Tromboza sinusului venos lateral
Otogenic lateral sinus thrombosis
Abstract
Otogenic lateral sinus thrombosis (LST) occurs as an intracranial complication of otitis media. In the preantibiotic era, the mortality was almost 100%. Today, thanks to antibiotics, the rate of mortality dropped at 10%. In the context of chronic otitis media, the infection migrates through bone dehiscence or erosions and causes initially an abscess around the lateral sinus, with thrombophlebitis of the venules that surround the external wall of the sinus in the proximity to dura mater, and these will lead to necrosis of the sinus wall, determining the adhesion of fibrin and platelets and, finally, forming a mural thrombus, which evolves towards superinfection and sinus occlusion. Parts of the infected thrombus will break off and enter the blood stream, with all the general symptoms and the possible complications from it. We present and discuss a case of lateral sinus thrombosis following chronic otitis media in the pandemic context. The particularity of the case is given by the COVID-19 restrictions. In the absence of the antibiotic therapy, due to the pandemic circumstances, the child developed a typical form of LST. Knowledge of the clinical manifestations of “classic” lateral sinus thrombosis facilitated the diagnostic process. Fortunately, today our patient was able to benefit from powerful broad-spectrum antibiotics which, combined with the surgical treatment, saved his life.Keywords
chronic otitis medialateral sinus thrombosisCOVID-19 pandemicRezumat
Tromboza sinusului venos lateral (TSL) poate să apară ca o complicaţie intracraniană a otitei medii. În era preantibiotică, mortalitatea era de aproape 100%. Astăzi, datorită antibioticelor, rata mortalităţii a scăzut la 10%. În contextul otitei medii cronice, infecţia migrează prin dehiscenţele osoase sau prin zonele erodate şi determină iniţial un abces în jurul sinusului lateral, cu tromboflebita venulelor care înconjoară peretele extern al sinusului în apropierea durei mater, iar secundar se produce necroza peretelui sinuzal, determinând aderenţa fibrinei şi a trombocitelor, în final formând un tromb mural, care evoluează spre suprainfecţie şi ocluzie sinuzală. Părţi ale trombului infectat se vor rupe şi vor intra în fluxul sanguin, cu toate simptomele generale şi posibilele complicaţii consecutive. Prezentăm şi discutăm un caz de TSL în urma unei otite medii cronice în context pandemic. Particularitatea cazului este dată de restricţiile impuse de pandemia de COVID-19. În absenţa terapiei cu antibiotice din cauza circumstanţelor pandemice, adolescentul a dezvoltat o formă tipică de tromboză a sinusului venos lateral. Cunoaşterea manifestărilor clinice „clasice” ale TSL a facilitat procesul de diagnosticare. Din fericire, pacientul a putut beneficia de antibiotice cu spectru larg, care, combinate cu tratamentul chirurgical, i-au salvat viaţa.Cuvinte Cheie
otită medie cronicătromboza sinusului lateralpandemia de COVID-19Introduction
Lateral sinus thrombosis (LST) is generally considered the third or fourth most common complication among all intracranial complications of chronic otitis media(1). In the preantibiotic era, it was one of the most frequent fatal complications of otitis media, ranking second place after meningitis. Nowadays, in the era of antibiotic treatment of suppurative ear disease, LST accounts for 6% of all intracranial complications(2,3). Still, it is a rare otogenic complication that can have serious consequences if left untreated. It is frequently associated with other intracranial or extracranial complications(4,5). LST is difficult to diagnose based on clinical signs, because the associated complications and the antibiotic treatment mask the typical symptoms that might help the physician to make a correct diagnosis.
Case report
A 17-year-old young male with a history of chronic suppurative otitis media from early childhood, having numerous episodes of active otitis as a child, presented with a septicemic state, with left hemicrania, “picket-fence” fever (38.5-40ºC), intense otalgia and left otorrhea, symptoms that had become more intense seven days before presentation, with the worsening of the general condition in the last day.
Otomicroscopy after ear cleaning revealed mucopurulent discharge in a large amount from the middle ear through a near-total tympanic membrane perforation.
The patient has also a puffy edema of the postauricular soft tissues overlying the mastoid process (Griesinger’s sign).
The clinical features pointed towards an infectious complication of middle ear origin.
Among the blood tests performed, the C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), leukocytes and fibrinogen had very high levels.
