Managementul terapeutic al simptomelor non-cognitive ale demenţei
The therapeutic management of non-cognitive symptoms of dementia
Abstract
It is estimated that, with the increase of the life expectancy of the population, one in two people at the age of 85 years old will have a form of dementia. This will represent a real burden for medical systems, and an increasing responsibility for their families and for society. The behavioral and psychological symptoms of dementia continue to receive insufficient attention. These symptoms can be observed some years before an adequate diagnosis of dementia, and they can be the first signs of alarm before the development of specific cognitive pathology. Patients suffering from dementia can benefit from integrated medical services, specialized care at home or at the hospital, day care services, specialized health services, memory assessment services, psychological and home care therapies, together with a specific drug therapy. Taking into account all of these aspects presented above, the aim of the paper is to analyze if an earlier diagnosis of dementia can be done in clinical practice, because the initiation of earlier treatment, in the mild-to-moderate phase, can lead to a considerable improvement of cognitive functions. In this context, as dementia is diagnosed earlier, an appropriate treatment can also improve the behavioral symptomatology. Also, a multidisciplinary approach can be of real help in assessing, anticipating and managing all these issues.Keywords
dementianon-cognitive symptomstreatmentRezumat
Se estimează că, odată cu creşterea speranţei de viaţă a populaţiei, una din două persoane cu vârsta de peste 85 de ani va fi diagnosticată cu o formă de demenţă. Aceasta va reprezenta o povară reală pentru sistemul de sănătate şi o responsabilitate crescândă pentru familiile acestor pacienţi, precum şi pentru societate. Simptomele comportamentale şi psihologice ale demenţei continuă să aibă de suferit din cauza atenţiei insuficiente. Aceste simptome pot fi observate cu câţiva ani înainte de diagnosticul specific de demenţă şi pot fi primele semne de alarmă înainte de dezvoltarea unei patologii cognitive specifice. Pacienţii diagnosticaţi cu demenţă pot beneficia de servicii medicale integrate, asistenţă specializată la domiciliu sau în spital, servicii de îngrijire de zi, servicii de sănătate specializate, servicii de evaluare a memoriei, de terapii psihologice şi de îngrijire la domiciliu, împreună cu o terapie medicamentoasă specifică. Având în vedere toate aceste aspecte amintite, scopul lucrării este de a analiza dacă un diagnostic precoce al demenţei poate fi realizat în practica clinică, deoarece iniţierea unui tratament cât mai precoce, în faza uşoară până la moderată, poate conduce la o îmbunătăţire considerabilă a funcţiilor cognitive. În acest context, deoarece demenţa este diagnosticată mai devreme, un tratament adecvat poate îmbunătăţi simptomatologia comportamentală. De asemenea, o abordare multidisciplinară poate fi de un real ajutor în evaluarea, anticiparea şi gestionarea tuturor acestor probleme.Cuvinte Cheie
demenţăsimptome non-cognitivetratamentDementia – and, in particular, dementia in Alzheimer’s disease – is one of the major problems of current medicine due to its increasing incidence and its chronic evolution, with major socioeconomic consequences. In most developed countries, with a suitable network of community psychiatry, the care system of patients diagnosed with dementia has changed radically. Thus, social services networks have been developed that respond to the needs of patients and their families, for the various stages of the disease, ensuring a continuity of the medical care(1). Unfortunately, in Romania, there is not such a conception regarding the continuity of assessment and care of the person diagnosed with dementia and of the family, thus consequently the diagnosis and the therapy are initiated late and the long-term follow-up is poor. Also, in clinical practice, both in our country and in other countries, physicians are confronted with the problem of early diagnosis of dementia, which is often carried out in the final stage of the evolution of the disorder, usually in the moderate or severe form. However, it is known that the condition had the onset with at least 10 to 15 years before the first clear clinical signs of dementia(2,3).
