Din aceeași categorie
Tratamentul carcinomului renal metastatic cu terapiile TKI şi mTOR: prezentare de caz

Introduction
Real-world data
Real-world data (RWD) have started to play an important role in clinical research and in decision making in medical practice. Beginning with 2016, the medical world in the United States of America has started using more RWD when considering regulatory decision-making. Generally speaking, RWD are represented by observational data, which are extracted outside of controlled clinical studies, thus they are generated by day-to-day clinical practice. The United States Food and Drug Administration (FDA) describes RWD as originating from a series of sources like medical electronic records, observation charts from clinics and hospitals, medical assertions, financial receipts from private clinics, disease registries and patient-generated data.
Real-world evidence data (RWE) offer useful information regarding the hallmarks of included patients either from observational studies, or directly form collected data from official evidences. Accordingly, RWE helps contour a so-called patient profile and also helps to determine the choice of therapy line(s), dosing strategies, treatment sequencing, toxicity and adverse events management. In spite of these, the whole potential of real-world evidence data remains unexploited in healthcare primarily because of structural and behavioral factors. Structural factors include the lack of legislation regulation, lack of fast availability of real-world data and the quality and integrity deficit of these data. Behavioral factors include healthcare providers’ rigid mentalities that lead to misunderstanding and not rapidly incorporating the RWE.
Correspondingly, observational studies are often used for emphasizing benefits of new cancer approved therapies. These studies are often used for analyzing evidence from medical databases of hospitals and other medical institutions, and are especially meaningful if these data come in an electronic form(1).
Observational studies
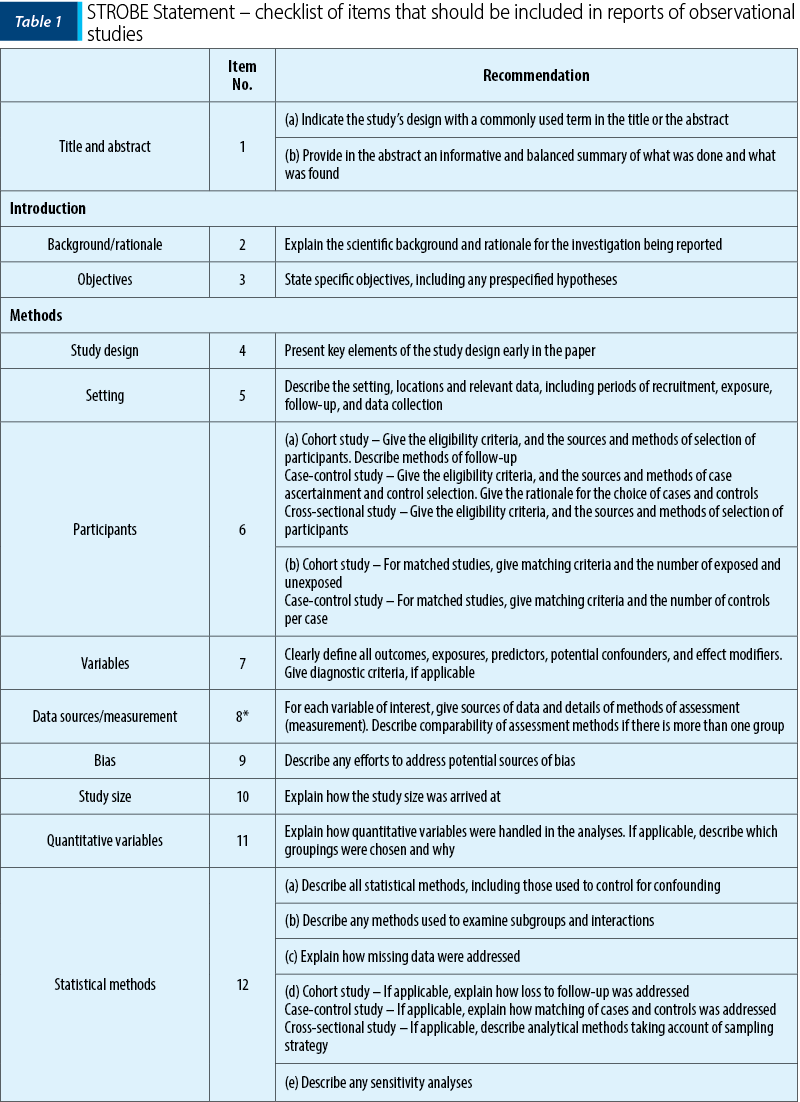
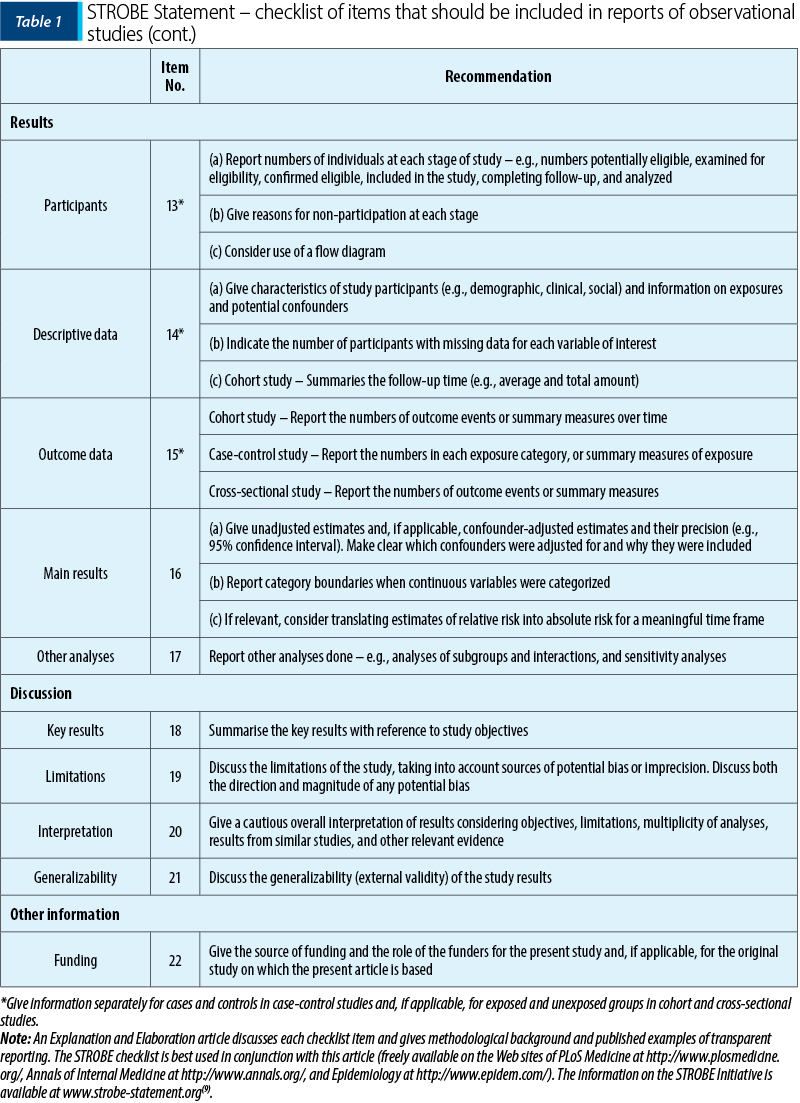
RWD are related to observational studies. An observational study represents the research analysis conducted for observing the effects of intervention, risk factors, diagnostic tests or new forms of therapy. This kind of research must statistically evaluate the results, without trying to influence who is, or who is not exposed to these(2).
