O analiză a fertilităţii, vârstei materne şi a sindromului Down la naştere în România: de ce contează un registru al sarcinii?
An analysis of fertility, maternal age and Down syndrome in Romania: why does a national pregnancy registry matter?
Abstract
Down syndrome (DS; trisomy 21) is the most common viable chromosomal anomaly to be diagnosed during pregnancy. The cases of trisomy 21 raise medical, familial and social consequences due to their development impact and associated malformations. The objective of this article is to analyze fertility, maternal age and the cases diagnosed with Down syndrome at birth in Romania, for a better understanding of the need of an effective national preventive healthcare system. Materials and method. We used a retrospective descriptive tabulation of data reported by the Romanian National Institute of Statistics and Eurostat. Results. In 2018, the average age at birth was 28 years old in Romania, compared to 30.58 years old in the European Union. The total number of pregnancies declined with an average annual rate of 3%, but the number of birth in women above 30 years old registered a steady growth. A decrease of DS cases at one million children between 2010 and 2015 (annual averages of 5.3%) for Romania was associated with a decrease in birth for women under 30 years old. Discussion. The number of DS cases at birth has decreased in the last decades, raising the question if the increasing costs led to an improvement in the prenatal screening diagnosis. New and often expensive tests have become available and widely prescribed. Understanding the impact of a national screening policy for Down syndrome in Romania is useful for rationale population-wide testing strategies. Nevertheless, a national pregnancy and birth registry, including pregnancy outcome and child surveillance corroborated with regular audit control, may contribute to allocate funds based on real needs.Keywords
Down syndromefertilitymaternal ageRomaniachildbirthRezumat
Sindromul Down (SD; trisomia 21) este cea mai frecventă anomalie cromozomială viabilă care trebuie diagnosticată în timpul sarcinii. Cazurile de pacienţi cu trisomie 21 ridică numeroase consecinţe medicale, familiale şi sociale, din cauza impactului asupra dezvoltării şi a malformaţiilor asociate. Obiectivul acestui articol este de a analiza fertilitatea, vârsta maternă şi cazurile diagnosticate cu sindrom Down la naştere în România, pentru o mai bună înţelegere a nevoilor unui sistem naţional de sănătate preventiv eficient. Materiale şi metodă. Am utilizat o tabulare descriptivă retrospectivă a datelor raportate de Institutul Naţional de Statistică din România şi de Eurostat. Rezultate. În 2018, vârsta medie la naştere se ridica la 28 de ani în România, comparativ cu 30,58 ani în Uniunea Europeană. Numărul total de sarcini a scăzut cu o rată medie anuală de 3%, dar numărul naşterilor la femeile de peste 30 de ani a cunoscut o creştere constantă. O scădere a cazurilor de SD la un milion de copii între 2010 şi 2015 (medii anuale de 5,3%) pentru România a fost asociată cu o scădere a naşterilor la femeile sub 30 de ani. Discuţie. Numărul cazurilor de SD la naştere a scăzut în ultimele decenii, ridicând întrebarea dacă fondurile alocate au dus la îmbunătăţirea screeningului prenatal. Testele noi şi în multe cazuri costisitoare devin disponibile şi prescrise pe scară largă. Înţelegerea impactului unei politici naţionale de screening pentru sindromul Down în România este utilă pentru fundamentarea strategiilor de testare la nivel de populaţie. Cu toate acestea, un registru naţional al sarcinii şi al naşterilor, inclusiv rezultatul sarcinii şi supravegherea copilului, coroborat cu un control periodic de audit, poate contribui la alocarea de fonduri pe baza nevoilor reale.Cuvinte Cheie
sindrom Downfertilitatevârstă maternăRomânianaştereDown syndrome (DS; trisomy 21) is the most prevalent and most commonly studied chromosomal abnormality. According to the European Commission, around 2.5% of the 5 million births registered by EUROCAT (European Surveillance of Congenital Anomalies) in the European Union have congenital anomalies(1). Eight percent of congenital anomalies at birth are represented by Down syndrome, meaning 1 to 1000 to 1 to 1100 live birth(2). In the United States of America, data from 2010 have reported an incidence of 1 to 792 live births(3), while in France: 23 to 10,000 (in the year 2005)(4). In many countries, registries have been used to prevent, to treat and to achieve targeted policies and healthcare planning for disease control programs, including Down syndrome registries(5-7).
