Spectrul de placentă accreta – o serie de trei cazuri dintr-un institut de îngrijire de nivel terţiar
Placenta accreta spectrum – a series of three cases from a tertiary care institute
Abstract
Placenta accreta spectrum is a potentially fatal condition and its incidence has been increasing worldwide in the last few decades. Although the overall reported incidence is low, we still encounter such patients not infrequently. It is one of the most difficult scenarios to manage for any obstetrician even in tertiary care setups. In this article, we describe a series of three such patients managed in a time span of six months, with case history, comparative characteristics and a review of current knowledge. Lastly, we have included a few recommendations based on our experience which we hope that will be helpful to all obstetricians managing such cases.Keywords
obstetriclaborplacentaincretaRezumat
Spectrul de placentă accreta este o condiţie medicală cu potenţial fatal şi cu o incidenţă în creştere în ultimele decenii. Deşi incidenţa globală raportată este mică, încă întâlnim cazuri, şi nu rareori, fiind unul din cele mai dificile scenarii de manageriat pentru orice obstetrician, chiar şi în unităţi de îngrijire terţiare. În acest articol, descriem o serie de trei cazuri, gestionate într-un interval de timp de şase luni, alături de istoricul pacientelor, caracteristicile comparative şi de un review al cunoştinţelor actuale în domeniul acestei patologii. În încheiere, am inclus câteva recomandări bazate pe experienţa noastră, care sperăm că le vor fi de ajutor obstetricienilor care îngrijesc asemenea cazuri.Cuvinte Cheie
obstetricătravaliuplacentăincretaIntroduction
Placenta accreta spectrum (PAS) represents a group of disorders where the abnormal pathomorphology of the placenta causes it to be either morbidly adherent to, or invade the uterine myometrium. It is one of the most challenging cases ever faced by any obstetrician and is responsible for potentially life-threatening peripartum hemorrhage and hysterectomies worldwide. In this article, we describe a series of three such cases managed by us at the Sri Shankaracharya Institute of Medical Sciences, Bhilai, India, which is a tertiary care medical college and hospital, within a time span of six months (October 2021 – March 2022).
Case 1
A 23-year-old patient, G2P1L1A0, with previous caesarean, was diagnosed at 24 weeks with PAS by ultrasonography (USG). Ultrasonography showed anterior low-lying placenta, with multiple vascular lacunae within the placenta, with reduced retroplacental thickness of myometrium. The Doppler showed turbulent lacunar flow. The findings were confirmed by repeated USG at 30 weeks and by MRI at 32 weeks. MRI showed intraplacental bands on T2-weighted imaging with the disruption of zone between uterus and placenta. The patient was taken for elective caesarean section at 35 weeks and 4 days. Preoperatively, the patient received two units of PRBC for anemia correction (Hb = 8 g%). Two doses of betamethasone (12 mg) were given at 24 hours apart for fetal lung maturity.
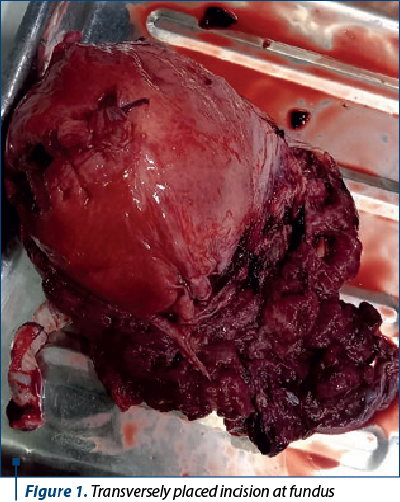
Caesarean section was done by midline vertical incision. After entering the abdomen, placenta was seen encroaching anteriorly up to the mid uterine segment. A transverse incision was made at the fundus to avoid the placenta. A single live female baby was delivered by breech extraction. After cord clamping, total hysterectomy was planned. Prophylactic tranexamic acid i.v. (1 g) was given in anticipation of bleeding. Bilateral uterine and internal iliac arteries were ligated, followed by hysterectomy (Figure 1). Hemorrhage checklist was maintained and the patient was given the required amount of packed cells, plasma and platelets. As hemostasis was satisfactory, abdominal drain was not placed. The total operative time was 90 minutes.
Postoperatively, the patient was monitored in high dependency unit (HDU) and received antibiotic coverage – ceftriaxone, metronidazole and amikacin. The postoperative period was uneventful. The catheter was removed after 48 hours and the patient was discharged on the sixth day postoperatively. Subsequently, placental specimen showed placenta increta on histopathology.
