Clamparea întârziată la nou-născuţii din sarcină gemelară
Delayed cord clamping in newborn babies from twin pregnancy
Abstract
Multiple pregnancies are unique situations in which obstetricians and neonatologists may hesitate in performing the delayed cord clamping (DCC). The delayed clamping of the umbilical cord appears to be beneficial for the term newborn and also for the premature ones. Studies have shown that the prematurely born twins who received DCC required less transfusions and treatment with surfactant for respiratory distress syndrome (RDS) compared to the newborns for whom the precocious clamping of the umbilical cord was performed. DCC is feasible and safe for the twin pregnancies with dichorionic twins. The American College of Obstetricians and Gynecologists recommended (in 2020) the delayed umbilical cord clamping for at least 30-60 seconds after birth in vigorous term and preterm infants, the milking not being recommended, especially in very preterm babies (below 28 weeks).Keywords
delayed clampingnewborntwin pregnancyRezumat
Sarcinile multiple sunt situaţii unice în care medicii obstetricieni şi neonatologi pot avea o atitudine ezitantă privind efectuarea clampării întârziate. Clamparea întârziată a cordonului ombilical pare a fi benefică pentru nou-născuţi la termen, dar şi pentru prematuri. Studiile au arătat că gemenii născuţi prematur la care s-a efectuat clamparea întârziată au necesitat mai puţine transfuzii şi tratament cu surfactant pentru sindromul de detresă respiratorie (SDR), comparativ cu nou-născuţii la care s-a efectuat clamparea precoce a cordonului ombilical. Clamparea întârziată este fezabilă şi sigură la sarcinile gemelare cu gemeni dicorionici. Colegiul American de Obstetrică şi Ginecologie recomandă (2020) clamparea cordonului ombilical la 30-60 de secunde după naştere la nou-născuţii viguroşi la temen sau prematuri, mulgerea cordonului ombilical nefiind recomandată la nou-născuţii prematuri (sub 28 de săptămâni).Cuvinte Cheie
clampare întârziatănou-născutsarcină gemelarăIntroduction
At birth, the newborn is still attached to the mother through the umbilical cord, which is part of the placenta. It is subsequently separated from the placenta through the clamping of the umbilical cord.
Multiple gestations are unique situations in which the obstetricians and neonatologists may hesitate in performing the delayed cord clamping (DCC) due to the concerns related to the placenta, the vascular connections between the fetuses in case of monochorionic twins, the complications in case of the second twin, the difficulty of the extraction of the second twin during the caesarean section, due to the delay of the birth of the first child and the increased risk of postpartum hemorrhage.
The ideal moment to perform the DCC in multiple gestations is not known yet(2).
However, DCC promotes a lighter cardiopulmonary transition, especially in premature newborns, such as the case of the newborns from twin pregnancy(2).
The recommendation of the American College of Obstetricians and Gynecologists is that, in case of the second twin, a delay of the umbilical cord clamping should be performed for at least 30 to 60 seconds after birth, both in the vigorous and the premature newborn(1).
Materials and method
This is a general review. We performed a review of the currently available information in the PubMed database regarding the delayed cord clamping. The keyword for this search was “DCC”.
Results
The delayed clamping of the umbilical cord appears to be beneficial for the term newborns and also for the premature ones. For the term newborns, the delayed clamping of the umbilical cord increases the level of hemoglobin at birth and improves the iron deposits during the first few months of life, which may have a favorable effect on the results of the development. There is a slight enhancement of jaundice in this group of newborns. Consequently, at the maternities where delayed clamping of the umbilical cord is practiced in term newborns, the necessary devices should also be provided to monitor and treat neonatal jaundice.
Before the mid-1950s, the term precocious clamping was defined as the clamping of the umbilical cord within 1 minute after birth, and the late clamping was defined as the clamping of the umbilical cord in more than 5 minutes after birth(3).
Considering the benefits for most newborns, the American College of Obstetricians and Gynecologists now recommends a delay in the clamping of the umbilical cord in vigorous term newborns and also in premature newborns for at least 30-60 seconds after the birth. The ability to perform a delayed clamping of the umbilical cord may vary according to the maternity; the decisions under these circumstances are taken by the team handling the mother and the child.
Delayed cord clamping from 30 seconds until the last pulsation of the umbilical cord was supported by a series of governmental organizations(4).
The American College of Obstetricians and Gynecologists recommended a delay of 30-60 seconds in umbilical cord clamping for all preterm deliveries(5).
The Royal College of Obstetricians and Gynecologists also recommends deferring umbilical cord clamping for healthy term and preterm infants for 2-5 minutes after birth(5).
The World Health Organization recommends delayed cord clamping, defined as cessation of pulsations or 120-180 seconds, as the standard of care for infants who do not require resuscitation(5).
Several randomized controlled studies, cohort studies and meta tests were published about delayed clamping in premature newborns.