Since 1990, in Romania, prenatal and postnatal diagnosis tests have become available, as well as centres for DS support and day-to-day parents support. Currently, data on the effectiveness of prenatal screening are scarce and are reported for single medical institutions(8-10), without a national level integrative analysis.
There are many reasons to analyze DS cases in Romania:
1) DS cases diagnosed during pregnancy have an important impact on the family, on the doctors and on society, due to associated intellectual disability, developmental delay and to congenital malformations.
2) Special healthcare needs at and after birth, that will continue during the entire life (the average lifespan of a person with DS is around 60 years old)(11,12).
3) To be able to evaluate the screening tests for Down syndrome, including ultrasound evaluation, biochemical markers and noninvasive prenatal tests.
The aim of this study is to understand the evolution of Down syndrome cases in Romania based on fertility indicators (such as the number of births and maternal age) and to discuss the effectiveness of the introduction of pregnancy registries in order to improve the detection and the follow-up in caring for Down syndrome persons.
Materials and method
A retrospective descriptive tabulation of data reported by the Romanian National Institute of Statistics and Eurostat was done(1,13). Data are presented for the total number of pregnancies, maternal age at birth, mean age of women at childbirth, number of births by mother’s age, number of cases of Down syndrome at birth, number of reported congenital malformations at birth, prevalence of Down syndrome at 10,000 total births, and number of performed ultrasound tests for the screening of malformations. Trend data for 2007 through 2016/2019 are presented for selected indicators.
The data are presented for Romania beginning with 2007 (the year when Romania joined the European Union).
Results
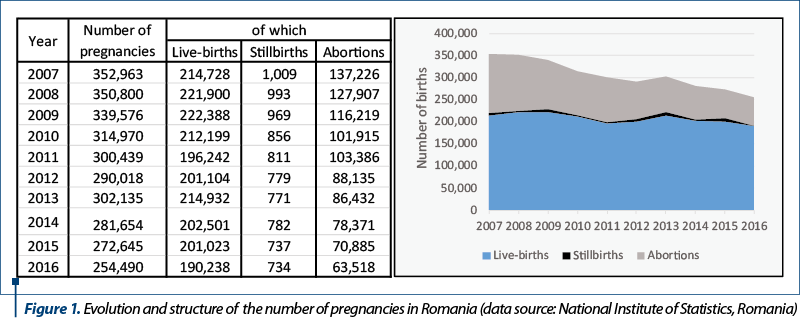
The total number of pregnancies declined in Romania in the last decade, with an average annual rate of 3%. A total of 63,518 abortions were registered in Romania in 2016, down with 54% from 2007. The number of stillborn pregnancies declined by 27%, and the number of pregnancies fell by 11% in the same analysis period. The number of live births decreased in Romania, but the trend is reverse for women above 30 years old, where the birth increased with an annual average of 2% (from 65,458 in 2007 to 82,640 in 2019). The Down syndrome birth decreased by 39.8% (down to 106 cases) in 2015 compared to 2010 and the number of births with congenital malformation decreased to 6387 cases in 2015 (-41.3%).
The main demographic trends in Romania show a sharp decrease in the number of pregnancies at the national level, contributing to the population ageing.
The total number of pregnancies has declined in Romania over the last decades, up to a 21st century minimum level of 255,000 pregnancies. The number of stillbirths and abortions decreased as well. The decrease can be observed both in absolute and relative terms – as the number of abortions decreased by 53.7% in 2016 compared to 2007 (an annual average decrease rate of 8.2%) and the number of stillbirths declined by 27.3% (an annual average decrease of 3.47%). Moreover, the percentage of abortions in the total number of pregnancies decreased from 38.9% in 2007 to 25% in 2016 (Figure 1).
