulty acquiring or maintaining change processes and outcomes during the 12-step intervention(39). Executive dysfunction moderated the correlation between change processes and outcome in this population(39). Based on this analysis, change processes were strongly related to the outcome for unimpaired individuals, but weakly related in case of impaired individuals(39).
Patients with substance use disorder with a high level of executive dysfunction (N=15) may have persistent cognitive deficits even after one month of intensive outpatient program(40). These deficits were determined by using the CANTAB and the self-reported Behavior Rating Inventory of Executive Functioning questionnaire (BRIEF-A)(40). However, significant improvements in organization as a consequence of this outpatient program were detected(40). The remaining deficits may affect patients’ engagement and participation in treatment programs(40).
Medication is also recommended for improving the inhibitory function, and direct neural stimulation of inhibitory circuitry may be considered an alternative in SUD, but the research is still in its early stages(26). The efficacy of pharmacotherapy over executive function in SUD is a controversial issue. According to a review that evaluated the existing data about the effect of nicotine, bupropion, varenicline, disulfiram, acamprosate, nalmefene, naltrexone, methadone, buprenorphine and lofexidine over three core domains of executive function – working memory, inhibitory control and cognitive flexibility –, it is possible that pharmacotherapy-induced enhancement of executive function may improve cessation outcomes in dependent populations(32). Psychoactive drugs administered for improving working memory in SUD, in order to optimize the dopaminergic neurotransmission, may be considered(26). Pharmacologic options to improve decision-making – e.g., modafinil and atomoxetine – are being explored in SUD patients(26).
Autism spectrum disorder
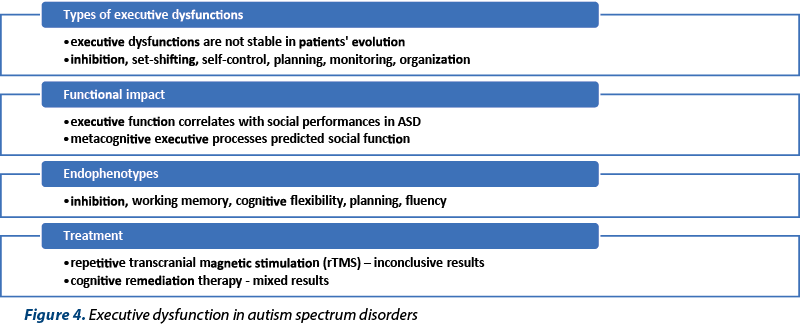
Executive dysfunction has been considered a promising endophenotype in neurodevelopmental disorders(41). According to a meta-analysis dedicated to executive dysfunction in autism spectrum disorders (ASD; n=235 studies, N=14081 participants), there is a moderate overall effect size for reduced performances during cognitive tasks(42). This meta-analysis confirmed the existence of a broad range of executive dysfunctions in patients with ASD that remain stable across the development(42). Unfortunately, the evaluation of individual subdomains of executive dysfunction is not supported by the currently administered psychometric instruments(42). Another meta-analysis (n=42 studies, N=2419 participants) compared adults presenting high-functioning autism (HFA) with typically developing adults, using neuropsychological tests for the measurement of five executive functioning domains: inhibition, working memory, flexibility, planning and fluency(43). A moderate overall effect size for decreased executive functioning across domains was found in patients versus controls(43). The most affected cognitive domains were flexibility and planning(43). These results may be useful when the therapeutic management is considered for individuals for HFA(43). Yet another review of 26 studies that examined patients diagnosed with ASD and ADHD showed that the executive function was affected in both disorders, especially in the domains of flexibility and planning (for the ASD group), and in the response inhibition deficit (within the ADHD group)(41). Deficits in attention, working memory, preparatory processes, fluency and concept formation do not appear to discriminate between ASD and ADHD groups(41).
Not only the ASD patients, but even unaffected siblings of ASD children may present impairments in executive function(44). In a study (N1=240 youths with ASD, N2=147 unaffected siblings, and N3=240 typically developing controls), the worst executive function tasks results were obtained by the patients, followed by the unaffected siblings(44). Relative to controls, siblings performed worse in forward and backward digit recalls and made more errors in spatial working memory, suggesting possible endophenotypes for ASD(44).
The existence of early executive function deficits in ASD is controversial, but there is evidence supporting significant differences between preschoolers with ASD and controls(45). Working memory, inhibition and shifting may be differentially affected by the presence of ASD, but these findings are moderated by mental and chronological age(45).
