Din aceeași categorie

Introduction
Gynecomastia is the excessive benign development of breast glandular tissue in male patients. Physiological gynecomastia classically occurs in three age groups: newborns, adolescent boys and older men, involving hormonal changes(1).
Neonatal breast enlargement is a physiological transient response to diminished levels of maternal estrogen at the end of pregnancy, which activates the secretion of prolactin from the newborn’s hypophysis gland(2). However, it is possibly related to placental transformation of androgens to estrogens, which enter the fetal circulation and stimulate glandular breast proliferation(3).
In addition, neonatal breast enlargement is frequent and can be observed in approximately 70-80% of neonates and is independent of the sex of the infant, occurring both in males and females(2).
Breast enlargement usually develops in the first few days of life and resolve spontaneously within weeks to months, without a specific treatment. Furthermore, it is sometimes associated with a milky nipple discharge called “witch’s milk”, maintained and aggravated by squeezing the breast(4).
Continued compression of the breast without parental guidance can result in inflammation, further enlargement, persistence of hypertrophied tissue, and possible infection (mastitis or abscess)(2,5,6).
In addition, overlapping hormonal contraceptive treatment of the breastfeeding mother may play a role in the pathophysiology of breast hypertrophy in the breastfed infant.
Case report
We present the case of a 2-month-old infant referred for endocrine evaluation from the pediatric surgery service for bilateral asymmetric gynecomastia.
He was born at term, at 39 weeks of gestation, by caesarean section, after uncomplicated pregnancy, with a birth weight of 3750 g, and with 9 and 10 Apgar scores at 1 minute and 5 minutes, respectively. He is the second child of the family. He was exclusively breastfed and showed no signs of discomfort or irritability. The parents denied using creams or body oils with xeno- or phytoestrogens.
Bilateral gynecomastia was noticed by the parents since birth, but the breasts continued to grow, with significant enlargement of the left breast, with accentuation in the last two weeks, which coincided with the start of desogestrel progestogen-only pill treatment by the mother, on the recommendation of the gynecologist, after resumption of mothers’ menstruation.
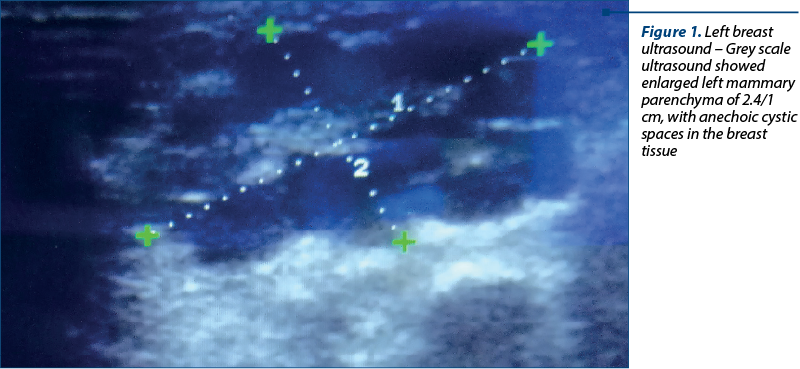
Firstly, on the presentation to the pediatric surgery department, the infant was in good clinical condition, without rash, without signs of staphylococcal skin disease and without fever. The surgeon recommended the application of a local compress with iodine solution to the left breast, until the paraclinical investigations was finished (Figure 1).
Secondly, on the clinical endocrinological exam, the infant had normal anthropometric parameters corresponding to age, with bilateral asymmetrical gynecomastia with prominence of the left breast, corresponding to Tanner stage 2b, with normally colored areolas, with no evidence of tenderness or discharge. In addition, the infant had no particular phenotypic features, with pubertal development corresponding to stage 1 Tanner, with normally conformed penis, without scrotal hyperpigmentation, without pathological pubic hair, and without café-au-lait spots.
The paraclinical examinations showed normal parameters, with normal white blood cells, WBC count = 6400/mm3 (range: 4000-10000/mm3), and normal C-reactive protein (CRP) level (CRP<0.5 mg/dL; normal range <0.5 mg/dL), with no biological inflammatory syndrome.
Hormonal evaluation showed normal gonadotropins, adrenal, testosterone, estradiol and thyroid values, but with slight hyperprolactinemia (prolactin level 20 ng/ml; normal range 4-17 ng/ml).
