Semnificaţia gazelor din cordonul ombilical în encefalopatia nou-născutului – review al literaturii
The significance of cord gases in neonatal encephalopathy – overview
Abstract
Experimental studies and animal models have shown that hypoxic ischaemic encephalopathy (HIE) is not a single event, but rather an evolving process, resulting in cell death. Therapeutic hypothermia is used to break the process and protect the neurons from secondary injury. Cord gases analysis plays an important role in defining the population of babies who will benefit of therapeutic hypothermia. However, the physiology of cord gases is complicated and one should be aware of the pitfalls associated with interpreting their values.Keywords
cord gaseshypothermianewborn encephalopathyRezumat
Studii experimentale şi modele animale au arătat că encefalopatia hipoxic-ischemică este un proces în evoluţie, mai degrabă, decât un eveniment singular, care are ca rezultat final moartea celulară. Hipotermia terapeutică este folosită pentru a opri acest proces şi pentru a proteja neuronii de injuria secundară. Analiza sângelui din cordonul ombilical joacă un rol important în definirea populaţiei de nou-născuţi care beneficiază de hipotermie terapeutică. Totuşi, fiziologia gazelor din cordonul ombilical este complicată şi trebuie luate în considerare problemele care intervin în interpretarea valorilor acestora.Cuvinte Cheie
gaze din cordonul ombilicalhipotermieencefalopatia nou-născutuluiExperimental studies and animal models have shown that hypoxic ischaemic encephalopathy (HIE) is not a single event, but rather an evolving process, resulting in cell death. The cause is an initial hypoxic event in the perinatal period. Following this, brain cells are depleted of energy and die. Some neurons die in the initial phase and this injury is irreversible(1).
However, magnetic resonance spectroscopy showed that infants with evidence of moderate to severe asphyxia have an initial, transient recovery of cerebral oxidative metabolism, followed by secondary injury with cerebral energy failure from 6 to 15 hours after birth(2). The severity of the secondary injury correlates with the neurodevelopmental outcome(3). Studies have shown that the babies with encephalopathy who did not show the initial metabolic recovery had worse outcomes(2). This pattern of initial recovery followed by secondary energy failure was also observed on piglet, rat and sheep models. Initiating hypothermia prevents secondary injury by slowing the cerebral metabolism.
The UK resuscitation council recommends that term or near-term infants, with evolving moderate to severe hypoxic-ischaemic encephalopathy, should be treated with therapeutic hypothermia(4). This can be obtained either by whole body cooling or by selective head cooling. Cooling should be initiated and conducted in neonatal intensive care units, following clear protocols. The cord gases or a blood gas in the first hour of life are used as part of the criteria for initiating cooling.
The secondary injury occurs typically 6 hours after the initial injury; therefore, hypothermia must be started during the latent phase, ideally within the first 3 hours following the ischaemic event, to achieve the best possible neuroprotective effect.
Many infants are born in small hospitals without neonatal intensive care units or access to therapeutic hypothermia, hence the neonatal transport team plays a key role in establishing and maintaining therapeutic hypothermia during transport to tertiary centers.
The criteria for therapeutic hypothermia are defined according to the Total Body Hypothermia for Neonatal Encephalopathy Trial (TOBY). There are ‘A’ criteria and ‘B’ criteria. The ‘A’ criteria comprise the infants more than 36 completed weeks gestation, admitted to the neonatal unit with at least one of the following: Apgar score of ≤5 at 10 minutes after birth, continued need for resuscitation (including endotracheal or mask ventilation) at 10 minutes after birth, acidosis within 60 minutes of birth (defined as any occurrence of umbilical cord, arterial or capillary pH<7), Base Deficit ≥16 mmol/L in umbilical cord or any blood sample (arterial, venous or capillary) within 60 minutes of birth. Infants that meet criteria ‘A’ should be assessed for the neurological abnormality entry criteria ‘B’, i.e. seizures or moderate to severe encephalopathy, consisting of: altered state of consciousness (reduced response to stimulation or absent response to stimulation) and abnormal tone (focal or general hypotonia, or flaccid) and abnormal primitive reflexes (weak or absent suck or Moro response). Infants who meet criteria ‘A’ and ‘B’ are considered for treatment with cooling(5).
Safety versus efficacy must be balanced for preterm infants. All infants are at risk for cold stress following delivery, and thermoregulation is extremely important in the case of preterm infants. There is increased evidence that cold stress increases mortality in preterm infants, however so far there is no evidence that hypothermia is beneficial for babies born more than 34 weeks preterm.