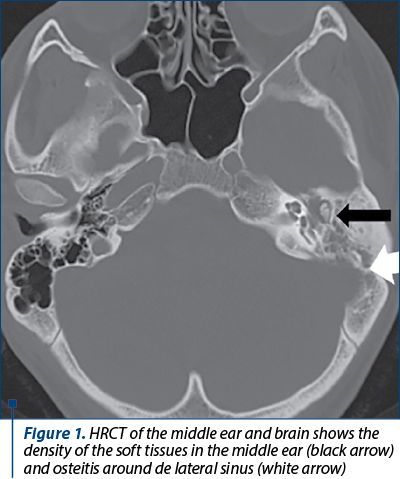
A high-resolution computed tomography (HRCT) with intravenous contrast revealed soft tissue densities present in the left mastoid and in the tympanic cavity (Figure 1)
and a filling defect at the level of lateral venous sinus (Figure 2)

and internal jugular vein (Figure 3),

without other signs of intracranial complications. Bacteriology smears and culture were negative.
The surgical treatment was decided shortly. We performed a canal wall down mastoidectomy with a wide meatoplasty. Intraoperatively, extended areas of osteitis and bone erosion of the external sinus wall were detected and removed.
The lateral sinus wall was exposed and punctured but, the sinus being occluded, a small amount of hemolyzed blood was all we got. We decided to open the sinus and try to remove the thrombus, but without succeeding to evacuate it entirely. The mastoid and tympanic cavities were rinsed with an antibiotic solution. An iodoform impregnated pack was left in the mastoid cavity.
Systemic antibiotic treatment was initiated in double therapy (vancomycin 2 g/12 h plus meropenem 1 g/8 h) associated with anticoagulants (Clexane® 40 mg x 2/day) and vitamin therapy (B1, B6).
There was a great improvement of all symptoms and signs on the first postoperative day. The patient was kept on a fifteen-day course of intravenous antibiotics. The pack was removed on the tenth day, and we placed sutures to close the incision.
The spread of the infection from the middle ear to the lateral sinus may be directly through bone erosion secondary to cholesteatoma or granulation tissue surrounding the outer wall of the sigmoid sinus, and may occur from infected small venules in connection with the sinus or through a dehiscence of the bone in the vicinity of the sinus. The final result is the formation of an obliterating thrombus. The thrombus may grow superiorly to other cranial sinuses and inferiorly to the internal jugular vein. Thrombus formation helps to restrict the infection and may be considered as a protective mechanism(3,6,7).
The most frequent symptoms at the LST onset are headache, fever, otalgia, otorrhea and vomiting. Signs of infection such as “picket-fence” fever due to septic thrombus that break down from the sinus thrombosis, and otalgia from exacerbation of the chronic ear disease, associated with signs of cerebral edema like severe headache and papilledema, are considered as being specific for LST. These symptoms and signs represented the classical presentation of LST in the preantibiotic era. Tenderness and edema over mastoid (Griesinger’s sign) are also characteristic for LST, being the result of thrombosis of the emissary vein. Pain in the neck along the sternocleidomastoid muscle, meaning internal jugular vein involvement and cranial nerve palsy, may be encountered in severe cases – our patient did not have this kind of complains, although, for instance, the jugular vein was affected. The COVID-19 pandemic – with the shortage of medical attention for other diseases and, thus, the lack of antibiotic treatment in the initial stage of the middle ear infection reactivation – took us back to the preantibiotic period. The clinical picture of LST was clear, without the well-known masking effect of the previous use of antibiotics or overlap of signs and symptoms with other concomitant infections(3,6,8).
The imaging exams to evaluate the patients with LST are important. CT and MRI are the investigations of choice. High-resolution CT scan shows the classic “delta sign” of peri-sinus dural enhancement and filling defect of the lateral sinus. Simultaneously, other intracranial complications (meningitis, different intracranial abscesses etc.) are common among patients with LST, complications that might be discovered also on the CT scan(3,9). Magnetic resonance imaging is an important exam in LST, being more sensitive than computed tomography in detecting the thrombus, but it is also more difficult to be performed in young children and more expensive than CT. It must be known that MRI is not mandatory, since the definitive diagnosis of LST is made at surgery. Doppler echography of the internal jugular vein may be equally useful.
The treatment is surgical, in combination with broad-spectrum intravenous antibiotics. Anticoagulant therapy might be associated.
Mastoidectomy with the removal of the entire thrombus, when is possible, and local packing are the treatment of choice(9). When the removal of the entire clot is not possible, its evacuation as much as possible will be acceptable. The antibiotics will be administered for two to three weeks. Anticoagulation therapy is under debate, and we usually recommend it under the supervision of the anesthesiologist or hematologist(9).
Still, the patient’s evolution must be carefully monitored, because a secondary intracranial complication has been reported in literature(6,10).