Both the European Union and Romania follow a similar steady increasing trend in the average age of women at childbirth, with a gap of around 3 years (Figure 2). In Romania, the average age at birth was 28 years old in 2018, up from 26.8 years old in 2007, whereas in the EU the average age of women at childbirth increased from 29.7 years old in 2007 to 30.6 years old in 2018

One of the contributors to the lower birth age in Romania, aside from some cultural values, especially in the rural area, is the percentage of teenage mothers. Romania occupies the first place in the European Union regarding the proportion of first children to mothers aged less than 20, with a whopping 12% compared to a 4% EU average(1).
The number of live births decreased in Romania, but a breakdown by mother’s age group at birth reveals two different trends. The general negative trend is triggered exclusively by the decrease in birth for women under 30 years old, whereas the number of births in women above 30 years old registered a steady growth throughout the analysis period (Figure 3).

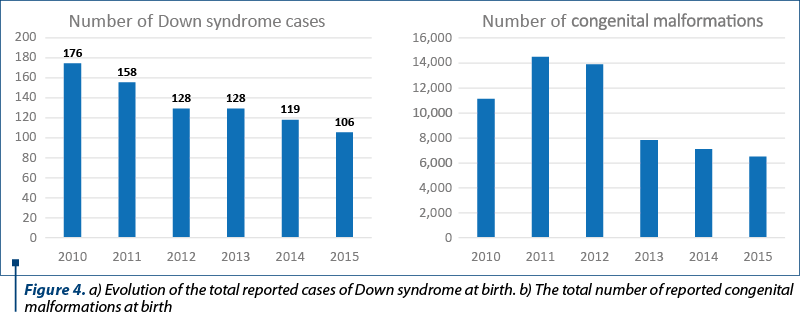
In Figure 4 we calculate that in Romania the Down syndrome births registered a decrease from 176 cases in 2010 to 106 cases in 2015 (-39.8%). Similarly, the number of births with congenital malformation decreased from 10,881 cases in 2010 down to 6,387 cases in 2015 (-41.3%). The trends display some irregularities, with some years with increases in the number of Down syndrome and congenital malformations and others with sharp decreases.
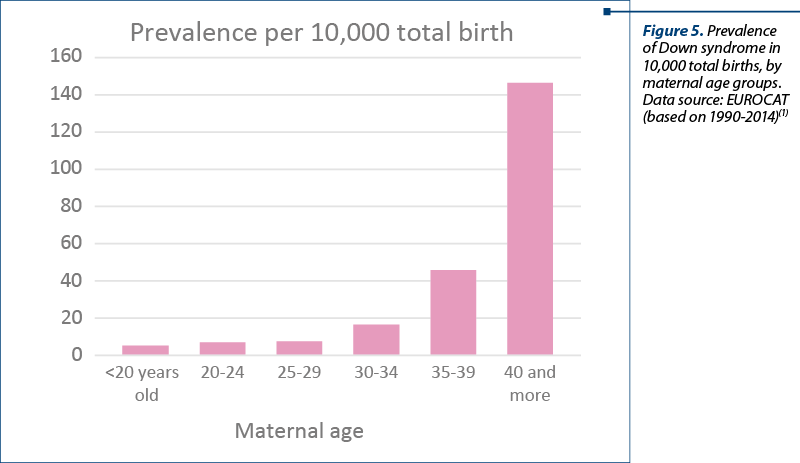
According to the EUROCAT study, based on 23 registries from different countries, the prevalence of DS is positively correlated to the maternal age – the highest prevalence can be observed in older mothers. Moreover, according to the same study, the overall increase in DS prevalence in the last decades can be linked to the increase in the average maternal age.
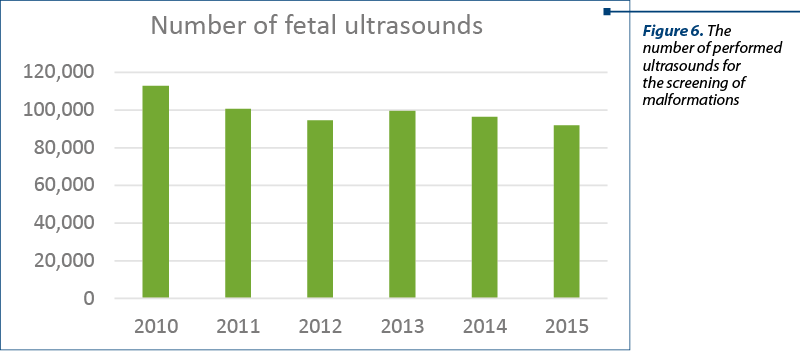
Between 2010 and 2015, the total reported ultrasound tests for screening examination decreased by an annual average rate of 3.1%, from 112,700 ultrasounds in 2010 down to 92,000 in 2015.