Cord gases analysis plays an important role in defining the criteria for cooling and the risk of HIE in newborn babies. There is significant variability in defining abnormality, outcomes and the values measured (arterial cord pH, venous cord pH, or base excess)(6).
In 1958, James et al. recognised that umbilical cord blood gas analysis can give an indication regarding preceding fetal hypoxic stress(7). Since then, it has become accepted that cord gases can provide important information with regards to perinatal stress and outcomes of newborn babies. Umbilical cord blood gas analysis is recommended in all high-risk deliveries by both the British and American Colleges of Obstetrics and Gynaecology(8,9). In some centers it is practiced routinely following all deliveries.
Cord gases can describe the acid-base balance of the infant at the moment of birth, when the umbilical circulation was stopped by clamping of the cord. However, the umbilical cord can become obstructed before birth, which causes a progressive increase in the difference between umbilical arterial and venous blood gas values.
Martin et al. showed that term infants with evidence of cord compression have larger differences between umbilical venous and arterial gases(1). However, in cases of placental abruption the arterial to venous differences are small(11). If the obstruction to the umbilical vessels was sudden, complete and persisted until delivery, the cord gases would provide information about the fetal acid-base balance prior to the obstruction, and maybe normal despite severe intrapartum asphyxia(12). Therefore, normal cord gases in the context of severe compromise of the newborn do not exclude acute intrapartum asphyxia.
The American Congress of Obstetricians and Gynaecologists recommends that cord gases should be obtained in the following circumstances:
- Caesarean delivery for fetal compromise
- Low 5-minute Apgar score
- Severe growth restriction
- Abnormal fetal heart rate tracing
- Maternal thyroid disease
- Intrapartum fever
- Multifetal gestations(13).
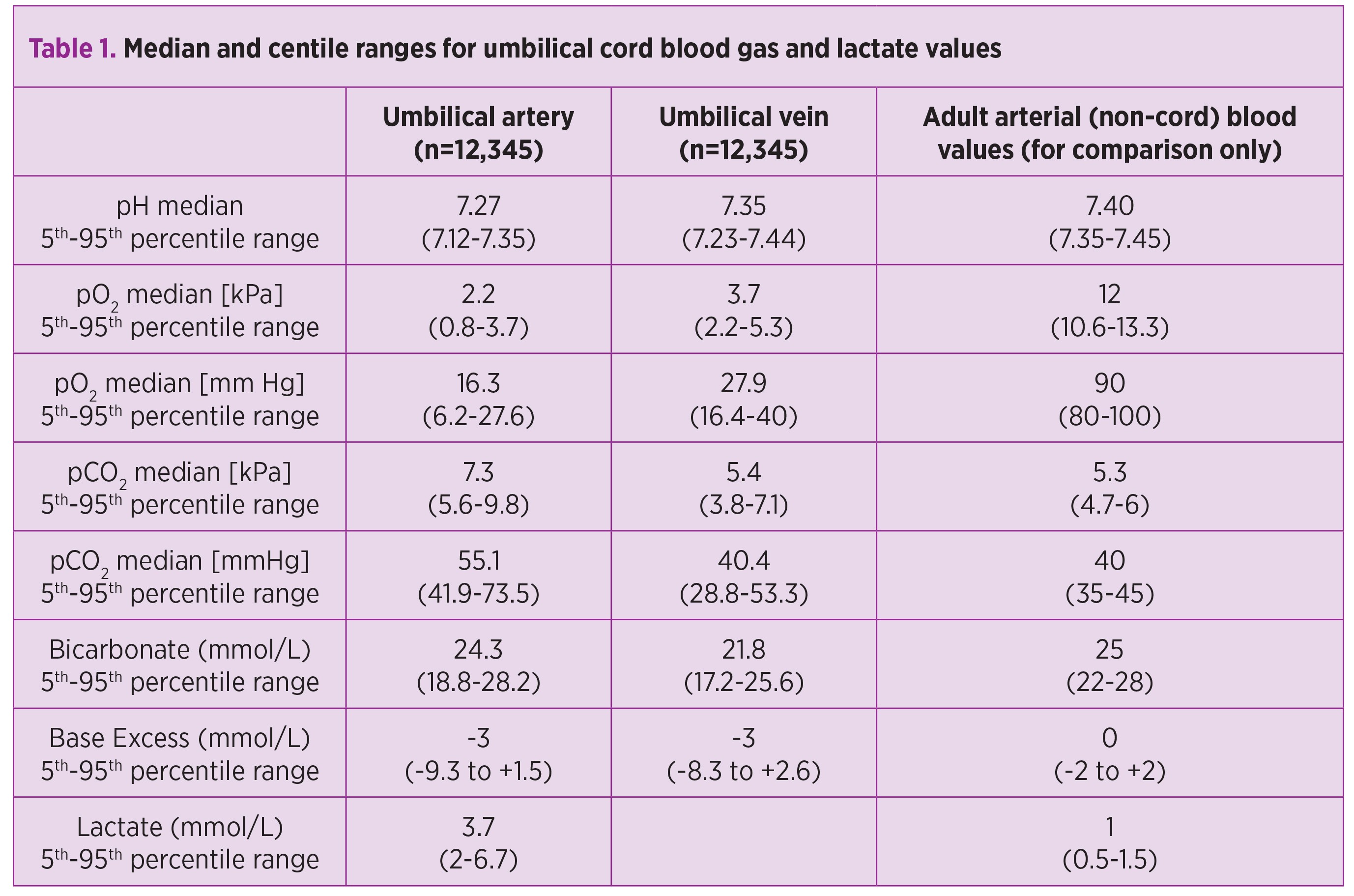
Because fetal carbon dioxide is removed from the umbilical arterial blood in the placenta, umbilical venous blood should have a slightly higher pH and lower pCO2 than umbilical arterial blood. Parity, breech presentation, mode of delivery and other factors influence cord gas values. Reference ranges for term infants are summarised in table 1(14).
Cord pH or base excess alone are poor predictors of outcome. Also, most infants with evidence of intrapartum asphyxia do not develop serious long-term sequelae. However, the combination of low pH at birth and abnormal clinical signs is strongly predictive of poor neurological outcome.