Case 2
A 36-year-old patient, G4P2L2A1, with two previous caesareans, was diagnosed with PAS at 30 weeks, in a government rural hospital and referred to our hospital. The diagnosis was confirmed by USG and MRI, and elective caesarean was planned. Preoperatively, anemia correction was done and the patient received a course of corticosteroids.
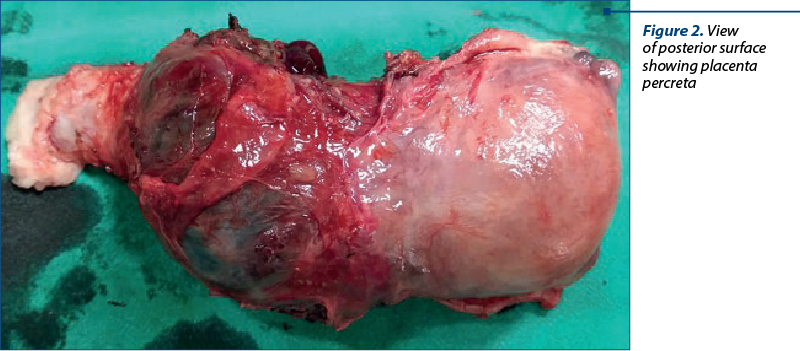
The patient was taken for elective caesarean section at 34 weeks and 3 days. Vertical incision was given. On entering the abdominal cavity, the placenta was seen in the lower uterine segment, involving the uterine serosa. A transverse incision was made two fingers width above the placental margin. As the baby was in longitudinal lie with breech presentation, the cephalic extraction of a live female baby was performed. The placenta was left in situ and uterine closure was done. Prophylactic tranexamic acid was given. Urinary bladder was found densely adhered to the lower uterine segment and the separation of bladder resulted in tear in the bladder which was repaired. Hysterectomy was completed after prior ligation of bilateral uterine and internal iliac arteries (Figure 2). Abdominal drain was placed and the patient was monitored in HDU postoperatively. She received multiple transfusions and antibiotics. The total operative time was 140 minutes.\
On the second postoperative day, the patient had two spikes of fever with symptoms of dysuria. Urine culture revealed an infection with E. coli and the patient was treated with a single dose of oral fosfomycin (3 g). The catheter was removed on the seventh day and the patient was discharged the day thereafter. The histopathology of placental specimen showed features of placenta increta with focal areas of placenta percreta.
Case 3
A 32-year-old patient, G3P1L1A1, with anterior low-lying placenta, was referred from a district hospital at 37 weeks with vaginal bleeding. Urgent USG was done which confirmed PAS. The patient had received antenatal corticosteroids before referral. One unit of packed RBC transfusion was done (Hb = 9.8 g%).
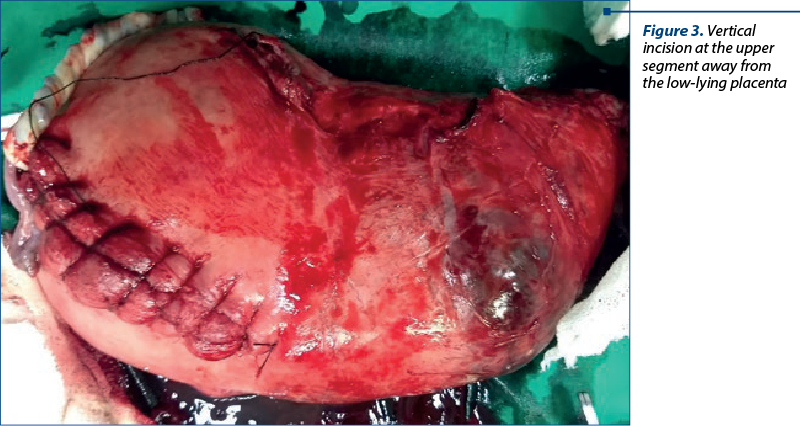
The patient was taken for emergency caesarean section. The abdomen was entered by vertical midline incision. Placenta was seen low lying. Vertical incision was made at the upper segment. A breech extraction of a live healthy male baby was done. After cord clamping, the uterus was closed using Vicryl. Subsequently, total hysterectomy was done after the ligation of bilateral internal iliac artery (Figure 3). The patient received three units of PRBC and plasma each intraoperatively. The operative time was 105 minutes. Abdominal drain was placed.
Postoperatively, the patient was managed in the HDU and received another unit of PRBC and two units of FFP. She was discharged on the seventh postoperative day. The specimen of placenta sent for examination showed features of placenta increta on HPE.