Conclusions
Due to the pandemic circumstances, the patient developed a typical form of lateral sinus thrombosis. Knowledge of the clinical manifestations of “classic” LST facilitated the diagnostic process. HRCT scan was a bonus in the case management. Fortunately, today our patient was able to benefit from powerful broad-spectrum antibiotics which, combined with the surgical treatment, saved his life.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY

Bibliografie
-
Viswanatha B, Naseeruddin K. Lateral sinus thrombosis in otology: a review. Mediterr J Hematol Infect Dis. 2010 Sep 7;2(3):e2010027. doi: 10.4084/MJHID.2010.027.
-
Ameri A, Bousser MG. Cerebral venous thrombosis. Neurol Clin. 1992 Feb;10(1):87-111.
-
Luntz M, Brodsky A, Nusem S, Kronenberg J, Keren G, Migirov L, Cohen D, Zohar S, Shapira A, Ophir D, Fishman G, Rosen G, Kisilevsky V, Magamse I, Zaaroura S, Joachims HZ, Goldenberg D. Acute mastoiditis – the antibiotic era: a multicenter study. Int J Pediatr Otorhinolaryngol. 2001 Jan;57(1):1-9. doi: 10.1016/s0165-5876(00)00425-0.
-
Singh GB, Rai AK, Singh S, Sinha M. A rare case of lateral sinus thrombosis with carotid space abscess. Case Rep Otolaryngol. 2012;2012:165987. doi: 10.1155/2012/165987.
-
Bianchini C, Aimoni C, Ceruti S, Grasso DL, Martini A. Lateral sinus thrombosis as a complication of acute mastoiditis. Acta Otorhinolaryngol Ital. 2008;28(1):30-33.
-
Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, deVeber G, Ferro JM, Tsai FY; American Heart Association Stroke Council and the Council on Epidemiology and Prevention. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011 Apr;42(4):1158-92. doi: 10.1161/STR.0b013e31820a8364.
-
Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004 Mar;35(3):664-70. doi: 10.1161/01.STR.0000117571.76197.26.
-
Cavalcanti DD, Raz E, Shapiro M, Dehkharghani S, Yaghi S, Lillemoe K, Nossek E, Torres J, Jain R, Riina HA, Radmanesh A, Nelson PK. Cerebral Venous Thrombosis Associated with COVID-19. AJNR Am J Neuroradiol. 2020 Aug;41(8):1370-1376. doi: 10.3174/ajnr.A6644.
-
Iseri M, Aydin O, Ustündağ E, Keskin G, Almaç A. Management of lateral sinus thrombosis in chronic otitis media. Otol Neurotol. 2006 Dec;27(8):1098-103. doi: 10.1097/01.mao.0000232002.62997.f3.
-
Tovi F, Fliss DM, Noyek AM. Septic internal jugular vein thrombosis. J Otolaryngol. 1993 Dec;22(6):415-20.

Forum ORL.ro rezumate
...
Femei celebre în stomatologie – secolele XVIII-XIX
Mihai Burlibaşa, Radu Cătălin Costea, Irina Adriana Beuran, Ioana Maria Stoica, Bogdan Alexandru Dumitru, Nicoleta Măru
După cum am arătat deja şi în prima parte a acestui material, emanciparea femeilor, atât în Europa, cât şi în SUA, a început cu adevărat în a doua jumătate a secolului al XIX-lea. ...
Aspecte practice privind corelaţia dintre dimensiunea verticală de ocluzie şi aspectul facial în edentaţia totală
Iuliana Babiuc, Mihai-Alexandru Gărgăianu, Radu Costea, Viorel Ştefan Perieanu, Mircea Popescu, Mădălina Violeta Perieanu, Ileana Ionescu, Mihai Burlibaşa
După cum bine ştim, munca medicului stomatolog este deosebit de importantă atunci când se realizează o determinare corectă a d.../24 - Otita externa necrozanta.webp)
Otita externă necrozantă (malignă) – revizuire narativă
Vlad Cozma, Corina Butnaru, Cristian Mârţu, Bogdan-Mihail Cobzeanu, Petronela Moraru, Luminiţa Rădulescu
Otita externă malignă (OEM), denumită și otită externă necrozantă, reprezintă o infecție rară a conductului auditiv extern care progresează către țesuturile moi învecinate, osul temporal și baza craniului. ...
6 ani de screening auditiv neonatal universal la Iaşi - rezultatele unui parteneriat interdisciplinar
Sebastian Cozma, Cristian Mârţu, Oana Manolache, Raluca Olariu, Gabriela Damean, Bogdan Cavaleriu, Diana Zota, Dan Mârţu, Luminiţa Rădulescu
Programul de detecţie a hipoacuziei la nou-născuţi se desfăşoară la Iaşi în mod neîntrerupt din anul 2008. La baza succesului aces...