ORIGINAL STUDY
Studiul erorilor diagnostice și terapeutice corelate cu studiul markerilor tumorali cu impact în prognosticul pacienților cu cancer localizat la cap și gât
The study of diagnostic and therapeutic errors correlated with the study of tumor markers with impact in the prognosis of patients with head and neck cancer
Abstract
Introduction. Choosing a treatment protocol for patients with carcinomas of the head and neck in locally advanced stages of the disease remains an open question. Growing incidence and mortality imposed an analysis of the administered treatment efficacy, of the causes of therapeutical failures, and the impact of the expression of tumor markers in the prognosis of patients. Materials and methods. The retrospective study was conducted in the Medical Oncology Clinic of the Emergency County Hospital of Craiova, Romania, during the period January 2000 - December 2008, patients included in the analytical study being randomized balanced, in two arms (270 patients treated with radiotherapy vs. 254 patients treated with concurrent or alternative radiochemotherapy). The morphopathological study was conducted on 93 pieces of biopsy selected mainly from patients who were recorded as failures. Results and discussions. A correct clinical and imaging diagnosis could avoid the understaging of the neoplastic disease and practicing surgery as a first therapeutic gesture in advanced stages, therapeutic error responsible for most therapeutic failures. Clinical factors with predictive value in terms of prognosis and therapeutic response rate in terms of the rate of overall survival and disease-free interval are disease stage, tumor location and the treatment administered. Concurrent radiochemotherapy reduces post-treatment relapse rate, and assuring the local control of the disease remains the objective of hyperfractionated radiotherapy. Factors with imunohistological and prognostic value are histopathological type, tumor differentiation degree, expression of tumor markers, respectively such as EGFR expression and p53 and Ki67 nuclear imunomarking. The detection of clinical, immunohistochemical and prognostic factors creates an expectation of fair therapeutic randomization based on histopathological and immunohistochemical analysis. The group with poor prognosis that requires the association of Erbitux to radiation therapy includes patients diagnosed with squamous cell carcinoma, poorly differentiated of the hypopharynx and larynx, locally advanced with membrane overexpression for EGFR, nuclear imunomarking for p53 >55% of tumor cells and nuclear immunomarking for Ki67 >55% of tumor cells.Keywords
head and neck cancerdiagnostic and therapeutic errostreatmenttumor markersprognosisRezumat
Introducere. Alegerea protocolului de tratament pentru pacienții cu carcinoame ale sferei ORL stadii avansate locoregional, rămâne o discuție deschisă. Incidența și mortalitatea în continuă creștere au impus analiza eficacității tratamentului administrat, a cauzelor eșecurilor terapeutice, precum și a impactului expresiei markerilor tumorali în prognosticul pacienților. Materiale și metode. Studiul retrospectiv a fost realizat în Clinica de Oncologie a Spitalului Clinic Județean de Urgență din Craiova, România, în perioada ianuarie 2000 - decembrie 2008, pacienții incluși în studiul analitic fiind randomizați echilibrat, în două brațe terapeutice (270 de pacienți radiotratați vs. 254 de pacienți radio-chimio-tratați). Studiul morfopatologic a fost efectuat pe 93 de piese de biopsie selectate cu precădere din grupul pacienților la care au fost înregistrate eșecuri terapeutice. Rezultate și discuții. Un diagnostic clinico-imagistic corect ar putea evita substadializările bolii neoplazice, cu practicarea intervenției chirurgicale ca prim gest terapeutic în stadiile avansate, eroare terapeutică responsabilă de majoritatea eșecurilor terapeutice. Factorii clinici cu valoare predictivă în termenii ratei de răspuns terapeutic și prognostică în termenii ratei de supraviețuire globală și a intervalului liber de boală sunt stadiul bolii, localizarea tumorală și tratamentul administrat. Radio-chimio-terapia concomitentă reduce rata recidivelor post-terapeutice, iar asigurarea controlului locoregional al bolii rămâne obiectivul radioterapiei hiperfracționate. Factorii cu valoare imuno-histo-prognostică sunt tipul histopatologic, gradul de diferențiere tumorală, expresia markerilor tumorali, respectiv imunomarcajul membranar pentru EGFR și imunomarcajul nuclear pentru p53 și Ki67. Decelarea factorilor clinico-imuno-histo-prognostici creează premisa unei randomizări terapeutice corecte bazată pe analiza buletinelor histopatologice şi imuno-histochimice. Grupa cu prognostic nefavorabil la care se impune asocierea Erbitux la radioterapie include pacienți diagnosticați cu carcinoame scuamoase slab diferențiate ale hipofaringelui și laringelui, stadii avansate locoregional, cu hiperexpresie membranară pentru EGFR, imunomarcaj nuclear pentru p53>55% din celulele tumorale și imunomarcaj nuclear pentru p Ki67>55% din celulele tumorale.Cuvinte Cheie
cancer al sferei cap și gâterori de diagnostic și terapeuticetratamentmarkeri tumoraliprognosticIntroduction
Head and neck cancers represent 10-15% of all cancers and cause 4-5% of all deaths from cancer. Annually, worldwide, approximately 650,000 patients are diagnosed with head and neck cancers, and 350,000 patients die from this disease(1-4).Growing incidence and mortality of head and neck malignancies imposed therapeutic outcomes analysis, detecting the causes of post-therapeutic failures, and the study of genetical and molecular changes impacting the prognosis(1-4).
Materials and method
Statistical data necessary for processing sheets were collected from ONC1 initial declaration files, from ONC2 sheets of evolution and ONC3 death records present in the archives of the Medical Oncology Clinic of Craiova and Medical Oncology Cabinet County Craiova.The overall incidence of head and neck cancers in Dolj county was 3.23‰ (524/17916), with an annual average of 20 cases, but an exponential increase in the number of patients registered for all neoplastic locations, during the study period.
Most patients included in the study were men (463 men/61 women, index ratio 7.59/1), elderly (median age 51.7 +/- 13.46 years), with provenance from the country side - rural/urban ratio: 1.81 (338/186 patients) -, dragged (chronic alcoholism, chronic smoking), but with acceptable performance status: 0-1 IP: 463 patients (88.35%) vs. IP 2: 61 patients (11.65%).
Most patients had carcinoma of the hypopharynx (210 patients; 40.07%) and larynx (195 patients; 37.21%) vs. oropharynx carcinoma (85 patients; 16.22%) and nasopharynx (34 patients; 6.48%). In the endoscopic confirmation of malignancy, it was detected the predominance of squamous carcinomas, moderately or poorly differentiated, characterized by marked tumor aggressiveness (493 patients; 94.08%). Patients randomized in the study presented as a whole and for each tumor location, locally advanced disease - stage III and IVA, B, respectively, clinical category T3 + T4 N1-3: 445 patients (84.92%) vs. stages I and II with clinical category correspondent T1 + T2 N0: 79 patients (15.07%). Localized disease stages were the prerogative of nasopharynx carcinoma (9/34 patients, 26%), carcinoma of the oropharynx and palatine tonsil more precisely (19/85 patients, 22.35%) and of the larynx glottis carcinomas (51/195 patients; 26.15%).