A polygenic score (PGS) for ASD was investigated in correlation to the severity of executive dysfunction in everyday life in a sample of 176 children, adolescents and young adults, aged 5-22 years old, without intellectual impairment(46). The common risk gene variants for ASD (or higher PGS) have been stronger associated with behavioral regulation aspects of executive dysfunction than ADHD risk/intelligence variants in a clinical sample of ASD patients(46).
Executive dysfunctions in ASD are not stable, as there is some evidence that age-related improvements from childhood to adolescence may appear(47). These observations suggest a prolonged window for effective treatment of executive dysfunctions in ASD(47). The natural evolution is not very favorable, because, despite the developmental gains, mature executive functioning is limited in ASD, as a reflection of impaired processing of information across all domains(47). Executive function correlates with social performances in ASD patients, and behavioral regulation executive processes (inhibition, shifting, emotional control) predicted social functioning in all children (patients and matched controls)(48). On the other hand, metacognitive executive processes (planning, monitoring, organization etc.) predicted social function only in ASD children, and not in typically developing children(48). Therefore, it seems that distinct metacognitive executive function-social symptom link in ASD may differentiate these patients from the general population(48).
Young patients diagnosed with autism presented impairments in executive functioning, both on set-shifting tasks (Intra-/Extradimensional test) and planning activities (Tower of London), when compared to non-autistic individuals with moderate learning disabilities and with normally developing children(49). The impairment was specific to the stages of each task that evaluated mostly the executive control(49).
A study that included 100 adolescents with ASD explored both the domains of theory of mind (how the patients understand other’s people perspectives) and the executive function, using 10 tasks, in order to verify if thinking ability impairments in ASD are linked to either of these domains or to both of them(50). Theory of mind ability was associated with both social communication symptoms and repetitive behaviors, while executive functioning correlated with theory of mind, but not directly with parent-reported symptom expression(50). Therefore, ASD behaviors could not be correlated with general thinking abilities, responsible for planning and executive tasks, suggesting that a different neuropsychological explanation is needed in this case(50).
A study focused on neural networks (N1=35 children with ASD and N2=40 IQ-matched controls) showed that the frontoparietal-insular cortex, including core nodes of the frontoparietal control and salience networks, had a significantly intense participation in children with normal development, but not in those with ASD during the executive functioning tasks(51). Changes in frontoparietal-insular participation coefficient predicted differences in executive function and behavioral symptoms in children with ASD, with repercussions over their ability to attend task-oriented activities, planning and organizing, as well as working memory functioning(51).
Treatment of executive function deficits in ASD has been researched, and transcranial magnetic stimulation (rTMS) was investigated in a double-blind, sham-controlled, pilot trial (N=40 patients, 16-35 year-olds)(52). A 20-session, four-week course of 20 Hz rTMS targeted the dorsolateral prefrontal cortex in ASD patients without intellectual deficits, but with impairment in their executive function(52). The overall results were not significant, as the differences between patients and controls were minor, but patients with more severe adaptive functioning deficits may benefit more than other patients from rTMS(52).
Cognitive remediation therapy for ASD patients has been explored as a potential treatment, with various results. This therapy using the frontal/executive program improved performance on BACS-J (Brief Assessment of Cognition in Schizophrenia) overall score, digit sequencing, verbal fluency and Tower of London tasks, but also on scales which evaluated social functioning(53).
Attention-deficit/hyperactivity disorder (ADHD)
ADHD affects 3-5% of school-age children, but in some cases this disorder may persist into adulthood (with an estimated prevalence of 1-3%)(54,55). Although no pathognomonic neuropsychological profile for this disorder has been identified, a number of studies explored the changes of executive functions and their impact in the real-world functionality in this population(55). Neuroimaging studies show disruption of the frontal-striatal-thalamic-cortical (FSTC) circuitry and cerebellum as the main causes of the cognitive and motor abnormalities seen in ADHD(55). Psychostimulant medication is considered to improve the executive functions through mediation of the underlying FSTC circuitry(55). Also, cognitive remediation training in adults presenting ADHD had positive results, with improvement of the organizational skills, in the same time decreasing the overall ADHD symptomatology and thelevels of anger(56).
The main executive dysfunction in ADHD is considered the weak inhibitory control(57). In children with ADHD, the main domains of executive functioning affected by the disorder were planning, sustained attention, cognitive flexibility, verbal fluency, inhibition response and working memory(58). In adults presenting with ADHD, the main disorders were reported in the domains of inhibitory response, capacity for planning, cognitive flexibility, verbal fluency and working memory (spatial working memory, logical or visual memory)(58). Several authors even consider that ADHD is essentially a cognitive disorder, a developmental impairment of executive functions which prevents the accomplishment of a wide variety of daily tasks(59).
