Diagnosticul prenatal al sindromului Jarcho-Levin
Prenatal diagnosis of Jarcho-Levin syndrome
Abstract
Jarcho-Levin syndrome includes a range of anomalies of the spine and ribs resulting in a short thorax and is frequently referred to in the literature as spondylocostal or spondylothoracic dysplasia. Our case was diagnosed prenatally using ultrasound and confirmed postnatally by the clinical evolution and the imagistic data (X-ray, magnetic resonance and computer tomography). Due to the rarity of this condition, there are a limited number of reports in the scientific literature and very few are diagnosed prenatal.Keywords
prenatal diagnosisspondylocostal dysplasiaJarcho-Levin syndromeabnormal vertebraeRezumat
Sindromul Jarcho-Levin include un grup de anomalii ale coloanei şi coastelor ce duc la un torace scurt şi este frecvent descris ca displazie spondilocostală sau spondilotoracică. Cazul nostru a fost diagnosticat ecografic prenatal şi confirmat postnatal de evoluţia clinică şi de rezultatele explorărilor imagistice (radiografie, tomografie computerizată, rezonanţă magnetică nucleară). Datorită rarităţii acestei patologii, există un număr limitat de raportări în literatura de specialitate şi foarte puţine cazuri sunt diagnosticate prenatal.Cuvinte Cheie
diagnostic prenataldisplazie spondilocostalăsindrom Jarcho-Levinanomalie vertebralăIn 1938, Saul Jarcho and Paul Levin described a syndrome that grouped severe anomalies of the spine and anomalies of the ribs resulting in a short thorax(1). Children with severe forms had frequent pulmonary complications (generated by the thoracic restriction) and had a high mortality in the first years of life. What clinicians presently include in Jarcho-Levin syndrome encompasses a range of diagnoses from spondylocostal dysplasia, spondylothoracic dysplasia to bizarre vertebral anomalies and multiple hemivertaebre(2,3). The disease is inheritable with both autosomal recessive pattern and autosomal dominant pattern. Due to the rarity of this condition very few cases are described prenatally, and from our knowledge no prenatal diagnosis has been reported in our country.
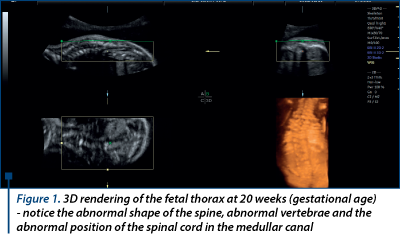
A patient of 23 years old with no prior obstetrical history presented in our department at 20 weeks for the sonographic anomaly screening. We noticed an abnormal shape of the spine, with abnormal vertebrae and an abnormal position of the spinal cord in the medullar canal. We did not notice any ribs anomaly and the cardio-thoracic ratio was normal. No additional anomaly except a single umbilical artery was noticed. Our diagnosis at this moment was: hemivertaebrae; suspicion of spina bifida oculta. We recommended kariotyping, but the patient refused the procedure for personal reasons. The patient came back at 30 weeks and the ultrasound revealed the same aspect of the spine we noticed at 20 weeks. Though no obvious abnormally shaped ribs were seen a shorter and slightly narrower thorax was noticed. After a careful review of existing literature we decided it was a form of Jarcho-Levin syndrome. Family was informed of the possibility that the child might have a rare disease with potential inherited component; hence it was important to know if any similar cases were ever recorded in the family history - an attentive anamnesis was conducted but none came up. Our recommendations were delivery in a tertiary center, MRI and genetic counseling postnatal.
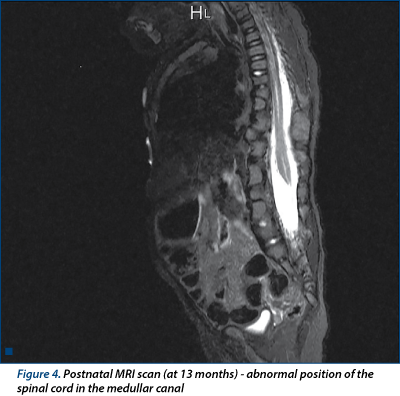
The baby was extracted by C-section at 39 weeks for an obstetrical indication unrelated to the baby’s condition. It was small for gestational age (2460 g), a condition frequently associated with single umbilical artery. The postnatal X-ray confirmed our suspicion that it was a form of spondylocostal dysplasia. In spite of the thoracic restriction, baby adapted well and was discharged after 6 days. Patient was referred to a radiology center where at the age of 13 months both CT and MRI were performed.They showed sever disorder of the vertebrae and ribs and abnormal position of the spinal cord in the medullar canal. The final diagnosis was spondylocostal dysplasia (Jarcho-Levin syndrome).