The primary objective of the study was to identify the most common errors in diagnosis and treatment responsible for therapeutic failures and detecting in this group of patients the expression of tumor markers that enable a correct therapeutic strategy after histopathological and immunohistochemical analysis.
Diagnostic errors
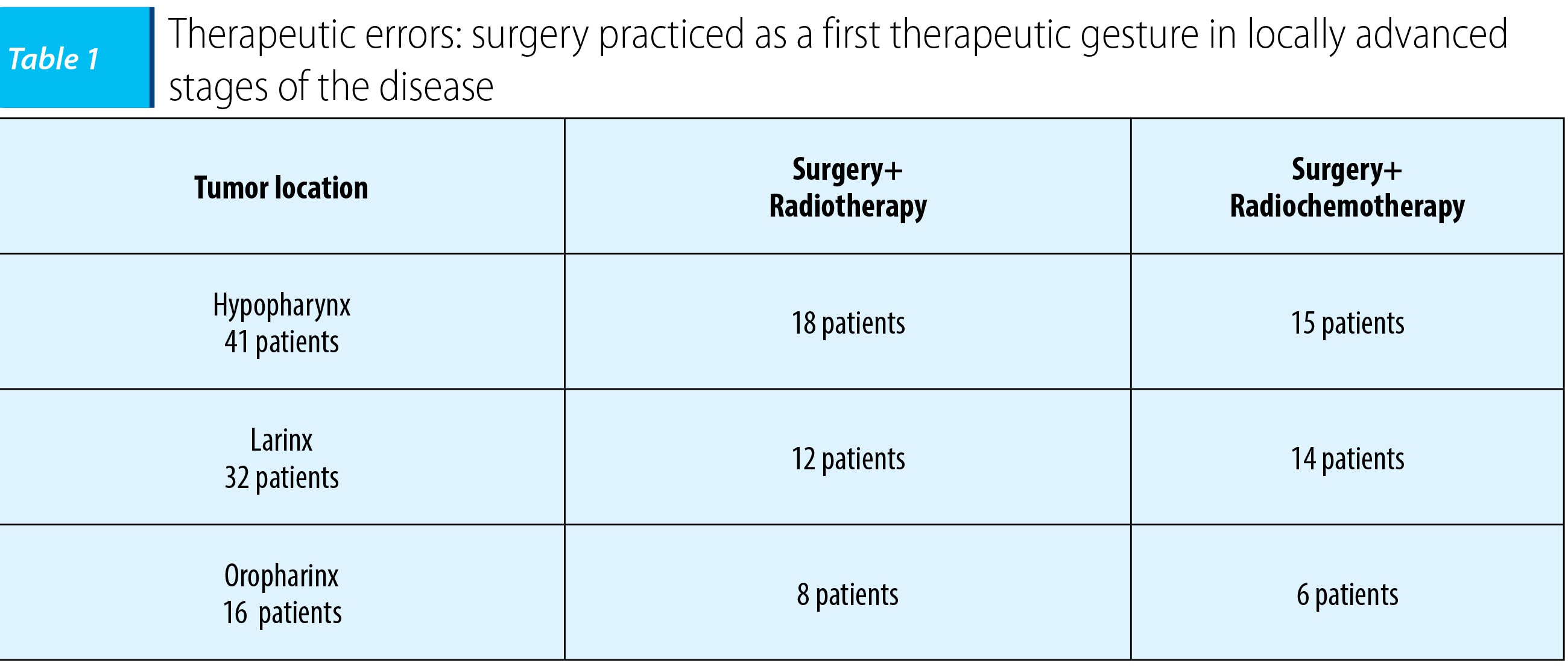
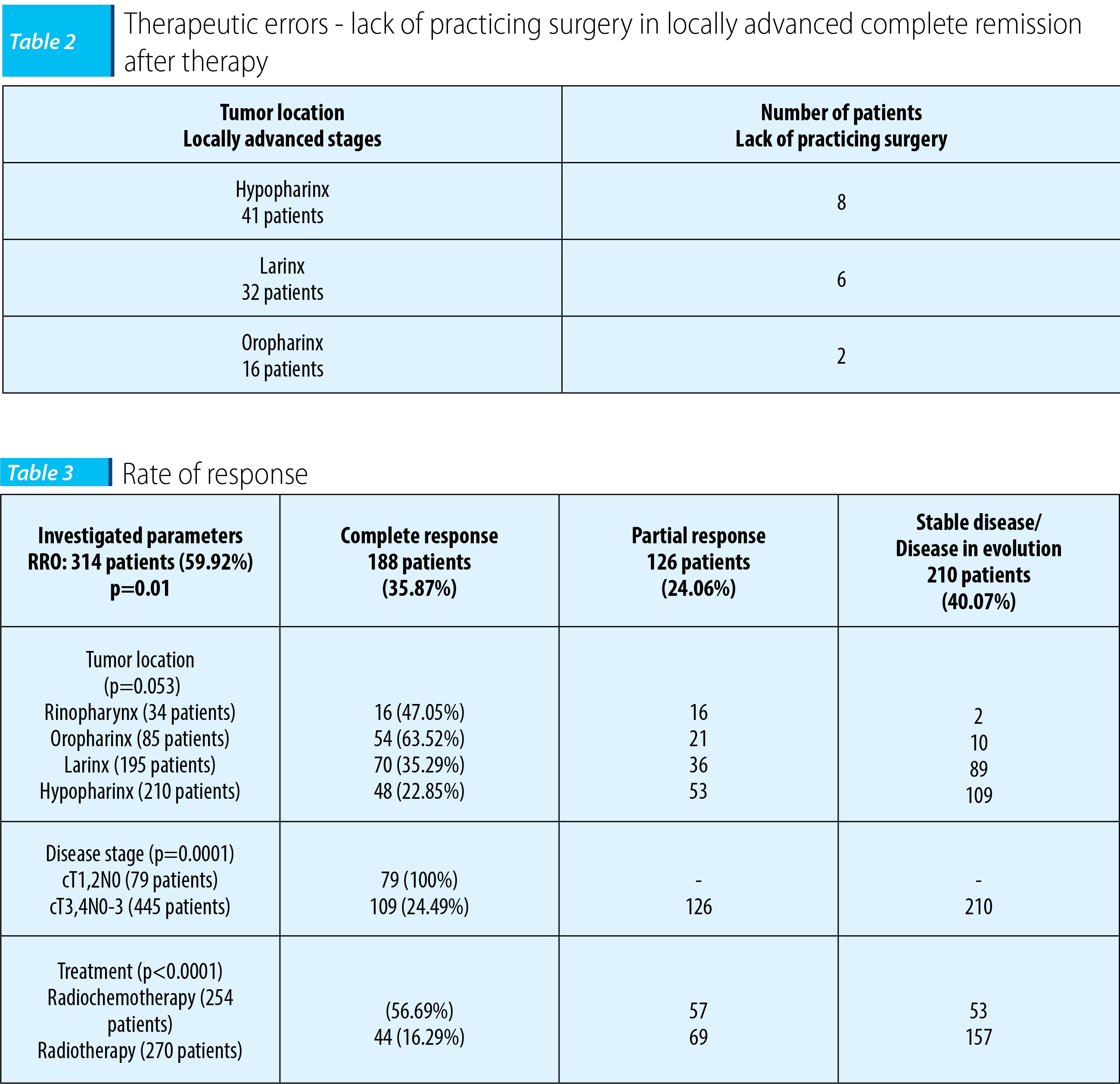
An error was practicing surgery as a first therapeutic gesture, that has been found in patients diagnosed with carcinoma of the oropharynx, hypopharynx and larynx with initial presentation to ENT clinics; after radical surgery, based on histopathological analysis bulletins, the patients were classified in stages III (pT3N1-3) or IVA, B (pT4N1-3) of the disease. Patients were randomized balanced in the two treatment arms, radiotherapy vs. radiochemotherapy, but all patients had therapeutic failures explained by an increased risk of distant dissemination, as a result of the practice of surgery as a first therapeutic gesture in locally advanced disease with lymphatic spread already present.Another therapeutic error was reported in 16 patients with carcinoma of the oropharynx, larynx and hypopharynx (stage III cT3N0/1), which showed complete remission post-radiochemotherapy. Clinical and imaging lack of appreciation of reconversion to operability in the oncologic control and therefore lack of practicing surgery or irradiation dose supplementation were responsible for therapeutic failures in the further evolution of these patients.