On the long run, a Cochrane review of 15 studies which involved 3911 women and pairs of newborns showed that DCC helps improve the hemoglobin and the levels of the postnatal hematocrit and decrease the iron deficiency from three to six months without increasing the percentage of maternal complications(7). The only disadvantage reported was the increased requirement for phototherapy.
Studies that compare the neonatal results in the first twin compared to the second one showed that the second twin presents a higher risk of morbidity if the Apgar score is low at birth; he presents asphyxia at birth, he requires resuscitation and intubation in the birth room, and he develops the respiratory distress syndrome or other neonatal complications which require admission to the neonatal intensive care unit (NICU).
Consequently, the second twin presents more neonatal complications, especially if he weighs less than1500 g and he is in noncephalic presentation(6).
Asphyxia at birth and respiratory distress syndrome have a major contribution in the increase of morbidity in the second twin(9,10).
The diminishing of the iron deficiency and the iron deficiency anemia may have a significant impact on the health of the children and on the neurodevelopment on the long term, not only in case of developing countries, where iron deficiency is higher, but also in the countries with high incomes(11).
A Swedish study noticed an improvement of the mild and social motor development in children aged 4 years old in which the DCC was performed more than 3 minutes after birth, compared to the ones in which clamping was performed immediately at birth(12).
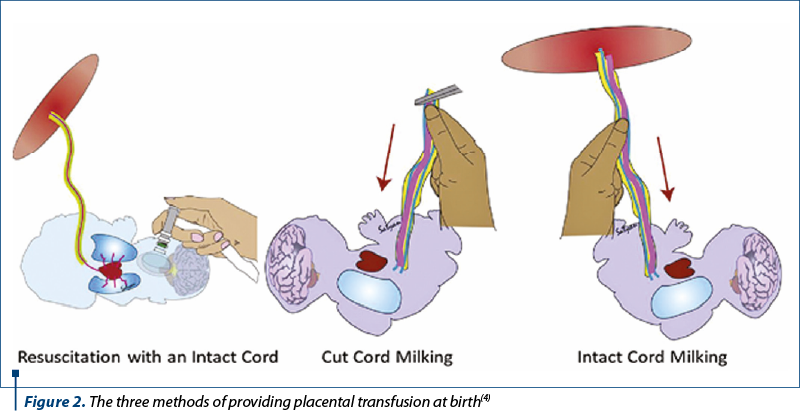
For premature newborn, the placenta transfusion, through DCC, improves the hematocrit levels and diminishes the need for blood transfusions. DCC diminishes the mortality in hospitals. In stable premature infants, DCC for more than 60 seconds, during which the child is placed at or below the level of the placenta and assuring the thermal comfort, may be attempted.
In premature infants, delayed clamping of the umbilical cord is associated with significant neonatal benefits, including improved transitional circulation, the establishment of a better volume of red blood cells, the decrease of the need for blood transfusion and the lower incidence of the necrotizing enterocolitis and intraventricular hemorrhage.
Delayed clamping of the umbilical cord was not associated with an increased risk of postpartum hemorrhage or increased loss of blood at birth and neither was it associated with a difference of the postpartum hemoglobin levels or the need for blood transfusion.
Monochorionic twins versus dichorionic
Monochorionic twins present a unique challenge to implementing DCC due to twin-to-twin transfusion syndrome (TTTS) complications and concerns about putting the second twin’s well-being at risk while performing DCC on the first one. Many studies excluded monochorionic multiples or a subset of those who fit the TTTS diagnostic criteria(6).
Studies have shown that premature born twins who received DCC required less transfusions and treatment with surfactant for respiratory distress syndrome compared to the newborns for whom the precocious clamping of the cord was performed(8).
Studies have shown that second-born twins have worse outcomes at almost every category compared with the first-born ones, including mortality, Apgar scores, respiratory distress syndrome, intubation and resuscitation(6).
One study showed that second-born twins had more neonatal complications, especially in infants with birthweight less than 1500 g and non-vertex presentation in the second twin(6).
Major contributors of morbidity in second twins were birth asphyxia and respiratory distress syndrome(9,10).
The biological sex has contributed to the first and second twin outcome discrepancy, with male second twins generally having worse outcomes than female second twins(10).
Umbilical cord milking
Intact umbilical cord milking (UCM) or milking of the attached cord refers to gentle grasping of the uncut umbilical cord and squeezing it toward the infant, usually for three or four times. The cord refills quickly (in about 2 seconds) and can be milked again. After three or four milkings of the cord, an infant receives about 17 ml/kg(4).
UCM provides a similar blood volume to a 2-minute delay in cord clamping in term infants, as measured by residual placental blood volume(4).
Discussion
What is already known?
Delayed clamping is beneficial for premature newborns.
Delayed cord clamping (DCC) is feasible and safe in twin pregnancies with dichorionic twins.