For a better understanding of observational studies, we will also reiterate another description that defines the type of our study: “Observational studies observe the effects of a risk factor, diagnostic test, treatment, or other types of interventions, without trying to change the exposure model. Cohort studies and case-control studies are two types of observational studies”. Our research consists of a case-control type of study. This type of study is defined as follows: the research identifies people with an already known health issue (“cases”) and also a similar group, but without health issues (“control”). Then these two groups are compared regarding exposure(s)(3).
Observational studies for determining the efficiency of therapies with new drugs
The most suitable standard design for determining the effectiveness of a therapy is considered to be the randomized controlled study (RCS). This is attributed to the fact that randomization raises the probability that the therapy prescribing is independent from patient characteristics (known and unknown), and the possibility of response to treatment can be scientifically evaluated(4).
The smaller number of the patients enrolled in a randomized controlled trial (RCT) determine the decrease of the significance of the results. This kind of alteration leads to an inaccurate estimation of efficacy. Regarding randomized controlled studies, observational studies can be used to examine the efficacy of drugs that already have been endorsed with marketing approval; observational studies can also be used for already approved drugs, for the reason that later study funding is limited. Secondly, observational studies can also verify the efficacy for rare indications of drug therapy(5).
Finally, there is a third situation where observational studies can be used: when the sample size of the patient lot is more representative of a specific clinical population, and less predisposed to the rigid characteristics of study accrual. Thus, it can allow external validity investigation of study results in heterogenous populations, rural or urban areas, older geriatric patients, which are often underrepresented in randomized controlled studies(6).
Researchers have theorized if randomized controlled studies are still to be considered as the mainstay of research for evaluating efficiency and safety profiles of new medications. Therefore, for a long time, RCTs have been the gold standard for evaluating new drugs and their pharmacology profiles. These studies are considered the most efficient method for overcoming the bias error of research and also to bring high-quality evidence, because patients are randomly assigned to receive the study drug, either a control/comparison product. The enrolled patients do not know which group they are assigned to, and all the other variables are maintained constant. In some studies (these are called double-blind), neither the investigator, nor the patient know what drug has been assigned to the participants(7).
Internationally recognized science associations have begun studying the roles and limitations of randomized controlled studies. The New York Science Academy has already organized a meeting for discussing the roles of RCTs. This board has included eminent representatives from pharma industry, the FDA, patients’ support groups, government health organizations and from universities, including Harvard and Duke. It has been stated that the amounts of time and funding necessary for RCTs are too overwhelming for pharma industry. The companies involved in the studies conducted have to invest significant amounts of funds and time for finding a sufficient large enough patients’ group, according to the sample size, so that the studies’ results are statistically significant. Also, the needs for systematizing a large group of study testing sites, the process of delivery comparison products and generally overseeing the whole process are very difficult to coordinate. Many companies do not possess the mandatory resources for finalizing the whole process in due time, especially if they are involved with many drugs in their pipeline(8).
Ethical issues have an important role in the debates. There have been voices who have stated that placebo using is unethical, because it means deceiving patients with advanced disease that they will receive a drug that might be useful and, instead, the investigators administrate a sugar pill. The strict supervision of RCTs in the pharma business removes the feeling of compassion towards the patients, resulting in them feeling like lab rats. This conference’s conclusions have stated that clinical trials still remain an important method for research and testing, but there is a need for innovatory approaches that will permit a larger number of patients to access investigational products, when they most need it. This condition could be attained by organizing more pragmatic studies, closer to “real-world data”. Also, is has been proposed that the FDA preliminary approves a drug usage using a surrogate endpoint, thus allowing the study to go on, until final testing is done to confirm the conclusions(8).
Observational study types
An observational study consists of research in which the variables involved are beyond of researchers’ control. As the term suggests, an observational study observes the real world, different from creating a controlled experiment. These are used especially when an experiment would prove to be unethical. Observational studies often require low development costs and large sample sizes. The following are common types of observational studies.
1. Natural experiments – a natural experiment is represented by a real situation which exhibits close resemblance to an experiment. For example, a state that bans a contaminant, but other states do not.