In the comparative analysis of the therapeutic results, there were 524 patients included, clinically and radiologically diagnosed and histologically confirmed with carcinoma of the hypopharynx, larynx, oropharynx and nasopharynx at any stage of the disease, except metastatic disease (stage IVC), who were randomized balanced for all lots and all neoplastic locations into two therapeutic groups:
- Group A included 254 patients treated using radiochemotherapy according to standard protocols: concurrent radiochemotherapy with cisplatin 20 mg/m²/day PIV CI x 5 days/4 weeks or 40 mg/m PIV CI/weekly or alternative radiochemotherapy using the regimen: 5-FU 1000 mg/m²/day i.v. day 1-4 CI + cisplatin 20 mg/m²/day i.v. on day 1/4 weeks.
- Group B included 270 patients treated with Theratron 75, energy Mv 1.25 (range 2000-2006) or Varian linear accelerator with 6 MV energy (2007-2008); the total dose was 68-72 Gy/primary tumor (1.8-2 Gy / fraction, 5 days/week) and 40 Gy/laterocervical region (2 Gy/fraction, 5 days/week).
The disease-free interval
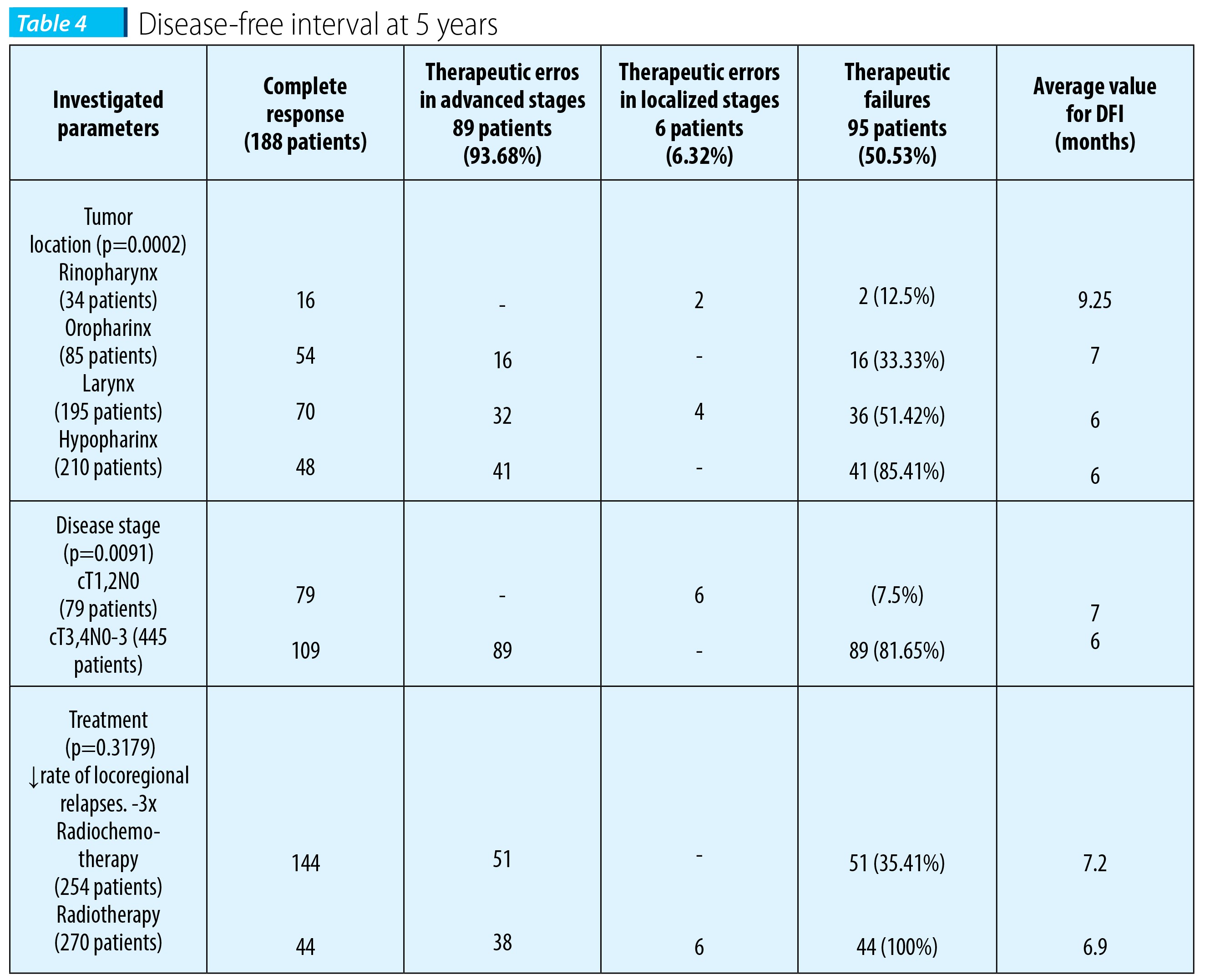
Patients who experienced complete remission and were recorded as failures benefited from reirradiation (according to TD administered initially and irradiated volume), salvage surgery (lymphadenectomy) or second-line palliative polychemotherapy for patients with locoregional evolving disease based on regimens with taxane (Paclitaxel/Docetaxel) and platinum (cisplatin/carboplatin) or first line palliative polychemotherapy for patients with locoregional or distant recurrences, 5FU + cisplatin regimen.Thus, from a total of 188 patients (35.87%) with complete remission post-treatment, 95 patients (50.53%) experienced treatment failure after a median disease-free interval of 7 months. Most treatment failures were recorded as evolutionary locoregional disease, the consequence of therapeutic errors or of practicing surgery as a first gesture in advanced locoregional disease (73 patients; 76.84%), or lack of practicing surgery or irradiation dose supplementation in stage III with reconvertion to operability (16 patients; 16.84%). A small percentage of treatment failures were recorded as resuming locoregional evolution of the disease and is the consequence of diagnostic errors, with understaging of the disease, lack of advanced imaging and therapeutic practice of surgery as a first gesture (6 patients; (6.32%).