A meta-analysis (n=83 studies, N1=3734 participants with ADHD, N2=2969 individuals without ADHD) showed significant impairment on all executive functioning tasks in patients versus controls, with effect sizes for all measures situated in the medium range (0.46 to 0.69)(60). Response inhibition, vigilance, working memory and planning were the most consistent effects detected in this population(60). These differences in executive functioning domains between patients and controls were not explained by group characteristics of intelligence, academic achievement or symptoms of other disorders(60). In conclusion, executive dysfunctions are not sufficient or necessary to explain the onset of ADHD in all cases, as they may be considered only one dimension of the complex neuropsychology of this disorder(60).
Working memory and verbal span have similar profile in patients with ADHD inattentive subtype and combined subtype (N=53 children, 7-10 years old), but the combined subtype was associated with lower performance in Simon task and with more impulsivity(57). On the other hand, the inattentive subtype correlated with lower performance in memory working tasks and planning(57). Therefore, differences in the executive functioning performances between the two subtypes exist, and they may be measured by neuropsychological tests. In another study, 357 children (aged 6-13 years old) diagnosed with ADHD were evaluated for response inhibition, response variability, speed, set-shifting, standardized intelligence and achievement level(61). Three clusters resulted based on the results of executive function tests: poor inhibitory control, poor set-shifting/speed and intact task performance(61). Intelligence, academic achievement and disruptive behavior/anxiety-mood symptoms were different between clusters, suggesting a high heterogeneity of executive dysfunctions among ADHD patients(61).
Neuropsychological deficits in ADHD have been investigated in a group of 30 children (6-14 years old, IQ>90, medication free) using Wechsler Intelligence Scale for Children (WISC-IV), Stroop test, WCST and Comprehensive Parent Rating Test (ADD-H)(54). Children diagnosed with ADHD presented an average IQ, symptoms of hyperactivity and executive dysfunction, confirmed by the Stroop test results and WCST(54). Children with ADHD were significantly more impaired on measures of executive dysfunctions than those without ADHD, in a study which compared 49 patients and 196 controls on eight variables(62). Only about 50% of children with ADHD had executive function deficits at the individual level, and the results were relatively robust across methods applied, which supports the high heterogeneity level of executive dysfunction impairment at the individual level(62).
In another study, both neuropsychological tests and real-life measures of executive function were administered in a group of 22 unmedicated boys with ADHD, and in a control group formed by 22 individuals matched on age and IQ with normal development(63). The ADHD group exhibited deficits in different variables of executive dysfunction – i.e., set-shifting (defined by perseverative errors and responses on WCST), and videogame play (fewer challenges completed)(63). Slow processing speed on the Stroop test and zoo activity, as well as slower rate of acquisition of the sorting rule on the WCST were reported by the ADHD patients(63). In conclusion, children with ADHD are affected by executive dysfunctions and processing speed impairments in real-world activities, as well as in neuropsychological testing situations(63). Therefore, the measurement of such executive deficits using validated tests could predict the functionality of these patients in real-world conditions.
Intellectual disability
A five-year longitudinal study compared the evolution of executive functions in adults with intellectual disability (N=46) and a control group with IQ≥85 (N=92)(64). Verbal fluency and executively loaded dual task word recall test at encoding were significantly impaired in adults with intellectual disability(64). After five years, no differences in executive functioning tests in patients were found when results were compared with initial results(64). The conclusion of this study is that individuals with intellectual disability have more problems with speed of accessing lexical items and difficulties with working memory-related executive control at encoding, including shifting between tasks(64).
Executive functioning analysis in 18 adults, aged between 22 and 57 years old, diagnosed with intellectual disability and evaluated using Barkley Deficits in Executive Functioning Scale, showed deficits in impulsivity, self-organization and self-emotional regulation(65). Therapeutic interventions focused on psychomotor training (which promotes adaptive and functional behaviors through movement and body experience) positively influenced outcomes in all domains, except for self-motivation(65). A five-month psychomotor intervention, with weekly sessions of 45 minutes of targeted psychomotor and cognitive-executive competences, improved more self-evaluated scores of executive functioning than those reported by others(65).