2. Case-control study: identifying groups based on results and then examining those results comparing them both with historical data. For example, comparing cancer diagnosed adults’ habits with healthy adults’ habits. This method was used by the early studies that have settled the link between smoking and lung cancer – Richard Doll and Bradford Hill study “Lung cancer and other causes of death in relation to smoking” (1956).
3. Case studies: these studies are closely related to a detailed analysis – for example, Jeanne Calment, a French woman who lived to be 122 years old. She was considered to be the oldest human to have ever lived on Earth. Case studies are based on interviews with her because she was very famous when she was “just” 111 years old, being remarkably full of life, with preserved cognitive function until the end. She also participated in medical examinations, including computed tomography when she was 118 years old.
4. Multidisciplinary study – fetching and analyzing data for a certain population at a certain time, like observing a population for a period of time. This can be either a short period, or a long period. For example, the Grant Study, that analyzes life results for 268 Harvard students from classes of 1939-1944 for a period of 75 years. Longitudinal studies are not observational, these being controlled experiments.
5. Prospective cohorts – these are longitudinal studies in which a cohort, a group with a common characteristic, is selected at the beginning of the study and then the collected data is analyzed in transversal sections. For example, a study over a period of 50 years, that determines the results of a certain community of people who have been breastfed whilst toddlers, compared with others who have not. A prospective cohort starts with the cohort and then collects future data.
6. Retrospective cohort – this is a longitudinal study based on historical data for cohorts. For example, comparing medical histories of people who have always lived in a geographical area with high-quality air.
7. Observational studies that advocate therapeutical recommendations. In the last decade, many scientists have debated if observational studies can support therapeutic recommendations made by oncology doctors. The question being asked would be this one: when a doctor recommends a certain therapy based on an observational study, what accuracy rate does this recommendation have?(10)
For solving this issue, we must keep in mind Kumar’s et al. study, who have collected data from national cancer treatment guidelines covering up to eight types of tumors. These guidelines make recommendations regarding drug therapy, surgical interventions and radiation therapy.
Another area of research is represented by identifying data from national cancer registry to see if these data are similar with those from randomized clinical trials. In this comparative efficacy research analysis, there have been included 141 randomized clinical trials from the National Cancer Database.
The corresponding reported hazard ratio for overall survival (OS) in these studies ranged from 56% to 70% of cases, and the concordant p-values ranged from 41% to 46% of cases. The conclusions of these studies suggest that comparative efficacy research often produces discordant results with those from randomized clinical studies(11).
Patients included in randomized clinical studies are often represented by a younger, better performance status group of individuals, also lacking major associated comorbidities compared to the general population presenting in oncology wards(12).
The result differences between randomized controlled clinical studies and comparative efficacy research could be a reflection of a different therapy effect on the healthier subjects in RCTs(13).
The characteristics of data collecting methods:
1. Observation is a systematic method. Observation is not random or unplanned. The length of observing periods, the intervals between them, the number of observations, the observing zone or situation and different techniques used for observation are carefully planned. Often, there is a systematic management for situation control if there are special factors planned to be studied. For example, the study of sport competitive spirit, honest behavior, leadership qualities, and so on.
2. Observation is specific. Observation is used not just for specific aspects of human behavior. Furthermore, observation is aimed at specific aspects of the total situation, presumed to be significative for the purpose of the study. This could be often overlooked, but the science observer should be trained to search for certain details that align with the purpose of the study, so that effort, time and money are not wasted.
3. Observation is objective. Observation should be objective and unbiased. Generally speaking, observation should be guided by a hypothesis. The observer must maintain ethical neutrality but, at the same time, he or she must maintain a flexible attitude, so that when a certain miscalculation inevitably happens, he or she can easily adapt.
4. Observation is quantitative. Although many important phenomena cannot be quantified, for their analysis is decisive to use specific means to quantify certain observations. Even quality must be converted to quality because this kind of data is also subjective, and quantitative data are objective and can be illustrated in an objective manner.