DCC has been shown to improve placental transfusion, leading to an increase in iron stores.
Practicing DCC – particularly in developing countries, where iron deficiency anaemia is relatively common – is a simple intervention that may improve the iron levels of the infants.
What is new?
Newborns from multiple gestations in which DCC is performed have similar results with those of the newborns from a unique pregnancy in which DCC was performed.
The second newborn from the twin pregnancy does not present more severe complications compared to the first newborn in which DCC was performed.
Delayed cord clamping is feasible in both monochorionic and dichorionic pregnancies.
Currently, the placenta transfusion should be considered in each case where the neonatal resuscitation is not necessary, because it may have an impact on the results of the newborns.
Bibliografie
- Stephen M, Chasen T, Chervenak FA. Twin pregnancy: labor and delivery, UpToDate. 2021.
- Ghirardello S, Mosca F. Delayed cord clamping in twin pregnancies: To do or not to do?. Neonatology. 2019;116(1):6–7.
- Sayed Ali DK, Talkhan HM. The role of delayed cord clamping in improving the outcome in preterm babies. Int J Pediatr Neonatol Prim Care. 2019;1(1):6–10.
- Katheria A, Hosono S, El-Naggar W. A new wrinkle: umbilical cord management (how, when, who). Semin Fetal Neonatal Med. 2018;23(5):321–6.
- Shirk SK, Manolis SA, Lambers DS, Smith KL. Delayed clamping vs milking of umbilical cord in preterm infants: a randomized controlled trial. Am J Obstet Gynecol. 2019;220(5):482.e1-482.e8.
- Jegatheesan P, Belogolovsky E, Nudelman M, Song D, Govindaswami B. Neonatal outcomes in preterm multiples receiving delayed cord clamping. Arch Dis Child Fetal Neonatal Ed. 2019;104(6):F575–F581.
- McDonald SJ, Middleton P, Dowswell T, Morris PS. Cochrane in context: effect of timing of umbilical cord clamping in term infants on maternal and neonatal outcomes. Evid Base Child Health. 2014;9(2):398–400.
- Prins RP. The second-born twin: can we improve outcomes? Am J Obstet Gynecol. 1994;170(6):1649–56.
- Armson BA, O’Connell C, Persad V, et al. Determinants of perinatal mortality and serious neonatal morbidity in the second twin. Obstet Gynecol. 2006;108(3 Pt 1):556–64.
- Arnold C, McLean FH, Kramer MS, et al. Respiratory distress syndrome in secondborn versus first-born twins. A matched case-control analysis. N Engl J Med. 1987;317(18):1121–5.
- Andersson O, Hellstrom-Westas L, Andersson D, Domellof M. Effect of delayed versus early umbilical cord clamping on neonatal outcomes and iron status at 4 months: a randomised controlled trial. BMJ. 2011;343:d7157.
- Andersson O, Lindquist B, Lindgren M, Stjernqvist K, Domellof M, Hellstrom-Westas L. Effect of delayed cord clamping on neurodevelopment at 4 years of age: a randomized clinical trial. JAMA Pediatr. 2015;169(7):631-8.

September-December 2021 Calendar
September-December 2021 Calendar...
Caracteristicile clinice ale nou-născuţilor cu sindrom de detresă respiratorie care au necesitat transferul cu ambulanţa la alte unităţi spitaliceşti
Adriana Nistor, Romina-Marina Sima, Liana Pleș, Anca Daniela Stănescu
Sindromul de detresă respiratorie (SDR) este o patologie critică importantă şi reprezintă o cauză semnificativă de morbiditate ş...
Tratamentul endodontic în sarcină
Irina-Maria Gheorghiu, Sânziana Scărlătescu, Loredana Mitran, George Nicola, Paula Perlea, Alexandru Iliescu, Mihai Mitran
Tratamentele stomatologice pe parcursul sarcinii reprezintă o situaţie cu care medicii dentişti se confruntă în mod frecvent. Pacienta însărcinată se prezintă la cabinetul stomatologic atât pentru manopere de restaurare ...
Complicaţii materne şi neonatale în sarcina gemelară obţinută spontan versus sarcina gemelară obţinută prin FIV
Ana Maria Măreşescu, Radu Vlădăreanu, Simona Vlădăreanu
Acest studiu a avut ca obiectiv identificarea complicaţiilor materne şi neonatale din sarcina gemelară obţinută spontan, comparativ cu sarcina gemelară obţinută prin tehnici de reproducere asistată (...
Sarcină gemelară obţinută spontan versus sarcină gemelară obţinută prin FIV/ICSI – review al literaturii
Ana Maria Măreşescu, Simona Vlădăreanu, Silviana Mănăilă, Andreea Radu
Sarcina gemelară reprezintă o provocare pentru echipa medicală, dat fiind riscul crescut de complicaţii materno-fetale, fiind cea mai frecventă formă de sarcină multiplă....