In females premutation/carriers of the fragile X mental retardation gene (N=20), significant impairments on the symbol digit modalities test, paced auditory serial addition test, behavioral dyscontrol scale and Haylings sentence completion task were reported compared to healthy controls (N=21)(66). All tasks requiring the rapid temporal resolution of responses were affected in the study group versus controls, suggesting the phenotype-based definition for this condition should include executive dysfunctions(66). An electroencephalography-based trial in patients diagnosed with fragile X-associated tremor/ataxia syndrome showed that P3 abnormalities were associated with lower executive function test scores and increased CGG repeat length of the fragile X mental retardation 1 (FMR1) gene, and with higher FMR1 mRNA levels(67). Abnormal frontoparietal attentional network dynamics explain the executive dysfunction, which is the main feature of cognitive impairment in the fragile X-associated tremor/ataxia syndrome(67).
Conclusions
Anxiety disorders are associated with multiple impairments in executive functioning, and there are different profiles of dysfunctions, although they do not possess significant degrees of specificity. While OCD patients have visuospatial and verbal memory, as well as verbal fluency deficits, in general anxiety disorder the most affected domains are inhibition of activities, set-shifting, working memory update and inductive reasoning processes(1-8). Patients with personality disorders have difficulties in planning (BPD, OCPD), problem-solving (BPD), attention (BPD, antisocial PD, schizotypal PD), working memory (BPD, antisocial PD, schizotypal PD), initiation of activities (BPD), visual short‑term memory impairments (antisocial PD), and decision impairments (narcissistic PD)(12-23). In patients with SUD, impaired attention, inhibition/regulation, working memory, decision making, cognitive flexibility and planning, as well as poor semantic/phonemic fluency have been reported(24-40). ASD have been associated with inhibition impairments, set-shifting, self-control, planning, monitoring and organizational deficits(44-51). Executive dysfunction in children and adults with ADHD have been described – e.g., weak inhibitory control, low ability for planning, reduced working memory, low verbal fluency(54-63). Difficulties in accessing lexical items, impaired working memory, decreased set-shifting and organizational abilities have been detected in patients with intellectual dysfunctions(64-67).
In patients with anxiety disorders, executive function impairments are relevant for the outcome of certain therapeutic interventions, because they may predict premature discontinuation(9,11). In several subgroups of anxiety disorders patients, executive dysfunction may indicate psychotherapy-resistance (e.g., impaired visuospatial memory in OCD patients)(9,11). Also, in SUD patients, executive dysfunction is a risk factor for poor treatment response, but both pharmacotherapy and psychotherapy may improve these patients’ cognitive outcome(26-37). ASD patients may benefit from the initiation of cognitive remediation therapy, psychomotor training may be efficient in improving executive functions in intellectual disability patients, and both cognitive remediation therapy and psychostimulants may improve cognitive outcomes in ADHD patients(52-55,65).
Neurocognitive endophenotypes could be defined, based on the reviewed data, in OCD, BPD, SUD and ASD(7,18,31,41-43). Functional impairment, especially in the psychosocial domain, correlated to executive dysfunction have been supported by evidence in patients diagnosed with substance use disorders, autism spectrum disorders and ADHD(24,25,28,48,63).
Individual differences in executive function and theory of mind variability have been correlated in patients diagnosed with BPD, ASD, and SUD(17,50). For example, theory of mind deficits have been associated with difficulties in integrating cues from face, prosody, gesture, and social context to identify emotions and others’ belief in BPD patients(17). Theory of mind ability was correlated with both social communication symptoms and repetitive behaviors in ASD, while metacognition and theory of mind were supposedly affected in SUD patients(26,50).
The inclusion of the cognitive evaluations in the case management, with periodic measurements, may have significant consequences in achieving full recovery and/or improving daily functionality and quality of life in patients with mental disorders.
Because not all the reviewed data are conclusive to support a correlation between psychometrically-determined impairments of executive function and real-life functioning, more research is needed in this direction. Also, future trials are required to determine the responsivity of executive dysfunction to the existing therapeutic interventions, as well as to evaluate the most appropriate guideline for monitoring these dysfunctions in specific mental disorders. n
Disclaimer: The author has no conflicts of interest to declare.
Bibliografie
-
Ferreri F, Lapp LK, Peretti CS. Current research on cognitive aspects of anxiety disorders. Curr Opin Psychiatry. 2011;24(1):49-54. doi: 10.1097/YCO.0b013e32833f5585.
-
Shin NY, Lee TY, Kim E, Kwon JS. Cognitive functioning in obsessive-compulsive disorder: a meta-analysis. Psychol Med. 2014;44(6):1121-30. doi: 10.1017/S0033291713001803.
-
Gulpers B, Lugtenburg A, Zuidersma M, Verhey FRJ, Oude Voshaar RC. Anxiety disorders and figural fluency: A measure of executive function. J Affect Disord. 2018;234:38-44. doi: 10.1016/j.jad.2018.02.038.