5. Observation is a matter of eyesight. P.V. Young states that observation is a systematic and deliberate study conducted through eyesight. An observer gathers data that have been seen with his or her own eyes. Information collecting through means of own’s eyesight is probably the most important technique of data collecting in social research.
6. Defined purpose. Observation must have definite purposes and objectives. These should be clearly defined before the process is started. Without the clear definition of purposes and objectives, observation would prove to be expensive and disorganized.
7. Observation enrolment is made without delay. Whilst the observation period is taking place, it is very difficult for the observer to remember every detail of said observation. Therefore, important data are easily lost. Human memory loss factor affects observational data entry, and so the observer must enroll all important data as soon as the observation is finalized.
8. Observation is certifiable. The results of the observation can be easily verified and validated. The observation is checked with usual norms of validity, viability and utility. It is possible to verify the results of the observation by comparing the results of different observers and reproducing the study(14).
Who or what defines the standard of care? Clinical studies versus real-world lung cancer patients
Some voices in medical world advocate that the rate of progress for lung cancer therapies is somewhat slow, because clinical studies take a lot of time to complete from the start. In the USA, only about 3% of patients with cancer are enrolled in clinical studies, and this number is even lower for lung cancer patients. The reasons behind this statistic are that a large number of patients do not have access to clinical studies without travelling significant distances, and another large number of patients might feel reluctant taking part in research studies. The latter might be explained by the abundance of magazine covers that picture a person inside of a cage, along with the title “Are you a guinea pig?” Another involved factor is the fact that some patients are ineligible for clinical studies. More recent research has compared the standard of care in clinical trials with the standard of care in real world. For example, a retrospective study from Germany has tried to formulate real-world data regarding the overall survival of patients diagnosed with advanced lung carcinoma, whilst listing the benefits of new therapies(15).
The discovery of new molecular alterations and the development of new therapies to target these alterations have led to a major improvement versus conventional standard chemotherapy when applied to selected patient populations(6-11).
A recent meta-analysis regarding TKI inhibitors gefitinib, afatinib and erlotinib has stated that these three agents have surpassed chemotherapy from the perspective of progression-free survival (PFS), global response rate and disease control rate. The results regarding the functional system are yet less known(16-21).
Similar results have been revealed in another meta-analysis regarding only erlotinib(12).
By contrast, an observational German study conducted on patients with EGFR-positive NSCLC has described that patients treated with TKI have fared better compared to patients never treated with TKI, with higher OS (mean OS 18.4 versus 13.6 months; HR 0.53; p=0.003)(22).
Besides aforementioned agents, the recent development of immune checkpoint inhibitors, like nivolumab and pembrolizumab, also extends therapy options for advanced NSCLC patients.
Mean survival (OS mean) reported in clinical trials has been 9.2-12.2 months (nivolumab) and 10.4-12.7 months (pembrolizumab, patients with PD-L1+) versus 6-9.4 months (docetaxel – chemotherapy)(23,24).
On the other hand, Hon et al. report that patient populations deemed incompatible for immunotherapy/targeted therapy have received first-line chemotherapy up until January 2016, when pembrolizumab in first-line setting was approved for patients with PD-L1 score above 50%(25).
The overall survival prediction for patients ineligible for targeted therapy/immunotherapy remains dismal still. Based on recent therapy advances, German and European treatment guidelines recommend mutational testing (EGFR, ALK, ROS-1, MET, NTRK), as well as PD-L1 status, for identifying patients that are eligible for and could benefit after targeted therapy/immune checkpoint therapies(26-31).
As a resolution over novel therapy efficiency approved for use in advanced NSCLC, we restate the conclusions of a retrospective study. Although using immunotherapy in the first-line setting has risen in the UK during this study’s period, most patients have received chemotherapy in the first line. A survival benefit regarding immunotherapy in the first line was noted, but this has proven to be smaller than that reported in clinical studies. Targeted therapy was associated with the highest OS interval, underlying the necessity for better therapy options in tumors without targetable mutations(32).