Ultrasound evaluation of the breasts showed bilateral retroareolar mammary glandular tissue, in the left breast with the size of 2.4/1 cm and 0.5/0.7 cm, respectively, in the right breast, without axillary adenopathy and without any ultrasound sign of mammary abscess (Figure 2).

The infant’s case was managed in a multidisciplinary team of pediatrician, surgeon and endocrinologist. Correlating clinical, paraclinical and ultrasound data, we were able to exclude the diagnosis of mastitis or breast abscess and the final diagnosis was neonatal gynecomastia, which overlapped or possibly interfered with the mother’s hormonal contraceptive treatment. Consequently, it was decided to discontinue the mother’s contraceptive medication for a period of time, to continue breastfeeding and monitor the baby without any special treatment. In addition, the parents were informed to avoid squeezing the breast and that a milky discharge might occur. The clinical evolution was favorable, with almost the complete remission of gynecomastia within six months of follow-up.
Discussion
Gynecomastia is a benign growth of male glandular breast tissue and is a common condition in the pediatric population, especially in newborns and young infants(3,7). The most common cause of gynecomastia is an imbalance between androgens and estrogens. One of the incriminated pathophysiological mechanisms is the placental transformation of dehydroepiandrosterone (from fetal and maternal sources) to estrone and estradiol which enter the fetal circulation and stimulate glandular breast enlargement(3). Furthermore, breast tissue hypertrophy is due not only to the effects of pregnancy hormones, but also to the endocrine system activity of the infant, gestational age being one of the factors in determining the normal breast tissue size(8,9). Although the presence of neonatal breast tissue is benign, its persistence and aggravation can be a source of concern(8,10).
In addition to hormonal changes in the mother and newborn, a factor that also influences the appearance and persistence of gynecomastia is the administration of hormonal treatment to the breastfeeding mother. In recent studies and in a systematic review, it has been shown that the administration of progestogen-only methods among postpartum women while breastfeeding is safe for infants, who have normal growth and development in the first years of life(11-13). It is also proven that the use of progesterone preparations does not influence milk production and it was not found any decrease in weight gain of the infant, unlike estrogenic or combined oral contraceptives which are known to decrease the amount of breast milk and produce an unsatisfactory weight gain of the infant(14-16). Even though studies show that the quantity and quality of milk are not modified, two cases of gynecomastia in infants whose mothers received desogestrel-containing progestogen-only pill have been described in literature, but without being able to establish a statistically significant link between the increased breast tissue and the desogestrel pill administration(11,15,17). In addition, the results concluded that neither the treatment with progestogen-only methods had an adverse impact on the health and development of the infants(11,15,17). However, further studies are required to study the exact mechanism by which desogestrel can be associated with breast enlargement.
Even though most cases of gynecomastia are diagnosed clinically, ultrasound plays an important role in differentiating a benign appearance from mastitis or abscess. Some authors have described the appearance of ultrasonography of neonatal mastitis as masses with mixed echotexture and internal vascularity or as poorly marginated hyperechoic breast tissue with hypervascularity(5,6,18). Mastitis can be differentiated from abscess due to the presence of increased peripheral vascular distribution that they saw around cystic breast lumps(5,6,19,20). In our case, ultrasound demonstrated bilateral retroareolar mammary glandular tissue with asymmetrical left-right dimensions, suggestive for gynecomastia.
In this case, we can consider a possible connection between the association of gynecomastia in which left breast enlargement overlapped with the initiation of desogestrel contraceptive therapy in the mother of an exclusively breastfed infant, but further studies are needed to establish the exact mechanism. Furthermore, the favorable outcome of our patient after the discontinuation of maternal hormone therapy without a specific treatment is similar to the data in the literature(2,11,17,21).
Conclusions
Breast enlargement in newborns is a common transient physiological condition that can occur in both girls and boys. It is important to distinguish newborn gynecomastia from mastitis or breast abscess. Parents should be informed that it will resolve in weeks to a few months, without treatment, and should be warned not to squeeze the breast. The most appropriate approach is to observe the breast involution. Further studies are needed to investigate the correlation between the use of progestogen (progestogen-only pill desogestrel) in breastfeeding mothers and the development of breast enlargement in breastfeeding infants.
Conflict of interests: The authors declare no conflict of interests.
ginecomastie neonatalădesogestrel