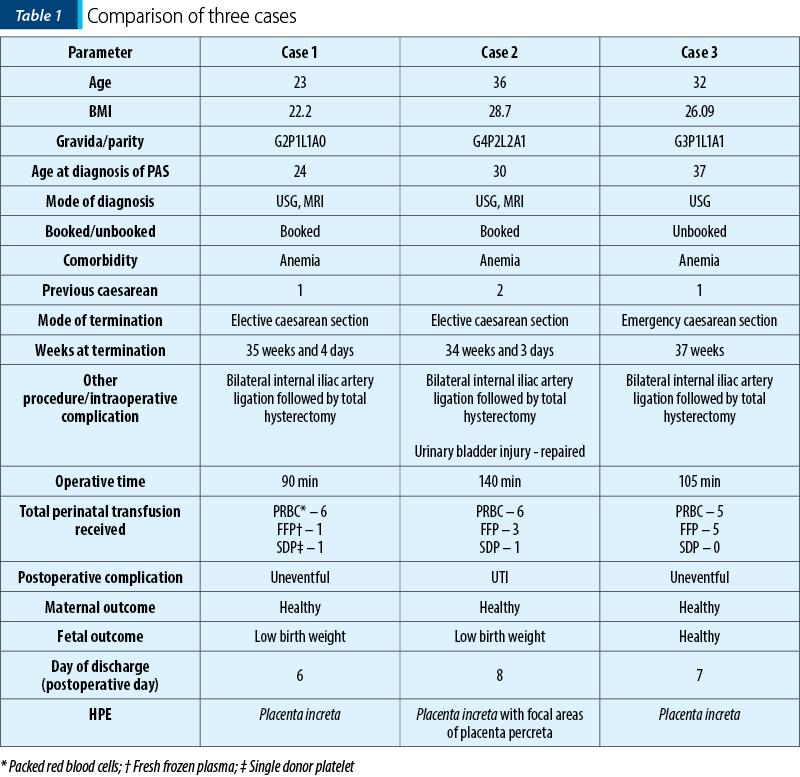
The summary of the three cases can be compared in Table 1.
Discussion
Placenta accreta spectrum is defined as an abnormal and pathological adherence of the placenta along with features of invasion of the myometrium(1), being one of the most difficult scenarios for any obstetrician to manage. While classically its incidence was reported as about one in one thousand(2), its current incidence is increasing worldwide, the involved factors being represented by increased frequency of previous caesarean sections(3) and placenta praevia(1). On the other hand, hypertension in pregnancy may be associated with a lower incidence of placenta accreta, although it needs more corroboration(4). PAS is a considerable cause of maternal mortality and morbidity and its increasing incidence in recent years has led to a significant attention from the clinical and scientific community worldwide.
The severity of PAS varies according to the depth of invasion of the chorionic villi into the myometrium(5). The least severe is the placenta accreta where the villi just adhere to the myometrium without any invasion, whereas in the most severe type (placenta percreta) the villi may invade up to the uterine serosa. The placenta increta is the intermediate form, where the villi invade the myometrium partially.
The antenatal diagnosis of placenta praevia is usually made in the second or third trimester. USG features of placenta accreta spectrum include abnormal absence of hypoechoic zone between placenta and myometrium, multiple vascular lacunae, thinning of retroplacental myometrium and extrauterine extension of the placenta(6). MRI is more sensitive than USG in detecting PAS and may be useful in cases of diagnostic difficulty by USG like posteriorly placed placenta or to assess the depth of invasion(7).
The main predicament in patients is represented by severe postpartum hemorrhage which is potentially life threatening, being recommended that the patients be managed in tertiary care referral centers with the availability of blood bank, along with adult and neonatal intensive care units(8). Except for rare cases where uterine preservation is a priority, caesarean hysterectomy is the management of choice. In a large study from a Norwegian center, with 96,313 patients, PAS was the main reason for patients undergoing hysterectomy(9). Strategies like the use of ureteric stents, internal iliac artery occlusion by balloon etc. have been advocated by some authors to facilitate the safe operation and to decrease the chances of massive perioperative hemorrhage(5,10).
In our series, one patient was diagnosed in the second trimester, while two patients were diagnosed in the third trimester. All had history of previous caesarean sections. All three underwent life-saving hysterectomy. The average operating time was 111.66 minutes and, on average, they required 5.6 units of packed cell transfusion. All the mothers were discharged in healthy condition, although two of the babies born had low birth weight.