-
Zainal NH, Newman MG. Executive function and other cognitive deficits are distal risk factors of generalized anxiety disorder 9 years later. Psychol Med. 2018;48(12):2045-2053. doi: 10.1017/S0033291717003579.
-
Fujii Y, Kitagawa N, Shimizu Y, Mitsui N, Toyomaki A, Hashimoto N, et al. Severity of generalized social anxiety disorder correlates with low executive functioning. Neurosci Lett. 2013;543:42-6. doi: 10.1016/j.neulet.2013.02.059.
-
Basso MR, Lowery N, Ghormley C, Combs D, Purdie R, Neel J, et al. Comorbid anxiety corresponds with neuropsychological dysfunction in unipolar depression. Cogn Neuropsychiatry. 2007;12(5):437-56. doi: 10.1080/13546800701446517.
-
de Lima Muller J, Torquato KI, Manfro GG, Trentini CM. Executive functions as a potential neurocognitive endophenotype in anxiety disorders: A systematic review considering DSM-IV and DSM-5 diagnostic criteria classification. Dement Neuropsychol. 2015;9(3):285-294. doi: 10.1590/1980-57642015DN93000012
-
Cavedini P, Zorzi C, Piccinni M, Cavallini MC, Bellodi L. Executive dysfunctions in obsessive-compulsive patients and unaffected relatives: searching for a new intermediate phenotype. Biol Psychiatry. 2010;67(12):1178-84. doi: 10.1016/j.biopsych.2010.02.012.
-
Mohlman J. Executive skills in older adults with GAD: relations with clinical variables and CBT outcome. J Anxiety Disord. 2013;27(1):131-9. doi: 10.1016/j.janxdis.2012.12.001.
-
Vandborg SK, Hartmann TB, Bennedsen BE, Pedersen AD, Thomsen PH. Can memory and executive functions in patients with obsessive-compulsive disorder predict outcome of cognitive behavioural therapy? Nord J Psychiatry. 2016;70(3):183-9. doi: 10.3109/08039488.2015.1074282.
-
Vandborg SK, Hartmann TB, Bennedsen BE, Pedersen AD, Thomsen PH. Are there reliable changes in memory and executive functions after cognitive behavioural therapy in patients with obsessive-compulsive disorder? Cogn Neuropsychiatry. 2015;20(2):128-43. doi: 10.1080/13546805.2014.981649.
-
Garcia-Villamisar D, Dattilo J, Garcia-Martinez M. Executive functioning in people with personality disorders. Curr Opin Psychiatry. 2017;30(1):36-44. doi: 10.1097/YCO.0000000000000299.
-
McClure G, Hawes DJ, Dadds MR. Borderline personality disorder and neuropsychological measures of executive function: A systematic review. Personal Ment Health. 2016;10(1):43-57. doi: 10.1002/pmh.1320.
-
Gvirts HZ, Braw Y, Harari H, Lozin M, Bloch Y, Fefer K, Levkovitz Y. Executive dysfunction in bipolar disorder and borderline personality disorder. Eur Psychiatry. 2015;30(8):959-64. doi: 10.1016/j.eurpsy.2014.12.009.
-
Gvirts HZ, Harari H, Braw Y, Shefet D, Shamay-Tsoory SG, Levkovitz Y. Executive functioning among patients with borderline personality disorder (BPD) and their relatives. J Affect Disord. 2012;143(1-3):261-4. doi: 10.1016/j.jad.2012.05.007.
-
Hagenhoff M, Franzen N, Koppe G, Baer N, Scheibel N, Sammer G, et al. Executive functions in borderline personality disorder. Psychiatry Res. 2013;210(1):224-31. doi: 10.1016/j.psychres.2013.05.016.
-
Baez S, Marengo J, Perez A, Huepe D, Font FG, Rial V, et al. Theory of mind and its relationship with executive functions and emotion recognition in borderline personality disorder. J Neuropsychol. 2015;9(2):203-18. doi: 10.1111/jnp.12046.
-
Houdys JW, Ruocco AC. Executive functioning in adults with borderline personality disorder and first-degree biological relatives. World J Biol Psychiatry. 2021;1-14. doi: 10.1080/15622975.2021.2012396.
-
Baliousis M, Duggan C, McCarthy L, Huband N, Vollm B. Executive function, attention, and memory deficits in antisocial personality disorder and psychopathy. Psychiatry Res. 2019;278:151-161. doi: 10.1016/j.psychres.2019.05.046.