Discussion
The mother’s age at birth increased in Romania, as well as in most of the EU countries. The analysis shows an increase in the number of births in women over 30 years old. As a result, we expected to see more cases of Down syndrome since we know the positive association between the two indicators(14,15). The statistical data analysis shows a decrease in the number of DS cases at birth, but there are no data available on the real number of cases diagnosed during pregnancy. The screening for Down syndrome by the first-trimester combined tests, second-trimester ultrasound, invasive and non-invasive prenatal tests (NIPT) is currently used and may explain the decrease in DS cases.
In Romania, most couples elect for termination of pregnancy after the diagnosis of a Down syndrome baby, because the malformation is still culturaly seen as a pathological syndrome, something to be avoided. Nevertheless, there are also parents electing to continue a pregnancy after learning their child has Down syndrome – in many cases due to religious reasons. The Romanian Penal Code allows the therapeutic termination of pregnancy in case of diagnosis before 24 weeks of pregnancy. Nonetheless, at the hospital level, the termination of pregnancy for Down syndrome is statistically registered as abortion on request, without specifying the diagnosis. The decrease in the number of registered ultrasounds for screening examination may be explained by the fact that women may attend scan screening in a private setting (which does not report data); some women have no scans during pregnancy, others, because they refuse or have restricted healthcare access, such as lack of healthcare insurance or lack of specialists in the geographic areal.
A study on 530 postpartum women about the prenatal diagnosis of Down syndrome in Romania in 2016 found that 48.1% of the participants had never heard about tests for Down syndrome, and 88% of participants were classified as lacking knowledge(16).
Moreover, even though the statistical data on the screening and performance of tests in the first and second trimesters are reported, there is a lack of standardization that raises questions on the comparability(8-10). The Romanian Society of Ultrasonography in Obstetrics and Gynecology recommends the use of the Fetal Medicine Foundation protocol for assessing the risk of Down syndrome in the first trimester of pregnancy(17), with a free choice about the existing software risk calculation packages (Prisca, FMF) and the screening report.
Many public hospitals are choosing to screen or karyotype for Down syndrome, and the biochemical markers (HCG and PAPP-A), along with the screening ultrasound and karyotype are reimbursed by the National Health Insurance House of Romania. However, screening or testing is a challenge most hospitals have faced, due to limited places and budget.
The application of first- and second-trimester combined screening for Down syndrome and aneuploidies could be improved by the implementation of standardized national protocols and guidelines. Also, a collaboration between medical units, internal audit control and learning improvements may contribute to elaborate a strategy for prevention and treatment, and – why not – it will be appreciated more by patients and doctors. Nevertheless, a national pregnancy and birth registry, including pregnancy outcome and child surveillance, corroborated with regular audit control, may contribute to allocate funds based on real needs.
In conclusion, the first step in understanding the prevalence and the impact of DS pregnancies on the Romanian society is to introduce a national pregnancy registry. Comprehensive statistical data will allow the construction of a scientific framework that will support the understanding of the medical needs of pregnant women, as well as the needs of the Down syndrome population in Romania.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
EUROCAT Data. Available at: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data_en (accessed Aug 2020).
-
Health Line. Down Syndrome: facts, statistics and you. Available at: https://www.healthline.com/ health/down-syndrome/down-syndrome-facts (accessed Jan 2020).
-
De Graaf G, Buckley F, Skotko BG. Estimation of the number of people with Down syndrome in the United States. Genet Med. 2017;19(4):439-47.
-
Rousseau T, Amar E, Ferdynus C, et al. Variations in the prevalence of Down’s syndrome in the French population between 1978 and 2005. J Gynecol Obstet Biol Reprod (Paris). 2010;39(4):290-6.
-
Glivetic T, Rodin U, Milosevic M, Mayer D, Filipovic-Grcic B, Seferovic Saric M. Prevalence, prenatal screening and neonatal features in children with Down syndrome: a registry-based national study. Ital J Pediatr. 2015;41:81.