Discussion
Jarcho-Levin syndrome includes a large spectrum of spondylothoracic and spondylocostal dysplasias. Though the true frequency is no really known, about 400 cases have been reported in the literature(4). The groups’ characteristics include anomalies of the vertebrae and ribs - the anomalies of the vertebrae frequently include hemivertebrae and fusion of the vertebrae generating scoliosis and/or kyphosis aspect that we met in our case as well. The spine and ribs anomaly generate a thorax with limited expansion and have frequent respiratory problems(5,6,7). With postnatal growth, the need for a larger respiratory volume leads to a protrusion of the diaphragm towards the abdominal cavity and consecutively an increased abdominal pressure. As a result of this, patients frequently develop inguinal hernia - our patient also developed inguinal hernia that was operated on at nine months postnatal. To this moment four genes involved in spondylocostal dysplasias were discovered: DLL3, MESP2, LFNG and HES7 - they explain 25% of the diagnosed cases(8,9). The mechanism described is the alteration of the Notch signaling pathway which takes part in the somite segmentation(10). The result is malformation and fusion of the vertebrae and ribs as described by Jarcho and Levin. Prenatal diagnosis helps in counseling the parents and referring the case to tertiary centers for delivery. A special mention is deserved for the use of 3D ultrasound both for the diagnosis (as it offers a multi-angle approach of the pathology) and for the patient who finds the images more suggestive.


Acknowledgments: This paper was published under the frame of European Social Found, Human Resources Development Operationl Programme 2007-2013, project no. POSDRU/159/1.5/136893. The study was approved by Craiova University of Medicine and Pharmacy Ethics Comitee.
Bibliografie
Jarcho S, Levin PM. Hereditary malformation of the vertebral bodies. Bull Johns Hopkins Hosp 1938; 62: 216-26.
Van Der Sar. A Hereditary Multiple Hemivertebrae. Documenta de Medicina Geographica et Tropica. 1952; 4:23-8.
Lavy NW, Palmer CG, Merritt AD. A syndrome of bizarre vertebral anomalies. J Pediatr 1966; 69(6):1121–5.
Kulkarni ML, Sarfaraz Navaz R, Vani HN, Manjunath KS, Matani D Jarcho-Levin Syndrome. Ind J Pediat, 2006; 7:245-7.
Cornier AS, Ramirez N, Arroyo S, Acevedo J, Garcia L, Carlo S, Korf B. Phenotype characterization and natural history of spondylothoracic dysplasia syndrome: A series of 27 new cases. American Journal of Medical Genetics. 2004; 128 (2): 120–6.
Poor MA, Alberti OJR, Griscom NT, Driscoll SG, Holmes LB. Nonskeletal malformations in one of three siblings with Jarcho-Levin syndrome of vertebral anomalies. The Journal of pediatrics. 1983; 103 (2):270–2.
Karnes PS, Day D, Berry SA, Pierpont MEM. Jarcho-Levin syndrome: four new cases and classification of subtypes. Am J Med Gen. 1991; 40(3):264–70.
Bulman MP, Kusumi K, Frayling TM, McKeown C, Garrett C, Lander ES, Krumlauf R, Hattersley AT, Ellard S, Turnpenny PD. Mutations in the human delta homologue, DLL3, cause axial skeletal defects in spondylocostal dysostosis. Nature Genet 2000; 24:438-41.
Whittock NV, Sparrow DB, Wouters MA, Sillence D, Ellard S, Dunwoodie SL,Turnpenny P. D. Mutated MESP2 causes spondylocostal dysostosis in humans. Am J Hum Genet 2004; 74: 1249-54.
Lewis J, Hanisch A, Holder M. Notch signaling, the segmentation clock, and the patterning of vertebrate somites Journal of Biology 2009, 8:44, doi:10.1186/jbiol145.a.

Sarcina la adolescente - o problemă la nivel global
Daniela Stan, Mihai Mitran
S-a spus că numărul adolescentelor însărcinate atinge proporţii epidemice. Însă nu ne putem da cu adevărat seama de amploarea acestui fenomen dacă nu luăm în considerare impactul pe care îl are sarcina asupra adolescentei. În cel mai bun caz, viaţa ei va fi supusă unor schimbări majore, care îi vor marca pe e...
Refluxul vezico-ureteral congenital
Simona Vlădăreanu, Monica-Mihaela Cîrstoiu, Costin Berceanu, Claudia Mehedințu, Virgil-Ionuţ Mihoci
Refluxul vezico-ureteral (RVU), existenţa unui flux de urină retrograd orientat dinspre vezica urinară spre tractul urinar superior, este diagnosticat frecvent în contextul unei infecţii de tract urinar (ITU). Menţinerea...
Metodologia de achiziţie a plânsului nou-născutului
Elvira Brătilă, Diana-Elena Comandașu, Ştefan-Stelian Diaconescu, Mircea Sorin Rusu, Gheorghiţa Sardescu
Plânsul reprezintă iniţierea comunicării vocale umane, fiind cel mai important mijloc de transmitere a nevoilor şi dorinţelor sugarilor. Acest articol furnizează informaţiile necesare pentru proiectar...
Miopia – indicaţie de cezariană, mit sau realitate?
Ramona Barac, Monica Pop, Florian Baltă, Corina Taban, Simona Vlădăreanu, Claudia Mehedințu
Mulţi obstetricieni încă consideră că prezenţa patologiei oculare, precum miopia, decolarea retiniană, glaucomul sau diabetul la gravidă, reprezintă, o indicaţie de naştere asistată şi chiar de naştere prin cezariană. Co...
Infecţia cu Virusul Herpes Simplex în sarcină
Payam Behzadi, Elham Behzadi, Reza Ranjbar, Esmaiel Saberfar, Saeed Morovvati
Infecţia cu virusurile Herpes Simplex (VHS) reprezintă un grup complex de infecţii, care pot avea drept gazdă organismul uman. Există două tipuri de VHS: VHS-1 şi VHS-2. În cea mai mare parte din cazuri, infecţiile cu VH...