-
Paast N, Khosravi Z, Memari AH, Shayestehfar M, Arbabi M. Comparison of cognitive flexibility and planning ability in patients with obsessive compulsive disorder, patients with obsessive compulsive personality disorder, and healthy controls. Shanghai Arch Psychiatry. 2016;28(1):28-34. doi: 10.11919/j.issn.1002-0829.215124.
-
Garcia-Villamisar D, Dattilo J. Executive functioning in people with obsessive-compulsive personality traits: evidence of modest impairment. J Pers Disord. 2015;29(3):418-30. doi: 10.1521/pedi_2013_27_101.
-
Brunell A, Buelow MT. Narcissism and performance on behavioral decision-making tasks. J Behav Decis Mak. 2017;30(1):3-14. https://doi.org/10.1002/bdm.1900.
-
Bahari S, Pour AB. Compare executive performance and working memory in individuals with low and high schizotypal personality traits. International Journal of Humanities and Cultural Studies. 2015;2(3):1237-1247.
-
Vasiliu O. Current status of evidence for a new diagnosis: Food addiction – A literature review. Front Psychiatry. 2022;12:824936. doi: 10.3389/fpsyt.2021.824936.
-
Vasiliu O. Maintenance pharmacologic therapies for opioid use disorders: beyond opioid agonists. Romanian Journal of Military Medicine. 2019;CXXII(1):52-70.
-
Ramey T, Regier PS. Cognitive impairment in substance use disorders. CNS Spectr. 2019;24(1):102-113. doi: 10.1017/S1092852918001426.
-
Mitchell JM, Fields HL, Désposito M, Boettiger CA. Impulsive responding in alcoholics. Alcohol Clin Exp Res. 2005;29(12):2158-69. doi: 10.1097/01.alc.0000191755.63639.4a.
-
Hagen E, Erga AH, Hagen KP, Nesvag SM, McKay JR, Lundervold AJ, Walderhaug E. One-year sobriety improves satisfaction with life, executive functions and psychological distress among patients with polysubstance use disorder. J Subst Abuse Treat. 2017;76:81-87. doi: 10.1016/j.jsat.2017.01.016.
-
Conversano C, Marazziti D, Carmassi C, Baldini S, Barnabei G, DellÓsso L. Pathological gambling: a systematic review of biochemical, neuroimaging, and neuropsychological findings. Harv Rev Psychiatry. 2012;20(3):130-48. doi: 10.3109/10673229.2012.694318.
-
Vasile D, Vasiliu O. Evidence-based pharmacological strategies for gambling disorder. Psihiatru.ro. 2021;66(3):10-18.
-
Michaud A, Vainik U, Garcia-Garcia I, Dagher A. Overlapping neural endophenotypes in addiction and obesity. Front Endocrinol. 2017;8:127. https://doi.org/10.3389/fendo.2017.00127
-
Butler K, Le Foll B. Impact of substance use disorder pharmacotherapy on executive function: A narrative review. Front Psychiatry. 2019;10:98. doi: 10.3389/fpsyt.2019.00098.
-
Dominguez-Salas S, Diaz-Batanero C, Lozano-Rojas OM, Verdejo-Garcia A. Impact of general cognition and executive function deficits on addiction treatment outcomes: systematic review and discussion of neurocognitive pathways. Neurosci Biobehav Res. 2016;71:772-801. doi: 10.1016/j.neubiorev.2016.09.030.
-
Brockett AT, Pribut HJ, Vazquez D, Roesch MR. The impact of drugs of abuse on executive function: characterizing long-term changes in neural correlates following chronic drug exposure and withdrawal in rats. Learn Mem. 2018;25(9):461-473. doi: 10.1101/lm.047001.117.
-
Rezapour T, Hatami J, Farhoudian A, Noroozi A, Daneshmand R, Sofuoglu M, et al. Baseline executive functions and receiving cognitive rehabilitation can predict treatment response in people with opioid use disorder. J Subst Abuse Treat. 2021;131:108558. doi: 10.1016/j.jsat.2021.108558.
-
Vasiliu O, Marinescu I, Vasile D. Therapeutic management of substance use disorders (II). Psihiatru.ro. 2020;60(1):14-19.
-
Houben K, Wiers RW, Jansen A. Getting a grip on drinking behavior: training working memory to reduce alcohol abuse. Psychol Sci. 2011;22:968–75. 10.1177/0956797611412392.
-
Tang YY, Tang R, Posner MI. Mindfulness meditation improves emotion regulation and reduces drug abuse. Drug Alcohol Depend. 2016;163(Suppl.1):S13-8. doi: 10.1016/j.drugalcdep.2015.11.041.