In patients receiving radiochemotherapy, from the 144 patients who had complete remission, 51 patients (68.62%) with carcinoma of the hypopharynx, larynx and oropharynx advanced locoregional experienced failures. In 35 patients who achieved therapeutic failures in terms of continuing the locoregional evolution of the disease, surgery was practiced as a first therapeutic gesture. 16 patients (31.37%) with treatment failures recorded in terms of resuming locoregional evolution of the disease after complete remission the therapeutical errors consisted in the lack of practicing surgery or at least supplementing the dose of irradiation. This aggressive development in terms of achieving complete remission after primary therapy raised the issue of performing immunohistochemical staining in order to detect molecular markers with prognostic value.
In the case of radiotreted patients, the 44 patients who experienced complete remission, therapeutic failures were the result of errors in diagnosis and treatment, being registered at a rate of 100%. Continuing the evolution of the disease in 38 patients with carcinoma of the hypopharynx, larynx and oropharynx in locally advanced stages was due to therapeutic errors, with the practice of surgery as the first therapeutic gesture. Resumption of locoregional evolution of the disease in 6 patients (4 patients with carcinoma of the larynx glottis and 2 patients with carcinoma of the nasopharynx) was consequently to diagnostic errors or failure to comply with therapeutic protocols or understaging.
On multivariate statistical analysis of the disease-free intervals, based on the tumor location and stage of disease, the threshold of statistical significance was achieved (p=0.0002, p=0.0091), demonstrating the prognostic value of tumor location and stage of the disease in terms of interval free of disease. In multivariate analysis of disease-free interval depending on the therapy administered, threshold did not reach statistical significance (p=0.3179); the failures were recorded in both arms after a median disease-free interval of 7 months, but with a rate of 3 times lower (35.41%) in patients receiving radiochemotherapy. Radiosensitising chemotherapeutic agents have a major role in increasing the effectiveness of radiotherapy and consequently the rate of therapeutic response, and improving locoregional disease control remains the objective of hyperfractionated radiotherapy.
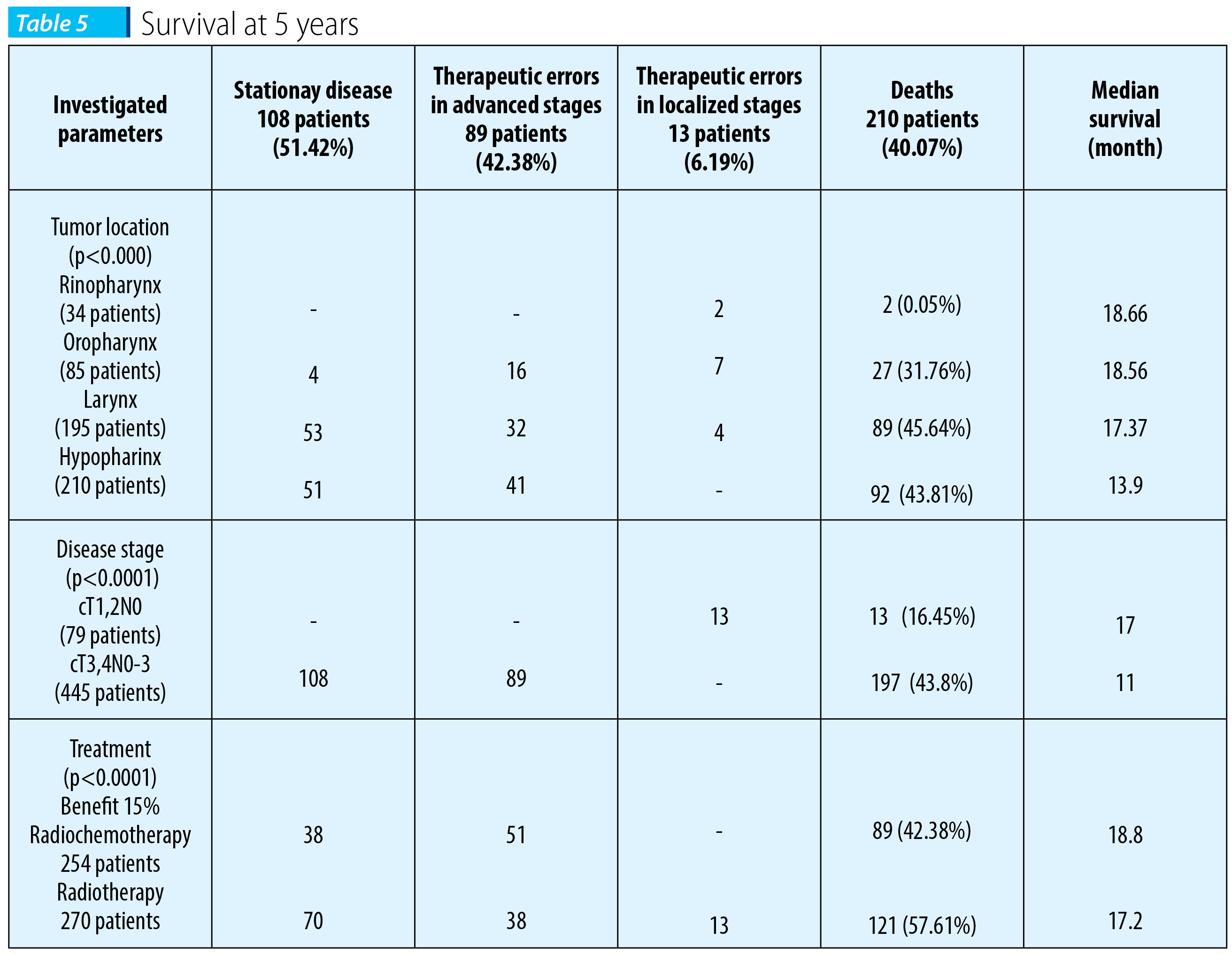
Another objective of the trial was to analyze the survival rate at 5 years, being registered a 40.07% cancer mortality (210 deaths), with a median survival of 19 months.
On multivariate statistical analysis based on the location of neoplastic disease stage and treatment administered, the results reached statistical significance (p<0.0001, p<0.0001, respectively p<0.0001), demonstrating the prognostic value of the parameters studied, in terms of the rate of survival at 5 years.
Concurrent chemoradiotherapy or alternative demonstrated a statistically significant benefit in terms of survival at 5 years (median survival 18.8 months vs. 17.2 months, with a benefit of 15%, p<0.0001).