Second-line systemic therapy for advanced NSCLC
An important issue for managing advanced and metastatic NSCLC is second- and third-line therapies, because at some point all patients progress after the first line. Controversy exists regarding refractory first-line palliative chemotherapy patients, and whether they could benefit or not from second line cytotoxic therapy. This situation was even more stringent when there was no immune checkpoint inhibitor therapy available. Almost 23-26% of patients presented with progressive disease and 6-8% of them died during the first-line chemotherapy(33-35).
If the patient is per se refractory to chemotherapy, things are not clear whether changing the chemotherapy will elicit a response; also, to note that the performance status usually decreases as the disease progresses over time. In the TITAN study, patients with NSCLC and progression during or right after chemotherapy (platinum doublets in the first line) were randomized to receive either eroltinib or chemotherapy (docetaxel or pemetrexed). A number of 424 (16.4%) were eligible for randomization. There was no difference between the two arms of the study and mean survival was approximately five months(36).
Anti-PD-L1 antibody therapy currently represents the backbone of immunotherapy in advanced NSCLC and could lead to impressive response rates and to durable disease remission, but only in a subgroup of patients. ICI have become the new standard of care, based upon positive responses from randomized controlled studies with immune checkpoint inhibitors versus chemotherapy in second- and third-line settings, with progression after platinum doublet in the first line(37-41).
The issue with second-line therapy efficiency has become even more important. Albeit substantial improvement of prognosis by using ICI in the first line has been noted, a significant number of patients are still refractory to first-line therapies. In randomized controlled studies, this ratio ranged from 3% to 13.3% under chemoimmunotherapy combined(42).
In the last decade, regulatory authorities, like FDA and EMA, have approved a significant number of novel therapies for advanced NSCLC treatment, especially immunotherapy agents and targeted therapies. Observational retrospective studies have been published to evaluate the safety and efficacy of second-line and subsequent line in the real-world setting(43).
Many of these studies have reached inferior results regarding safety and survival compared to pivotal studies. This is explained largely because pivotal studies were designed with strict inclusion rules. Among exclusion criteria from the studies are ECOG PS below 2, patients without CNS involvement (brain metastases), or the presence of autoimmune or infectious diseases (hepatitis B or C). Even more, the average age in clinical studies is usually smaller than the average age of the presenting patients in hospitals and clinics. All these factors hinder randomized controlled studies’ ability to reflect the entire population diagnosed with a certain cancer. But even so, results obtained from real-world data studies tend to confirm an improvement of safety and efficacy regarding chemotherapy. In the existing literature, the most studied immune checkpoint inhibitor is nivolumab. In a prospective study including 1420 patients with advanced NSCLC, Barlesi et al. confirmed the efficacy and safety of nivolumab stated in clinical studies. This study took place in a real setting in France and included a large percentage of advanced NSCLC patients with ECOG≥2 (17.1%) and central nervous system metastases (19.9%)(44).
In a multicenter study with atezolizumab, having enrolled 152 patients with advanced NSCLC, Fururya et al. attested good safety and efficacy profiles. These results have been obtained regardless of intensely treated patients and/or performance status ECOG=0 (the latter being a favorable predictive factor)(45).
Whilst a small number of publications have investigated the safety and efficacy of monotherapy with atezolizumab, in clinical practice the results between anti-PD-1 antibody nivolumab and anti-PD-L1 antibody atezolizumab have been compared. Ramagopalan et al. have studied these two antibodies on a significant number of patients, comparing efficacy regarding overall survival(46).