The behavioral and psychological symptoms of dementia continue to receive insufficient attention. These symptoms can be observed two or three years before a proper diagnosis of dementia, and can be the first signs of alarm before the development of specific cognitive pathology. However, in many cases, the morose behavior of the elderly persons is considered to be normal by the relatives. Thus, beyond a behavior manifested by agitation or apathy, aggression and distrust, it often hides the clinical picture of an undiagnosed dementia. These symptoms may also be related to other mental disorders such as depression, mild cognitive impairment or pain. Often, these manifestations are the reason for hospitalization of the patients with dementia in care centers, and with their detachment from the familiar environment, aggression, distrust and helplessness increase in intensity(4,5).
In this context, as dementia is diagnosed earlier, the earlier setting up of an appropriate treatment can also improve behavioral symptomatology. A multidisciplinary approach can be of real help in assessing, anticipating and managing all of these issues. Also, it is recommended to include in this team, for example, specialists in the fields of geriatrics or clinical psychology(6).
The purpose of this study is to analyze the clinical and therapeutic approaches of a lot of 763 patients hospitalized in a continuous care system during the year 2017 in the Socola Institute of Psychiatry from Iaşi.
Materials and method
In order to carry out a quantitative and a qualitative analysis of patients with the diagnosis of dementia who are admitted for continuous hospitalization in the Socola Institute of Psychiatry Iaşi, a descriptive retrospective study was conducted, in which we used as sources of information: the centralization of patients with diagnosis of dementia discharge from the hospital in the period 1.01-31.12.2017, statistics of dementia diagnoses on staging rates, within the analyzed timeframe, the prevalence of patients with the diagnosis of dementia in relation to the total number of patients discharged during this period.
The inclusion criterion of the patients in the study group was the main diagnosis of dementia, according to the WHO ICD-10 criteria. Of the 13,832 patients discharged from the Socola Institute of Psychiatry Iaşi, from 1.01 to 31.12. 2017, we found a number of 763 patients with the diagnosis of dementia, according to ICD-10 criteria(7).
Results and discusion
Of a total of 763 patients diagnosed with dementia, 339 patients have dementia in Alzheimer’s disease, and 424 patients have the main diagnosis of mixed dementia. Mixed dementia was found to be more common, with regard to the relationship between dementia in Alzheimer’s disease and vascular lesions: 56% mixed dementia and 44% dementia in Alzheimer’s disease.
Depending on the staging of the disease, the configuration of the studied group of patients was as follows: mild form – 39.3%; moderate form – 50.4%; severe form – 10.3%.
Most of the patients had a moderate form of dementia, with frequent behavioral manifestations and care difficulties, with psychomotor agitation and aggression, instinct disorders, confusing states or leaving home. In general, patients with the moderate-severe form of dementia have a reduced compliance to treatment, being great healthcare consumers. Thus, we found the example of a patient diagnosed with mixed dementia, with moderate form (MMSE =14), who in the first six months of the analyzed period presented 11 psychiatric admissions for psychomotor agitation states with aggressive manifestations caused by behavioral symptoms in the context of the total non-compliance to medication and an inadequate socio-familial support.
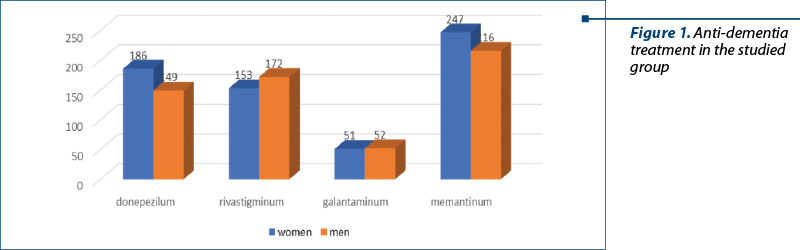
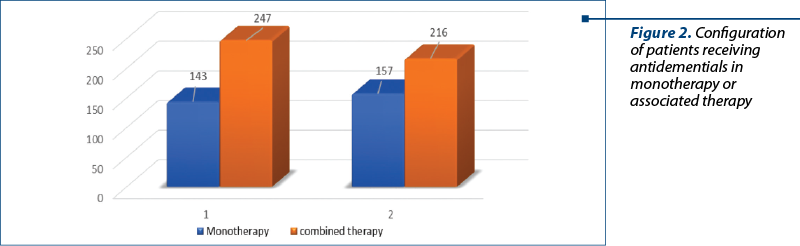
All patients included in the study group received anti-dementia treatment. The prescriptions were monotherapy with acetylcholinesterase inhibitors or their associations with memantine (Figure 1 and Figure 2).