Our results are consistent with the results of meta-analysis of 87 randomized trials that included 16.640 patients, which demonstrated that concomitant radiochemotherapy leads to an 8% benefit for overall survival at 5 years, p <0.0001.
Multivariate analysis has detected the factors with predictive value in terms of response rate and factors with prognostic value in terms of survival rate at 5 years and the disease-free interval at 5 years, being the tumor location, disease stage and the treatment given. In the category including patients with poor prognosis are those diagnosed with carcinoma of the hypopharynx and larynx, in advanced locoregional stages radiotreated.
Morphological study was performed in 93 patients who were evaluated in both histological and immunohistochemical aspects for molecular markers (EGFR, p53 and Ki67) which overexpressed; according to data published in scientific journals, they are correlated with a poor prognosis.
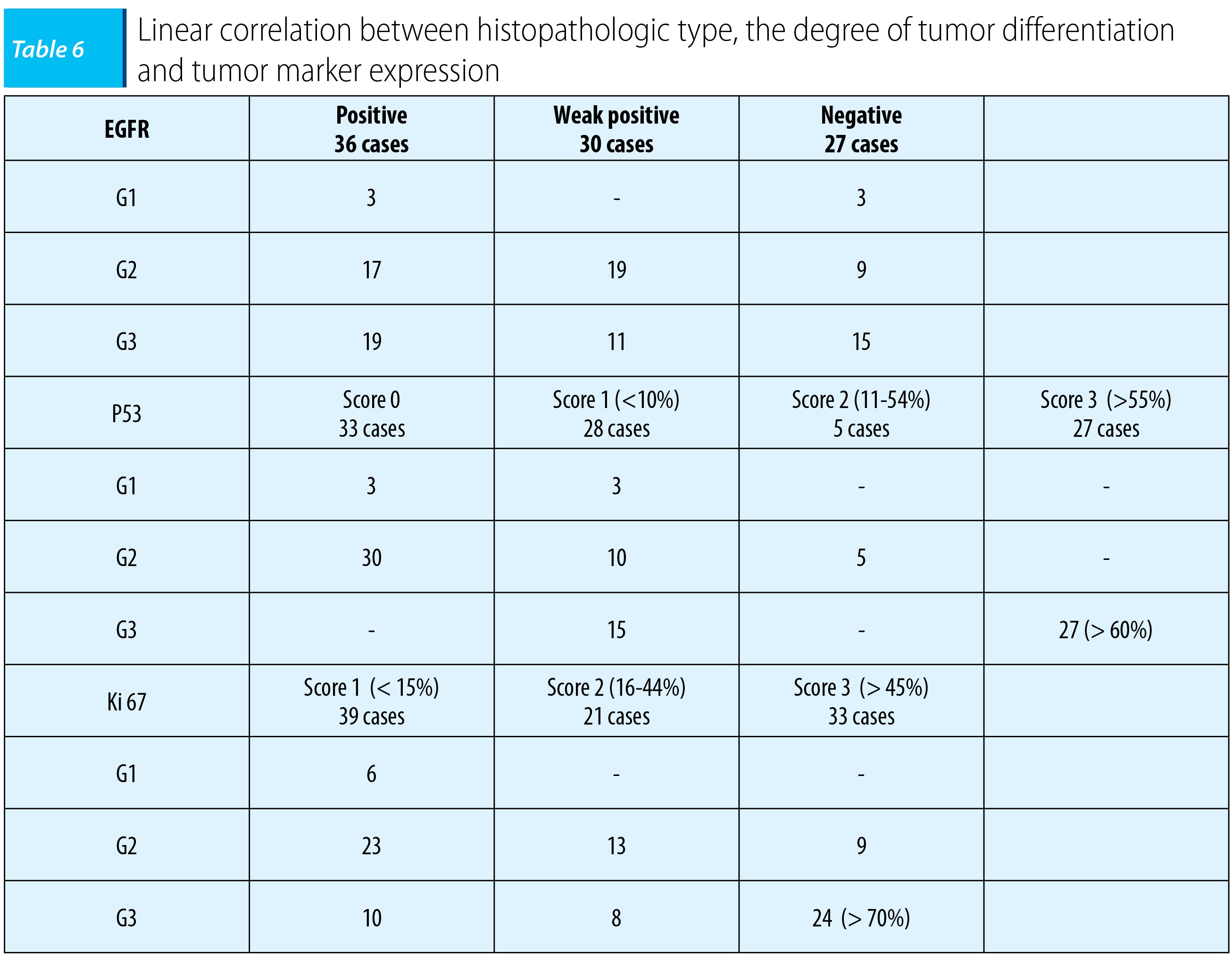
Immunoreaction for EGFR was membranous (score 0 = absence of immunomarking to tumor cells; score 1-3 = immunomarking weak positive, score ≥4 = strongly positive immunomarking). Nuclear immunomarking for proliferation index Ki67 was semiquantitative (score 1 - index ≤15%; score 2 - index of 16-44%, score 3 - index ≥45%). Nuclear immunomarking for p53 protein was semi-quantitative (score 0 = no; score 1 = nuclear immunomarking in less than or equal to 10% of tumor cells; score 2 = nuclear immunomarkingin in 11-54% of tumor cells; score 3 = immunomarking positive in at least 55% of tumor cells, and scores of 0 and 1 were considered negative for the presence of mutations in the p53 gene, and scores 2 and 3 positive for this mutation).
Immunohistochemical analysis detected linear relationship between the degree of tumor differentiation and membrane EGFR expression or p53 and Ki67 nuclear immunomarking. In epidermoid carcinomas poorly differentiated in most cases it was detected the overexpression of EGFR membrane (19/36 cases - 52%), nuclear immunomarking p53 in >55% of tumor cells (27 cases) and nuclear immunomarking Ki67 in> 45% of tumor cells (24/33 cases, 772.7250).