Perlman et al. showed that a combination of cord pH<7, need for intubation and Apgar <5 at 5 minutes had an 80% positive predictive value for the development of seizures(15). Portman R.J. et al. developed and validated a scoring system for predicting multiorgan impairment following perinatal asphyxia(16). A score combining cardiotocographic abnormality, umbilical arterial base excess, and low 5-minute Apgar score was strongly associated with morbidity compared with any individual factor. Carter et al. showed that the score had a positive predictive value of 73% and a negative predictive value of 99% for impairment of three or more organ systems(17).
The predictive value of isolated umbilical cord blood analysis for morbidity and mortality in preterm infants is less clear. However, Victory et al. demonstrated a relationship between increasing metabolic acidosis and poor outcomes in a cohort of preterm and very preterm babies(18).
A systematic review found that low arterial cord pH showed a consistent association with poor neonatal outcomes and this can be used to inform clinical management. This review suggested that arterial cord pH can be used as an important outcome measure alongside neonatal morbidity and mortality in obstetrics(19). The review analysed 51 articles, with a total of 481753 infants meeting the selection criteria. The meta-analysis showed that low arterial cord pH was significantly associated with neonatal mortality (odds ratio [OI] 16.9, 95% confidence interval [CI] 9.7 to 29.5), hypoxic ischaemic encephalopathy (OI 13.8, 95% CI 6.6 to 28.9), intraventricular hemorrhage or periventricular leukomalacia (OI 2.9, 95% CI 2.1 to 4.1), and cerebral palsy (OI 2.3, 95%CI 1.3 to 4.2).
Conclusions
Umbilical cord arterial acid-base balance and gas assessment remains the most objective determination of the fetal metabolic condition at the moment of birth. The avoidance of a low cord pH at birth is a target for day to day obstetric practice. Based on existing evidence, increased initial surveillance of neonates born with a low arterial cord pH, regardless of their clinical condition, may prove beneficial as the incidence of complications has been shown to be higher in this group. It is difficult to draw strong conclusions on the necessity of long term follow-up for babies with low arterial cord pH; however there appears to be an association with adverse neurological outcomes, and this may need to be explored further.Bibliografie
1. Davidson J O, Wassink G, Van den Heuij L G, et al. Therapeutic Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy – Where to from Here?; Front Neurol. 2015; 6: 198.
2. Lynn A, Beeby P. Cord and placenta gas analysis: The accuracy of delayed sampling, Arch Dis Child Fetal Neonatal Ed 2007, 92F281–F285.