-
Morgenstern J, Bates ME. Effects of executive function impairment on change processes and substance use outcomes in 12-step treatment. J Stud Alcohol. 1999;60(6):846-55. doi: 10.15288/jsa.1999.60.846.
-
McKowen JW, Isenberg BM, Carrellas NW, Zulauf CA, Ward NE, Fried RS, Wilens TE. Neuropsychological changes in patients with substance use disorder after completion of a one month intensive outpatient treatment program. Am J Addict. 2018;27(8):632-638. doi: 10.1111/ajad.12824.
-
Craig F, Margari F, Legrottaglie AR, Palumbi R, de Giambattista C, Margari L. A review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiatr Dis Treat. 2016;12:1191-202. doi: 10.2147/NDT.S104620.
-
Demetriou EA, Lampit A, Quintana DS, Naismith SL, Song YJC, Pye JE, et al. Autism spectrum disorders: a meta-analysis of executive function. Mol Psychiatry. 2018;23(5):1198-1204. doi: 10.1038/mp.2017.75.
-
Xie R, Sun X, Yang L, Guo Y. Characteristics executive dysfunction for high-functioning autism sustained to adulthood. Autism Res. 2020;13(12):2102-2121. doi: 10.1002/aur.2304.
-
Seng GJ, Tseng WL, Chiu YN, Tsai WC, Wu YY, Gau SSF. Executive functions in youths with autism spectrum disorder and their unaffected siblings. Psychol Med. 2021;51(15):2571-2580. doi: 10.1017/S0033291720001075.
-
Garon N, Smith IM, Bryson SE. Early executive dysfunction in ASD: Simple versus complex skills. Autism Res. 2018;11(2):318-330. doi: 10.1002/aur.1893.
-
Torske T, Naerland T, Bettella F, Bjella T, Malt E, Hoyland AL, et al. Autism spectrum disorder polygenic scores are associated with every day executive function in children admitted for clinical assessment. Autism Res. 2020;13(2):207-220.
-
O’Hearn K, Asato M, Ordaz S, Luna B. Neurodevelopment and executive function in autism. Dev Psychopathol. 2008;20(4):1103-32. doi: 10.1017/S0954579408000527.
-
Leung RC, Vogan VM, Powell TL, Anagnostou E, Taylor MJ. The role of executive functions in social impairment in Autism Spectrum Disorder. Child Neuropsychol. 2016;22(3):336-44. doi: 10.1080/09297049.2015.1005066.
-
Hughes C, Russell J, Robbins TW. Evidence for executive dysfunction in autism. Neuropsychologia. 1994;32(4):477-92. doi: 10.1016/0028-3932(94)90092-2.
-
Jones CRG, Simonoff E, Baird G, Pickles G, Pickles A, Marsden AJS, Tregay J, et al. The association between theory of mind, executive function, and the symptoms of autism spectrum disorder. Autism Res. 2018;11(1):95-109. doi: 10.1002/aur.1873.
-
Lynch CJ, Breeden AL, You X, Ludlum R, Gaillard WD, Kenworthy L, Vaidya CJ. Executive dysfunction in autism spectrum disorder is associated with a failure to modulate frontoparietal-insular hub architecture. Biol Psychiatry Cogn Neurosci Neuroimaging. 2017;2(6):537-545. doi: 10.1016/j.bpsc.2017.03.008.
-
Ameis SH, Blumberger DM, Croarkin PE, Mabbott DJ, Lai MC, Desarkar P, et al. Treatment of executive function deficits in autism spectrum disorder with repetitive transcranial magnetic stimulation: A double-blind, sham-controlled, pilot trial. Brain Stimul. 2020;13(3):539-547.
-
Miyajima M, Omiya H, Yamashita K, Miyata T, Yambe K, Matsui M, Denda K. The effects of cognitive remediation therapy using the frontal/executive program for autism spectrum disorder. Int J Psychiatry Med. 2016;51(3):223-35. doi: 10.1177/0091217416651254.
-
Zorcec T, Pop-Jordanova N. ADHD as an executive dysfunction. Prilozi. 2010;31(2):171-81.
-
Roth RM, Saykin AJ. Executive dysfunction in attention-deficit/hyperactivity disorder: cognitive and neuroimaging findings. Psychiatr Clin North Am. 2004;27(1):83-96, ix. doi: 10.1016/S0193-953X(03)00112-6.
-
Stevenson CS, Whitmont S, Bornholt L, Livesey D, Stevenson RJ. A cognitive remediation programme for adults with Attention Deficit Hyperactivity Disorder. Aust N Z J Psychiatry. 2002;36(5):610-6. doi: 10.1046/j.1440-1614.2002.01052.x.