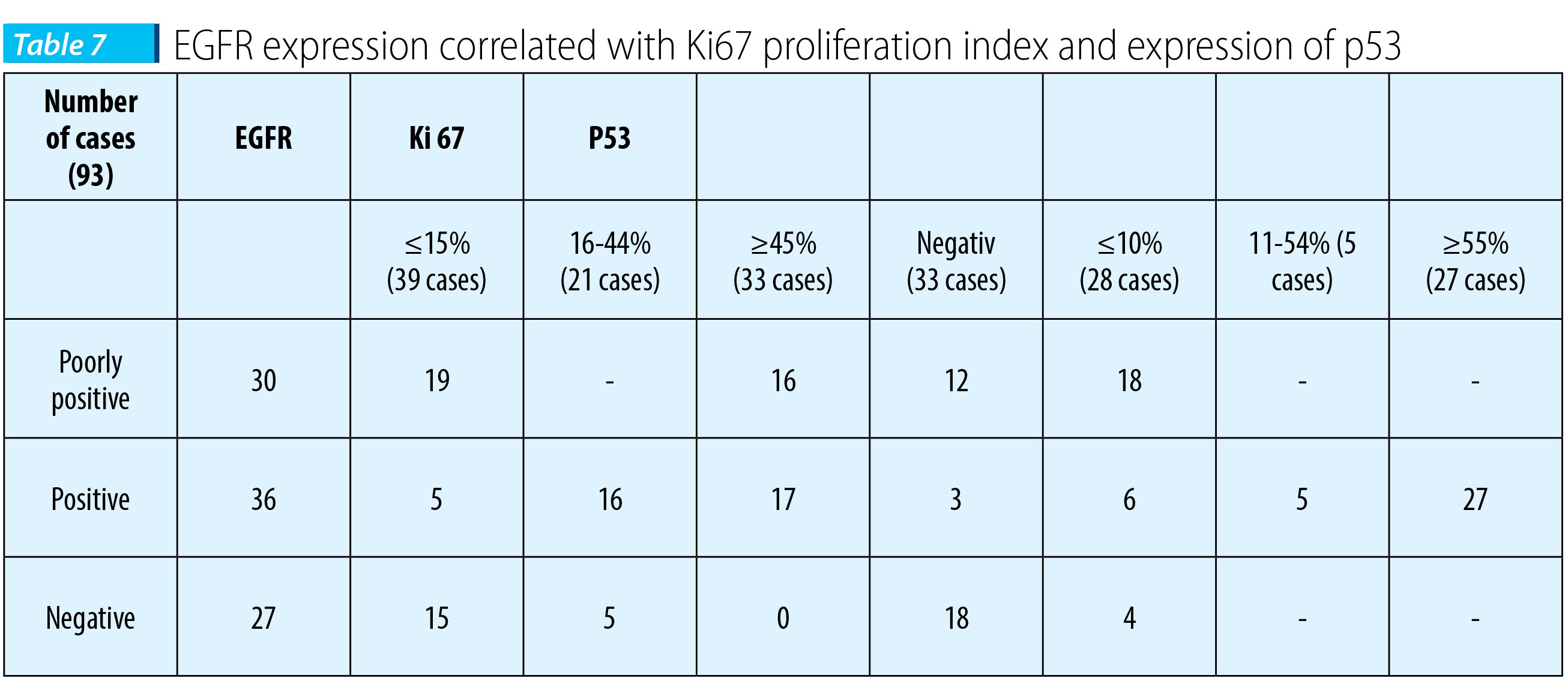
It was also noted a linear relationship between the expressions of tumor markers, carcinomas expressing intense membrane for EGFR presented an intense nuclear immunomarking for p53 (more than 55% of tumor cells) and Ki67 (more than 45%). So, patients with carcinoma who experienced a positive expression of EGFR (66 cases, 79.97%) had a Ki67 proliferation index greater than 45% (33 cases, 35, 48%) and p53 protein showed a positive nuclear immunomarking in cells in over 55% of the 27 cases (23.66%).
So, after immunohistochemical analysis we established a linear relationship between histopathologic type, degree of tumor differentiation and tumor marker expression.
The expression of molecular markers was detected immunohistochemical in patients receiving radiochemotherapy where the results reached statistical significance threshold in terms of therapeutic response rate, the overall survival and disease-free interval. The group with poor prognosis included 35 patients who were recorded as failures, with evolution of the disease, due to surgery practiced as a first therapeutic gesture in advanced stages of the disease and 16 patients with the resumption of the disease in the absence of practicing surgery after complete remission after therapy; death in this group was recorded when reporting data due to disease distant progression(23 cases of bone metastasis and 12 cases of lung metastases) and resumption of locoregional evolution of the disease (16 patients). Immunohistochemical staining detected intensely positive immunoreactions for EGFR membrane with nuclear immunomarking for p53 in a proportion of more than 55% in tumor cells and nuclear immunomarking for proliferative index Ki-67 in a proportion of more than 45% of tumor cells.
The group with intermediate prognosis included 38 patients out of 53 patients with stationary disease after radiochemotherapy, with resumption of disease progression after a median free interval of 7 months, the death being registered in reporting data by resuming locoregional evolution. Immunohistochemical stains detected weak positive immune reaction for EGFR with nuclear immunomarking for p53 in 10-55% of tumor cells and nuclear immunomarking for Ki67 in 10-45% of tumor cells.
The group with favorable prognosis included 93 patients of the 144 patients with complete remission after radiochemotherapy and who had a locoregional controlled disease when reporting the data. Immunohistochemical study due to material reasons was conducted only in 4 patients with poorly differentiated epidermoid carcinoma of the larynx. Immunohistochemical staining detected the absence of membrane expression of EGFR and p53 nuclear immunomarking was absent or present in <10% of tumor cells (0/1 score correlated with the absence of a mutant form of p53) and Ki-67 proliferative index was absent or present in <10% of tumor cells.
Following immunohistochemical study, the immunophenotypic groups could be defined as follows:
- a. favorable prognosis: absence of immunomarking for EGFR, nuclear immunomarking for p53, Ki67 absent or present in <10% of tumor cells;
- b. intermediate prognosis: immunomarking weakly positive for EGFR, p53 nuclear immunomarking in 10-55% of tumor cells and nuclear Ki67 immunomarking in 10-45% of tumor cells;
- c. unfavorable prognosis: immunomarking strongly positive for EGFR, p53 nuclear immunomarking positive in >55% of tumor cells and nuclear immunomarking Ki67 positive in >45% of tumor cells.
Discussions
Choosing the appropriate treatment remains a controversial topic, considering the poor prognosis of locoregional advanced stages with the presence of tumor formations over 3 cm in size and/or laterocervical lymph nodes metastasis, with a curability rate of 30%(5-7). According to the results of “MACH-NC meta-analysis of Chemotherapy in Head and Neck Cancer”, based on 15 randomized trials involving 2487 patients, multi-agent induction (regimes platinum + 5FU) + radio-chemotherapy vs. exclusive radiotherapy lead to a benefit of 5% in overall survival at 5 years (p=0.05)(8-17). The results of a meta-analysis of 87 RCTs that included 16,640 patients showed that concurrent radiochemotherapy with Cisplatin vs. radiotherapy alone determines an exclusive benefit of 8% in overall survival at 5 years (p<0.0001). So, multi-agent induction followed by concurrent radiochemotherapy is the standard treatment in locally advanced stages and induction polychemotherapy regimens with taxanes (especially Paclitaxel) and platinum are cited in literature as the most effective, with rates of therapeutic responses of 71% to 100% with a 1-year survival rate of 69-98% and a 3-year survival rate of 41-82%(18-21).The results of Bonner’s study showed that the combination of Cetuximab (Erbitux) to radiotherapy determines an absolute benefit for survival (10% at 5 years), similar to that achieved by the addition of other chemotherapy regimens to radiotherapy (8% at 5 years) and represents an alternative to the clasical radiochemotherapy with similar efficacy and acceptable toxicity for locally advanced head and neck cancers with increased risk of local recurrence and/or locoregional (cT2-4 and cN2,3)(24-26).