Benzodiazepines have been used to reduce anxiety, as well as to induce sleep for short periods (2-6 weeks) to avoid addiction. It has also been clinically found in some patients that the use of benzodiazepines may have a paradoxical effect of increasing anxiety and psychomotor agitation or the occurrence of confusional states; it is possible to produce disturbances of balance, risk of hammering or producing different fractures, which leads to a decrease in the quality of their lives. Lorazepamum and clonazepamum were used with predilection in 449 patients and they were well tolereted; alprazolamum was used in 267 patiens, and bromazepamum in 120 patients.
All patients in the analyzed group received additional preparations like vasodilators and cerebral trophies represented by vinpocetin, nicergoline, ginko biloba, cerebrolisyn, actovegin, and group B vitamins.
In the studied group of patients with dementia, we found that 271 women and 305 men had been admitted in the hospital due to a symptomatology represented by psychomotor agitation with or without aggressive manifestations. In general, the state of psychomotor agitation and aggressive manifestations of dementia occur when there are changes in the personal space, in the normal daily schedule, when they are tired, when they think that their goods have been stolen, when the caregiver forces them to do an activity they do not like it, when there are complex visual or auditory hallucinations, as well as delusional ideas. In the case of agitation and/or aggressive behavior, the caregiver’s attitude and early intervention are essential.
Non-pharmacological interventions have the role to prevent or reduce the duration and the intensity of the episode, so that the effects of the pharmacological medication administered can be seen. Thus, the first gesture to be done is to secure the patient, to prevent kicks, fractures, cuts, and to avoid entrapment. Direct approach without threats gives the best results. The attitude, gestures and voice of the therapist must be calm and secure. The controversy is to be avoided and the patient’s distraction from the situation that triggered the crisis will be used. If these methods do not result in diminishing the agitation state or patient compliance with pharmacological treatment, the mechanical contention for therapeutic purposes may be applied, according with the law, as a last resort. As an alternative to this method during the hospitalization it would be the atraumatic room.
In the analyzed group, we found a total of 7 women and 12 men who needed this procedure, from a total number of 271 women and 305 men, who presented psychomotor agitation during or at the moment of admission to the hospital.