-
Boyd PA, Devigan C, Khoshnood B, et al. Survey of prenatal screening policies in Europe for structural malformations and chromosome anomalies, and their impact on detection and termination rates for neural tube defects and Down’s syndrome. BJOG. 2008;115(6):689-96.
-
Zhu JL, Hasle H, Correa A, et al. Hospitalizations among people with Down syndrome: a nationwide population-based study in Denmark. Am J Med Genet A. 2013;161A(4):650-7.
-
Nemescu D, Bratie A, Mihăilă A, Navolan D, Tănase A. First trimester combined screening for fetal aneuploidies enhanced with additional ultrasound markers: An 8-year prospective study. Ginekol Pol. 2018;89:205–10.
-
Rădoi V, Bohîlţea CL, Bohîlţea RE, Albu D. Cell free fetal DNA testing in maternal blood of Romanian pregnant women. Iran J Reprod Med. 2015;13:623–6.
-
Simionescu AA, Stănescu AMA. Missed Down Syndrome Cases after First Trimester False-Negative Screening-Lessons to be Learned. Medicina (Kaunas, Lithuania). 2020;56(4):199.
-
Bittles AH, Glasson EJ.Clinical, social, and ethical implications of changing life expectancy in Down syndrome. Dev Med Child Neurol. 2004;46(4):282-6.
-
Esbensen AJ. Health conditions associated with aging and end of life of adults with Down syndrome. Int Rev Res Ment Retard. 2010;39(C):107-26.
-
TEMPO online.INSSE. Available at: http://statistici.insse.ro:8077/tempo-online/ (accessed Jan 2020).
-
Maternal age and Down’s syndrome. Lancet. 1978;312(8079):P24-25.
-
Thompson JA. Disentangling the roles of maternal and paternal age on birth prevalence of down syndrome and other chromosomal disorders using a Bayesian modeling approach. BMC Med Res Methodol. 2019;19(1):82.
-
Pop-Tudose ME, Popescu-Spineni D, Armean P, Pop IV. Attitude, knowledge and informed choice towards prenatal screening for Down Syndrome: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):439.
-
SROG. Clinical Guidelines. Available at: http://sogr.ro/ghiduri-clinice (accessed on 1 January 2020)

May-September 2021 Calendar
May-September 2021 Calendar...
Actualităţi în investigarea prenatală a fătului folosind RMN-ul fetal
Erick George Neştianu, Cristina Brădeanu-Guramba, Radu Vlădăreanu, Simona Vlădăreanu
Rezonanţa magnetică nucleară (RMN) fetală reprezintă o unealtă modernă, care vine în ajutorul stabilirii diagnosticului în sarcinile la risc. Acesta reprezintă o examinare complementară ecografiei, demonstrându-şi a...
IRM – avantaje şi limite în diagnosticul şi tratamentul endometriozei
Cristina Vladu, Andreea Boiangiu, Elvira Brătilă, Radu Vlădăreanu
Endometrioza este o boală ginecologică multifocală comună, care se manifestă în timpul anilor de reproducere, cauzând adesea dureri pelviene cronice şi infertilitate. Poate apărea ca noduli şi aderenţe fibrotice periton...
Factori implicaţi în eşecul testării prenatale neinvazive prin ADN extracelular fetal
Sorin Vasilescu, Daniela Meca, Natalia Ţurcan, Monica-Mihaela Cîrstoiu
Diagnosticul prenatal neinvaziv, care are drept scop principal detectarea anumitor anomalii genetice fetale, este posibil datorită trecerii celulelor nucleate fetale în sângele matern. Este important de ştiut că există s...
Experienţa noastră în managementul gravidelor infectate cu SARS-CoV-2
Diana Cristina Secară, Ana Veronica Uzunov, Mădălina Daniela Banete, Maria Sajin, Monica-Mihaela Cîrstoiu
Infecţia cu SARS-CoV-2 în rândul pacientelor gravide reprezintă o nouă provocare în întreaga lume. Stabilirea unei modalităţi eficiente de a preveni infecţia cu noul tip de coronavirus poate du...