A new approach to radio technology is required to improve locoregional control of the disease, namely, accelerated HART (Hyperfractionated radiotherapy), intensity modulated radiotherapy correlated with dynamic contrast imaging magnetic resonance (imaging-guided radiotherapy - GRT)(27-30).
According to data published in scientific journals, hyperexpression of p53 is correlated with the presence of mutant p53 form at a score of 1-2 (immunomarking present in 10-50% of tumor cells), expression of Ki67 index correlates with mitotic activity and EGFR hyperactivity indicates an uncontrolled division of cells and is present in 90% of head and neck epidermoid carcinomas(22-23).
Immunohistochemical study correlated with clinical study helped us to define the clinical and immunohisto-prognostic groups as follows:
- a. favorable prognosis: absence of immunomarking for EGFR, nuclear immunomarking for p53, Ki67 absent or present in <10% of tumor cells;
- b. intermediate prognosis: immunomarking weakly positive for EGFR, p53 nuclear immunomarking in 10-55% of tumor cells and nuclear Ki67 immunomarking in 10-45% of tumor cells;
- c. unfavorable prognosis immunomarking strongly positive for EGFR, p53 nuclear immunomarking positive in >55% of tumor cells and nuclear immunomarking Ki67 positive in >45% of tumor cells.
Conclusions
Correct staging is based on clinical ENT examination correlated with imaging examinations for evaluating the real extension of the disease and thus reducing the risk of errors and of therapeutic failures, due mainly to practicing surgery as a first therapeutic gesture in advanced stages of the disease.The group with poor prognosis includes patients diagnosed with squamous cell carcinoma poorly differentiated of the hypopharynx and larynx, in advanced locoregional stages, that in the absence of performant imaging techniques were understaged; in consequence, surgery was practiced as a first therapeutic gesture, a therapeutic error responsible for treatment failures recorded in terms of distant progression of the disease (lung metastasis and/or bone). In this group of patients showing hyperexpression of tumor markers (EGFR, p53 and Ki67) it is required that molecular targeted therapy should be administrated concurrent with radiotherapy.
Clinical phenotypes with predictive and prognostic value in ENT cancers are tumor location, disease stage and treatment given. Radiosensitising agents associated is the key to reducing 3 times the rate of local recurrence, but improvement of locoregional control remains an objective for performance-conformational radiation therapy with hyperfractionated dose regimen.
Immunohistochemical study correlated with clinical study helped us to define the clinical and immunohisto-prognostic groups based on the analysis of histopathological and immunohistochemical results, so that adequate therapy could be ensured.
In the pre-therapeutic balance is required a clinical and imaging diagnosis correlated with histopathological and immunohistochemical analysis, bulletins elements underlying a fair treatment to improve the prognosis of patients with risk and thus reducing therapeutic failures.
The group with poor prognosis includes patients diagnosed with squamous cell carcinoma poorly differentiated of the hypopharynx and larynx in advanced locoregional stages with strongly positive immunomarking for EGFR, nuclear immunomarking for p53 in more than 55% of tumor cells, and nuclear immunomarking for Ki67 positive in more than 45% of the tumor cells; that requires the association of Erbitux treatment to standard induction therapy and/or radiotherapy. n
Bibliografie
1. Ferlay J, Bray F, Pisani P, Cancer incidence, mortality and prevalence wordwide, version 1.0 (IARC Cancer Base No 5), Lyon: IARC Press, 2001.
2. Hill C, Doyon F., La fréquence des cancers en France en 2000 et leur évolution depuis 1950, Bull Cancer 2005; 92:7–11.
3. Jemal A, Murray T, Ward E, Cancer Statistics, 2005, CA, Cancer J Clin 2005;55:10-30.
4. Bădulescu F., Gorunescu F. - Informatică oncologică, metode statistico-informatice în oncologie, Ed. Didactică şi Pedagogică, 2003, 100-160.
5. Danic D, Maruic M, Uzarevic B, Milicic D (2000) Prognostic factors in squamous cell carcinoma of the larynx, ORL J Otorhinolaryngol Relat Spec 62:143–148.
6. Brasilino de Carvalho M (1998) Quantitative analysis of the extent of extracapsular invasion and its prognostic significance: a prospective study of 170 cases of carcinoma of the larynx and hypopharynx, Head Neck 20:16–21.
7. Lassaletta L, Garcia-Pallares M, Morera E, Bernaldez R, Gavilan J (2001) T3 glottic cancer: oncologic results and prognostic factors, Otolaryngol Head Neck Surg 124:556–560.
8. Bourhis J, Armand JP, Pignon JP. Update of MACH-NC (Meta-Analysis of Chemotherapy in Head and Neck Cancer) database focused on concomitant chemoradiotherapy, Proc Am Soc Clin Oncol 2004; 22 [abstract5505].
9. Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapy added to locoregional treatment for head and neck squamous cell carcinoma: three meta-analysis of updated individual data, Lancet 2000; 355:949–55 MACH-NC Collaborative Group.
10. HainsworthJD, Meluch AA, McClurkan S, Gray JR, Stroup SL, Burris HA 3rd, Yardley DA, Bradof JE, Yost K, Ellis JK, Greco FA, Induction paclitaxel, carboplatin and infusional 5-FU followed by concurrent radiation therapy and weekly paclitaxel/carboplatin in the treatment of locally advanced head and neck cancer: a phase II trial of the Minnie Pearl Cancer Research Network, Cancer J. 2002 Jul-Aug; 8(4):311-21
11. Pignon JP, Bourhis J, Domenge C, Designe L, Chemotherapy added to locoregional treatment for head and neck squamous cell carcinoma: three meta-analysis of updated individual data, Lancet 2000; 355:949–55.
12. Posner M, Colevas A, Tischler RB, The role of induction chemotherapy in the curative treatment of squamous cell cancer of the head and neck, Semin Oncol 2000; 27:13–24.
13. Ghi MG, Paccagnella A, D’Amanzo P, Mione CA, S, Paro S, Mastromauro C, Carnuccio R, Turcato G, Gatti C, Pallini A, Nascimben O, Biason R, Oniga F, Medici M, Rossi F, Fila G, Neoadjuvant docetaxel, cisplatin, 5-fluorouracil before concurrent chemoradiotherapy in locally advanced squamous cell carcinoma of the head and neck versus concomitant chemoradiotherapy: a phase II feasibility study, Int J Radiat Oncol Biol Phys., 2004 Jun 1;59(2): 481-.
14. Gibson MK, Li Y, Murphy B, Randomized phase III evaluation of cisplatin plus fluorouracil versus cisplatin plus paclitaxel in advanced head and neck cancer (E1395): an intergroup trial of the Eastern Cooperative Oncology Group, J ClinOncol 2005;23:3562-3567.
15. G, Kritselis G, Liossi P, Giannakouras G, Douzinas E, Katsilieris I, Induction chemotherapy followed by concurrent chemoradiation in advanced squamous cell carcinoma of the head and neck: final results from a phase II study with docetaxel, cisplatin and 5-fluorouracil with a four-year follow-up, Oral Oncol. 2006 Aug; 42(7):675-84. Epub 2006 May 30.