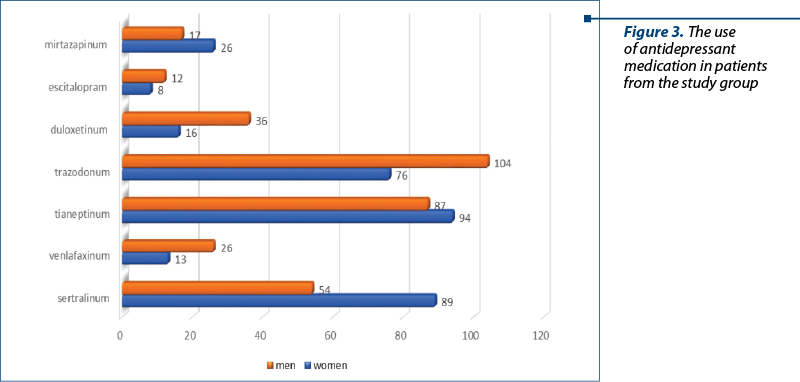
Non-cognitive manifestations of dementia are mainly represented by depression, psychotic symptoms and behavioral manifestations. They appear in more than 50% of patients with dementia, representing a major cause of consumption of medical services. Geriatric depression is a risk factor for dementia and is difficult to diagnose because there are frequent similarities between depressive symptoms and dementia symptoms. In the study, we found that 658 patients – 322 women (49%) and 336 men (51%) – received antidepressant medication. The main antidepressant used was trazodonum at doses of 100-150 mg/day in 180 patients (27.3%). This is the antidepressant of choice used in third-age patients, when depression is associated with anxiety, insomnia or aggression. Tianeptine was the second antidepressant encountered as frequency in the patients of the study, in 181 patients (27.5%). The neuroplasticity effect of tianeptin is known, which brings additional benefit to the deteriorating symptomatology. It is an anxiolytic antidepressant, without hepatic metabolism, well-tolerated at the cardiac level and effective in geriatric depression. Doses between 12.5 and 37.5 mg per day were administered in two or three times a day. The next antidepressant used in the patients from the study group was sertraline, in 143 patients (21.7%). This is part of the group of serotonin reuptake inhibitors (SSRIs), which, along with escitalopram, are considered first-line antidepressants in third-age patients (Figure 3).
An important goal in the treatment of depression in these patients was the preservation of cognitive function, a field in which SSRI antidepressants have shown superiority. Following a first depressive episode, it is recommended to continue and monitor treatment for at least six months with the same antidepressant and at the same dose that achieved the best therapeutic response in the acute phase.
Cognitive dysfunctions, somatic and psychiatric comorbidities are risk factors for the development of therapeutic resistance in geriatric depression, which is met in approximately 30% of cases. In these situations, the combinations of SSRIs with mood stabilizers, such as carbamazepine, sodium valproate and gabapentin, are recommended. These drug associations also have the effect of alleviating aggression, agitation or hypersensitivity. Thus, in the study group, 197 patients (97 women and 100 men) benefited from this treatment.
The psychotic disorders are frequently encountered in the development of dementia, especially in moderate and severe stages. The highest incidence presents the visual and auditory hallucination, as well as the delusion of persecution. In these situations, it is necessary to use an antipsychotic treatment. Haloperidol has been used in a relatively small number of patients (30 patients) due to its side effects, especially extrapyramidal and cardiovascular. Although it improves hostility, suspicion, aggression and psychomotor agitation, these frequent occurrences of neurological side effects in these patients limit the duration and dosing of this treatment. Among the atypical antipsychotics, risperidone was administered at doses of 0.5-2 mg/day in 30 patients (4.55%) and quetiapineXR at doses of 50 mg/day to 200 mg/day in 13 patients (1.97%). The most commonly used neuroleptic in the trial group was tiapridal at doses of 100-200 mg/day (125 patients; 18.9%). It should be used with caution, due to neurological side effects, as well as important orthostatic hypotension.
Conclusions
An early diagnosis and the initiation of anti-dementia therapy as soon as possible for the management of cognitive symptoms and especially behavioral disorders, that occur along the progression of dementia, has an impact on the quality of life of the patients and their families. Dementia is usually considered a health problem for the elderly, but for a number of patients, the diagnosis of dementia can be sustained much earlier. Patients with an early onset of dementia have a faster evolution, with a generalization of cognitive deficits associated with affective and behavioral symptoms, compared to patients with late onset, but also with social consequences, and their quality of life is much more important(8,9).
The emergence and unfavorable evolution of multiple affective and behavioral symptoms contributes to significant increases in direct and indirect costs associated with dementia treatment. Moreover, normal functioning deteriorates and the quality of life decreases more dramatically for both the patient and the caregiver. As the symptoms of the illness increase, these symptoms contribute to the exhaustion of the caregiver and frequently lead to the institutionalization of the patient(10). From this point of view, the effective treatment of emotional and behavioral symptoms has a potential role to reduce the personal, social and economic burden caused by dementia.