Third and subsequent line of therapy
Improvements in clinical results make the second, third and subsequent lines of therapy a reality for a growing number of patients. A systematic review has evaluated therapy methods and clinical results from real world for patients receiving second- and third-line therapies for advanced NSCLC. In this analysis, approximately 30% of the included patients have received a third-line of therapy. Treatment decision was based on age, performance status, comorbidities, previous therapies, molecular and safety profiling from anterior lines and patient’s own preference. Chemotherapy (50%) and targeted therapy (40%) were most used among third-line regimens. Docetaxel, gemcitabine, vinorelbine, pemetrexed or erlotinib monotherapy were among the most frequent options. Four out of twelve studies included in this analysis have reported overall survival data in third-line setting. Mean OS (95% CI) from the beginning to the end of the third-line varied from 3.8 months (95% CI; 2.6-5.4) to 12 months (95% CI, 9.3-14.2)(47).
These being said, the best management approach and the third-line therapies’ role in this setting remain unclear. Currently, there are no standard of care or specific guidelines for systemic therapy for those patients that progressed on two or more therapy lines. There is also a paucity of phase II/III studies addressing this issue. Among these, some investigate targeted therapies like EGFR TKIs (osimertinib, erlotinib)(48,49) immune checkpoint inhibitors (durvalumab)(50) and next-generation antiangiogenic agents. Nevertheless, antiangiogenic agents play an important role in anti-cancer therapy. Tumoral angiogenesis is essential in development, invasion and metastatic dissemination of cancers. In the neoplastic angiogenesis pathway, there are involved molecular factors and different signaling mechanisms. Pro-angiogenic factors include vascular endothelial factor (VEGF), platelet derived growth factor (PDGF), fibroblast growth factor (FGF) and angiopoietins. VEGF is the most intensely studied factor, stimulating angiogenesis through activation of vascular endothelial growth factor receptor 2 (VEGFR-2), which is extensively expressed in NSCLC(51).
The inhibition of vascular forming in NSCLC therapy has used two main strategies: monoclonal antibodies that target VEGF (bevacizumab) or VEGFR (ramucirumab), and small molecule tyrosine-kinase inhibitors (nindetanib), that inhibit multiple proliferative and angiogenic pathways. Bevacizumab is approved for first-line use for non-squamous advanced NSCLC in combination with platinum chemotherapy(52). Ramucirumab and nintedanib are approved for use in many countries in second-line setting, combined with docetaxel for advanced NSCLC(53), respectively non-squamous NSCLC(54). The possible benefits of other small molecule TKI like anlotinib(55), apatinib(55) and fruquintinib are currently under investigation. Authorized drugs for use in Europe include atezolizumab, durvalumab, nivolumab and pembrolizumab, with slightly different therapeutic indications(57). During the study time (2016-2018), the main indication for ICI was for second- or third-line setting, post-progression after platinum doublet chemotherapy and targeted therapy, whichever was the case(58-60).
The European Medicines Agency (EMA) has approved nivolumab and atezolizumab for use regardless of PD-L1 status, in 2015 and 2017, respectively. Pembrolizumab was approved for use in advanced NSCLC therapy in 2016, but for tumors that express a TPS PD-L1≥1%(61,62).
In an Italian study that included unselected populations of patients diagnosed with advanced non-small cell lung cancer, anti-PD-1/PD-L1 therapy administered in any therapy setting line lowered the risk of death for up to two years since the diagnostic date, confirming the immunotherapy efficacy, outside of clinical trials(63).
Conclusions
Although randomized controlled trials are considered the standard in evaluating the treatment efficacy and safety of newly developed drugs, the results of these trials may be limited or partly contradicted in real medical practice. Observational studies evaluate the effectiveness of treatment in patients in everyday clinical practice. The results of these studies can confirm and extend the results reported in controlled and randomized clinical trials obtained for the carefully controlled population. Retroactive observational studies can use “real-world” data when they are recorded electronically or even on paper (more difficult). When they are prospective, they also use data from the patients’ files without influencing the usual protocols of doctors. Observational studies and real-world data have developed a lot in the last period and they mostly confirm the results from clinical trials, but sometimes not to the same extent, and other results from randomized clinical trials can be disproved.
Conflicts of interests: The authors declare no conflict of interests.