16. J. B. Vermorken, E. Remenar, C. van Herpen, J. GermaLluch, S. Stewart, T. Gorlia, M. Degardin, K. Schollen, J. Bernier, Standard cisplatin/infusional 5-fluorouracil (PF) vs. docetaxel (T) plus PF (TPF) as neoadjuvant chemotherapy for nonresectable locally advanced squamous cell carcinoma of the head and neck (LASCCHN): a phase III trial of the EORTC Head Neck Cancer Group (EORTC #24971) (abstract), ASCO Annual Meeting Proceedings (post-meeting edition), J ClinOncol 2004; 22:5508.
17. Chemotherapy (ICT) with cisplatin/5-fluorouracil (PF) vs. docetaxel (T) plus PF (TPF) followed by chemoradiotherapy (CRT) vs. CRT for unresectable locally advanced head and neck cancer (LAHNC) (abstract). ASCO Annual Meeting Proceedings (post-meeting edition). J Clin Oncol 2005;23:5578.
18. Machtay M, Rosenthal DI, Hershock D, Jones H, Williamson S, Greenberg MJ, Organ preservation therapy using induction plus concurrent chemoradiation for advanced respectable oropharyngeal carcinoma: a University of Pennsylvania Phase II trial, J Clin Oncol 2002; 20:3964–71.
19. Wee J, Tan EH, Tai BC, et al. Randomized trial of radiotherapy versus concurrent chemoradiotherapy followed by adjuvant chemotherapy in patients with American Joint Committee on Cancer/International Union Against Cancer Stage III and IV nasopharyngeal cancer of the endemic variety, J Clin Oncol 2005;23:6730-6738.
20. Mittal BB, Kepka A, Mahadevan A, Tissue/Dose Compensation to reduce toxicity from combined radiation and chemotherapy for advanced Head and Neck Cancers, Int J Cancer (Radiat Oncol Invest) 2001; 96:61-70.
21. Chan Atc, Teo Pml, Ngan Rk, Concurrent chemotherapyradiotherapy compared with radiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: Progression-free survival analysis of a phase III randomized trial, J Clin Oncol 2002; 20:2038–44.
22. J. Metges, et al. No statistical impact of intra-tumoral overexpression of EGFR, VEGF and p53 on the overall survival in head and neck squamous cell cancer (HNSCC): Preliminary results of the GORTEC 99-02 randomized trial, Journal of Clinical Oncology, 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June20 20 Supplement), 2007: 6010
23. Hardisson D. (2003), Molecular pathogenesis of head and neck squamous cell carcinoma, Eur Arch Otorhinolaryngol 260:502–508.
24. Bonner JA, Giralt J, Harari PM, Cetuximab prolongs survival in patients with locoregionally advanced squamous cell carcinoma of head and neck: A phase III study of high dose radiation therapy with or without cetuximab [abstract], J ClinOncol, 2004;22(14S): 5507.
25. Bonner JA, Harari PM, Giralt J, Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck, N Engl J Med. 2006; 354 (6): 567-578.
26. Bonner JA, Harari PM, Giralt J, Cetuximab prolongs survival in patients with locoregionally advanced squamous cellcarcinoma of head and neck: A phase III study of high dose radiationtherapy with or without cetuximab (abstract). ASCO Annual MeetingProceedings (post-meeting edition), J Clin Oncol 2004; 22: 5507.
27. Etessami A, Lapeyre M, Tortochaux J, Geo Frois L, Verrelle P, Domenge C, Wibault P, Auperin A, Bourhis J. Very accelerated RT versus accelerated RT + concomitant CDDP-5 FU in patients with palpable N2 and N3HNSCC: preliminary results of the GORTEC 96-01 randomize trial, Lung Cancer 2001;34[suppl 1], S68.
28. Abitbol A, Abdel-Wahab M, Lewin A, Troner M, Rodrigues MA, Hamilton-Nelson KL, Markoe A, Phase II study of tolerance and efficacy of hyperfractionated radiotherapy and 5-fluorouracil, cisplatin, and paclitaxel (Taxol) in stage III and IV inoperable and/or unresectable head-and-neck squamous cell carcinoma: A-2 protocol, Int J RadiatOncolBiol Phys. 2002 Jul 15;53(4):942-7.
29. Hliniak A, Gwiazdowska B, Szutkowski Z, Kraszewska E, Kukolowicz P, Jarzabski A, A multicentre randomized/controlled trial of a conventional versus modestly accelerated radiotherapy in the laryngeal cancer: influence of a 1 week shortening overall time, Radiother Oncol 2002; 62:1–10.
30. Chao KSC, Low DA, Perez CA, Intensity modulatedradiation therapy for head and neck cancers: the Mallinckrodt experience, Int J Cancer (Radiat Oncol Invest) 2000; 90:92-103.
Articole din ediția curentă

EDITORIAL
National Society for Medical Oncology (SNOMR) and continuously medical education
Alexandru Grigorescu
For the educational process in medicine generally and in medical oncology in particular, the experience exchange is very important. For this reason, I have organized in the National Society for Medical Oncology from Romania (SNOMR) many international events under the auspices of European Society for Medical O...
CASE PRESENTATION
Carcinomul pulmonar scuamos
Alexandru Grigorescu
Cancerul pulmonar fără celule mici scuamos este unul dintre cancerele care nu are încă un avantaj cert în cadrul terapiei țintite. Deși rezultatele cu terapii noi se lasă așteptate, unele studii au relevat noi medicamente care par să schimbe evoluția acestei boli incurabile. Cazul pe care îl prezentăm este ex...
CASE PRESENTATION
Ambivalenţa chimică: prezentare de caz
Sorin Buga, Chandana Banerjee, Finly Zachariah, Bonnie Freeman
Ambivalenţa chimică este un răspuns maladaptativ întâlnit la pacienţii trataţi cu opioide care ajung să utilizeze această medicaţie nu neapărat pentru ameliorarea durerii fizice produse de cancer, ci pentru a face faţă stresului emoţional asociat cu diagnosticul de cancer. Autorii prezintă cazul unei paciente...Articole din edițiile anterioare
ORIGINAL STUDY
Impactul diabetului de tip 2 asupra prognosticului pacienților cu carcinom hepatocelular
Andreea-Daniela Gheorghe, Alina-Doina Nicoară, Laura Mazilu
Obiectiv. Studiul a fost făcut pentru a evalua impactul diabetului de tip II la pacienții diagnosticați cu carcinom hepatocelular (HCC). Materiale și metode. Acesta este un studiu observațional desfățurat în Departamen...
ORIGINAL STUDY
Chimioterapia intraarterială a cancerelor sferei ORL
Ioan Andrei, Anda Crişan, Florinel Bădulescu, Mihai Cosmin Stan
Elementul-cheie care ne-a determinat să inițiem un studiu privind evaluarea beneficiilor chimioterapiei intraarteriale este faptul că, în ciuda progreselor terapeutice, prognosticul cancerelor sferei ORL este rezervat, c...
ORIGINAL STUDY