-
Romero-Ayuso DM, Maestu F, Gonzalez-Marques J, Romo-Barrientos C, Andrade JM. Executive dysfunction in attention deficit hyperactivity disorder in childhood. Rev Neurol. 2006;42(5):265-71.
-
Rodriguez-Jimenez R, Cubillo A, Jimenez-Arriero MA, Ponce G, Aragues-Figuero M, Palomo T. Executive dysfunctions in adults with attention deficit hyperactivity disorder. Rev Neurol. 2006;43(11):678-84.
-
Brown TE. ADD/ADHD and impaired executive function in clinical practice. Curr Psychiatry Rep. 2008;10(5):407-11. doi: 10.1007/s11920-008-0065-7.
-
Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry. 2005;57(11):1336-46. doi: 10.1016/j.biopsych.2005.02.006.
-
Roberts BA, Martel MM, Nigg JT. Are these executive dysfunction subtype within ADHD? J Atten Disord. 2017;21(4):284-293. doi: 10.1177/1087054713510349.
-
Lambek R, Tannock R, Dalsgaard S, Trillingsgaard A, Damm D, Thomsen PH. Executive dysfunction in school-age children with ADHD. J Atten Disord. 2011;15(8):646-55. doi: 10.1177/1087054710370935.
-
Lawrence V, Houghton S, Douglas G, Durkin K, Whiting K, Tannock R. Executive function and ADHD: a comparison of children’s performance during neuropsychological testing and real-world activities. J Atten Disord. 2004;7(3):137-149. doi: 10.1177/108705470400700302.
-
Danielsson H, Henry L, Ronnberg J, Nilsson LG. Executive functions in individuals with intellectual disability. Res Dev Disabil. 2010;31(6):1299-304. doi: 10.1016/j.ridd.2010.07.012.
-
Rodrigues AR, Santos S, Rodrigues A, Estevens M, Sousa E. Executive profile of adults with intellectual disability and psychomotor intervention’ effects on executive functioning. Physiother Res Rep. 2019;2:1-7. doi: 10.15761/ PRR.1000122.
-
Shelton AL, Cornish KM, Kraan CM, Lozano R, Bui M, Fielding J. Executive dysfunction in female FMR1 premutation carriers. Cerebellum. 2016;15(5):565-9. doi: 10.1007/s12311-016-0782-0.
-
Yang JC, Chan SH, Khan S, Schneider A, Nanakul R, Teichholtz S, et al. Neural substrate of executive dysfunction in fragile X-associated tremor/ataxia syndrome (FXTAS): a brain potential study. Cereb Cortex. 2013;23(11):2657-66. doi: 10.1093/cercor/bhs251.

România văzută prin ochii unui psihiatru. Larg închişi
Ovidiu Alexinschi
România de suflet este un tărâm de poveste, cu un puternic filon popular şi cu tradiţii învăluite în emoţii pure, care au inspirat şi încântat generaţii întregi. ...
Tragic dimensions in the interpretation of the film Bucharest Non-Stop (I)
Simona Trifu, Silvia Dumitriu
The motivation originates in the plurality of plans for the interactions carried out between the consciousness and unconsciousness of characters in the film Bucharest Non-Stop. The topic of the film in a psychoanalytic interpretation is the phantasm, while in an existential interpretation, it is the transacti...
Implementarea unui program de activităţi socio-recreative la pacienţii internaţi cu tulburări psihice. Studiu-pilot
Alina Golea, Mohamed Amine Bensalem, Lavinia Duică
În timpul spitalizării, disconfortul şi suferinţa cauzate de tulburarea psihică, precum şi lipsa motivaţiei şi a interesului pacienţilor se pot amplifica, având ca rezultat o recuperare limitată într-...
Factori genetici în adicţii
Andrei Buciuta, Horia George Coman
Adicţiile reprezintă o problemă de sănătate publică la nivel mondial. Empiric, dar şi prin studii de heritabilitate, a fost demonstrată existenţa unui factor de risc genetic în dezvoltarea şi menţinerea adicţiilor şi a comportamentului adictiv. Deşi progresele ştiinţifice din ultimii ani sunt importante, impl...
Litiul – o opţiune terapeutică necesară în tulburările afective
Alexandra Boloș, Ovidiu Alexinschi
Tulburarea afectivă bipolară (TAB) afectează 1 din 100 de persoane în întreaga lume, cu un risc suicidar de 10 până la de 20 de ori mai mare în cazul persoanelor netratate, comparativ cu populaţia generală. Un demers terapeutic eficient în tulburarea afectivă bipolară depinde de o explorare clinică şi anamnes...