Bibliografie
- Hokama M, Oka S, Leon J, et al. Altered expression of diabetes-related genes in Alzheimer’s disease brains: the Hisayama study. Cereb Cortex. 2013; 24 (9): 2476-88.
- Ferreira-Vieira T, et al. Alzheimer’s disease: targeting the cholinergic system. Curr Neuropharmacol. 2016; 14:101-115.
- Băjenaru O, Popescu BO, Tudose C. Ghid de diagnostic şi tratament în demenţe, Ed. Amaltea. 2013.
- Higgins P. Involving people with dementia in research. Nursing Times. 2013; 109(28):20-23.
- Huang Ch, Wahlund LO, et al. Cingulate cortex hypoperfusion predict Alzheimer’s disease in mild cognitive impairement. BMC Neurol. 2002; 2:62-68.
- Houlihan D, Buchanan J. Geriatric behavior therapy: The challenges of a changing environment. Behav Therap. 2011; 42:1-2.
- ICD-10. Clasificarea Tulburarilor Mintale şi de Comportament. Simptomatologie şi diagnostic clinic. MS 1992. Editura ALL Educational. Bucureşti, 2017.
- Denesh T, et al. Ethnopharmacological Approach for Dementia Therapy and Significance of Natural Products and Herbal Drugs. Front Aging Neuroscience. 2018; 10:3.
- Hampel H, Mesulam MM, Cuello AC, et al. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain. 2018; 7(1):1917–1933.
- Dominguez E, et al. Management of moderate to severe Alzheimer’s disease: Focus on memantine. Taiwanese J Obst Gynecol. 2017; 50:415-423.

Eficacitatea psihoterapiei în prevenţia comportamentului suicidar
Romulus-Dan Nicoară
Suicidul este o problemă globală de sănătate publică, care provoacă anual aproximativ un milion de decese la nivel mondial. Tendinţele suicidare pot fi controlate, iar riscul suicidar poate fi tratat. Psihoterapia cognitivă comportamentală (CBT) şi psihoterapia dialectică comportamentală (DBT) par să fie cele...
Model de evaluare a spiritualităţii şi rezilienţei în depresia majoră
Emilia-Cristina Popescu, Doina Cozman
La momentul actual, depresia este o importantă problemă de sănătate publică. Existând puţine date despre influenţa spiritualităţii şi rezilienţei asupra depresiei majore, se impune studierea acesteia şi pe un eşantion di...
Testarea dependenţei de internet la studenţii străini din România
Dana-Cristina Herţa, Amin Muhammad, Bogdan Nemeş, Horia Coman
Utilizarea maladaptativă a internetului la studenţi influenţează sănătatea şi funcţionarea generală a acestui grup populaţional, însă problema este insuficient cercetată şi definită în prezent. ...
Realitatea virtuală imersivă în psihoterapia anxietăţii şi reabilitarea oculară. O abordare transdisciplinară
Marcel-Alexandru Găină, Andreea Moraru, Bogdan‑Victor Ştefănescu, Alexandra-Maria Găină, Andreea Silvana Szalontay, Dănuţ Costin
Realitatea virtuală imersivă (iVR) reprezintă nu numai o intervenţie indicată de ghidurile terapeutice în anumite tulburări de anx...
Implementarea realităţii virtuale în tulburările cognitive, psihotice şi anxioase
Marcel Găină, Andreea Silvana Szalontay, Emil-Ionuţ Botezatu, Alexandra-Maria Găină, Cristinel Ştefănescu
În ultimele două decenii, realitatea virtuală (RV) a fost utilizată într-o varietate de contexte terapeutice. Expunerea la RV imersivă (iVR) se realizează prin căşti virtuale dedicate care, prin inter...