3. Sykes GS, Molloy PM. Effect of delays in collection or analysis on the results of umbilical cord blood measurements, Br J Obstet Gynaecol 1984 Oct(91)989–92.
4. UK Resuscitation Council guidelines, https://www.resus.org.uk/resuscitation-guidelines.
5. TOBY trial; https://www.npeu.ox.ac.uk/toby
6. Armstrong L, Stenson BJ. Use of umbilical cord blood gas analysis in the assessment of the newborn, Arch Dis Child Fetal Neonatal Ed. 2007 Nov; 92(6): F430–F434.
7. James L S, Weisbrot I M, Prince C E. et al. The acid-base status of human infants in relation to birth asphyxia and the onset of respiration, J Pediatr 1958 Apr 52(4)379–94.
8. Royal College of Obstetricians and Gynaecologists - Clinical Effectiveness Support Unit - The use of electronic fetal monitoring: the use and interpretation of cardiotocography in intrapartum fetal surveillance. London: RCOG, 2001, http://www.rcog.org.uk.
9. ACOG Committee Opinion No 348, November 2006: Umbilical cord blood gas and acid-base analysis. Obstet Gynecol 2006 Nov, 108(5)1319–22.
10. Martin GC, Green RS, Holzman IR. Acidosis in newborns with nuchal cords and normal Apgar scores, J Perinatol 2005 Mar 25(3)162–65.
11. Johnson JW, Richards DS. The etiology of fetal acidosis as determined by umbilical cord acid-base studies, Am J Obstet Gynecol 1997 Aug 177(2)74–80.
12. Nakamura KT, Smith BA, Erenberg A et al. Changes in arterial blood gases following cardiac asystole during fetal life, Obstet Gynecol 1987 Jul 70(1)16–7.
13. The American Congress of Obstetricians and Gynecologists, Number 348, November 2006, (Reaffirmed 2012); Committee on Obstetric Practice.
14. White C, Doherty D, Henderson J et al. Benefits of introducing universal cord blood gas and lactate analysis into an obstetric unit, Australia and New Zealand J of Obstetrics and Gynaecology 2010; 50: 318-28.
15. Perlman JM, Risser R. Can asphyxiated infants at risk for neonatal seizures be rapidly identified by current high-risk markers? Pediatrics 1996 Apr 97(5)456–62.
16. Portman RJ, Carter BS, Gaylord MS et al. Predicting neonatal morbidity after perinatal asphyxia: a scoring system, Am J Obstet Gynecol 1990 Jan 162(1)174–82.
17. Carter BS, McNabb F, Merenstein GB. Prospective validation of a scoring system for predicting neonatal morbidity after acute perinatal asphyxia, J Pediatr 1998 Apr 132(4)619–23.
18. Victory R, Penava D, da Silva O et al. Umbilical cord pH and base excess values in relation to neonatal morbidity for infants delivered preterm, Am J Obstet Gynecol 2003 Sep 189(3)803–7.
19. Malin GL, Morris RK, Khan KS. Strength of association between umbilical cord pH and perinatal and long term outcomes: systematic review and meta-analysis; BMJ 2010, 340.

Modul în care anumite prebiotice reduc incidenţa dermatitei atopice
Bernd Stahl
Dr. Bernd Stahl, Director R&D în domeniul Cercetării Laptelui Uman la Nutricia Research, Utrecht, Olanda, discută despre rezultatele cercetării asupra efectului antialergenic al bacteriilor benefice din intestin şi despre modul în care activitatea şi numărul acestora ar putea fi încurajate cu oligozaharide sp...
Aspecte medico-legale în osteocondrodisplaziile neletale
Elena Alina Bordea, Diana-Elena Comandașu, C. Coroleucă, Octavia Velicu, Elvira Brătilă, Mihai Mitran
Osteocondrodisplaziile (OCD) sunt un grup larg, heterogen, de anomalii care implică formarea şi creşterea oaselor. Numite şi displazii scheletale, se pot manifesta încă din stadiile precoce ale dezvoltării fetale şi pot ...
Hernie congenitală diafragmatică pe partea dreaptă - prezentare de caz
Gheorghiţa Sardescu, , Adriana Sbârcea, Cătălin Cîrstoveanu
Hernia diafragmatică congenitală este o patologie ce constă în existenţa unui defect la nivelul diafragmului abdominal, din pricina căruia are loc migrarea viscerelor abdominale în cavitatea toracică....