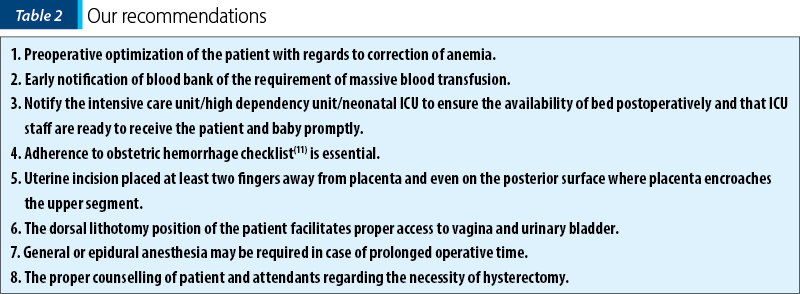
The salient points which we would like to emphasize particularly from our experience are presented in Table 2.
Conclusions
Placenta accreta spectrum is a serious and life-threatening obstetric condition. With a gradually increasing incidence over the last several decades, it is essential that there is an implementation of the proper protocol for managing such patients in all high-volume obstetrics centers. The proper training of healthcare personnel is also essential to ensure a good maternal and neonatal outcome.
Ethical approval. The manuscript was approved by institutional ethics committee.
Informed consent. The informed consent for publication was taken from all subjects for utilizing clinical information and images and that every effort will be made to keep information anonymous.
Funding: This research did not receive any funding from any sources.
Acknowledgement: None.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
-
Gloria C, Salvatore P, Francesco L, Anna GR, Francesco L, Chiara B, Gaspare C, Giuseppe C. Placenta Accreta Spectrum Disorder in a Patient with Six Previous Caesarean Deliveries: Step by Step Management. Case Rep Obstet Gynecol. 2021 Sep 12;2021:2105248. doi: 10.1155/2021/2105248.
-
Abotorabi S, Chamanara S, Oveisi S, Rafiei M, Amini L. Effects of Placenta Location in Pregnancy Outcomes of Placenta Accreta Spectrum (PAS): A Retrospective Cohort Study. J Family Reprod Health. 2021 Dec;15(4):229-235. doi: 10.18502/jfrh.v15i4.7888.
-
Kondoh E. Expectant Management of Placenta Accreta Spectrum Disorders. Surg J (N Y). 2021 Jun 3;7(Suppl 1):S2-S6. doi: 10.1055/s-0040-1722240.
-
Li L, Liu L, Xu Y. Hypertension in pregnancy as a risk factor for placenta accreta spectrum: a systematic review incorporating a network meta-analysis. Arch Gynecol Obstet. 2022 Apr 12. doi: 10.1007/s00404-022-06551-y. Epub ahead of print.
-
Roziana R, Kamarul Azhar K, Lau JH, Aina MAA, Nadia R, Siti Nordiana A, Mohd Zulkifli K. Morbidly adherent placenta: One-year case series in a tertiary hospital. Med J Malaysia. 2019 Apr;74(2):128-132.
-
https://www.acog.org/clinical/clinical-guidance/obstetric-care-consensus/articles/2018/12/placenta-accreta-spectrum
-
D’Antonio F, Iacovella C, Bhide A. Prenatal identification of invasive placentation using ultrasound: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2013;42:509–17. doi:10.1002/uog.13194.
-
Cnota W, Banas E, Dziechcinska-Poletek D, Janowska E, Jagielska A, Piela B, Czuba B. “The Killer Placenta” – a threat to the lives of young women giving birth by cesarean section. Ginekol Pol. 2022 Feb 14. doi: 10.5603/GP.a2021.0235. Epub ahead of print.
-
Pettersen S, Falk RS, Vangen S, Nyfløt LT. Peripartum hysterectomy due to severe postpartum hemorrhage: A hospital-based study. Acta Obstet Gynecol Scand. 2022 Apr 7. doi: 10.1111/aogs.14358. Epub ahead of print.
-
Takeda S, Takeda J, Murayama Y. Placenta Previa Accreta Spectrum: Cesarean Hysterectomy. Surg J (N Y). 2021 May 25;7(Suppl 1):S28-S37. doi: 10.1055/s-0040-1721492.
-
https://www.acog.org/-/media/project/acog/acogorg/files/forms/districts/smi-ob-hemorrhage-bundle-hemorrhage-checklist.pdf

September-December 2022 Calendar
September-December 2022 Calendar...
Caracteristicile neonatale în malformaţiile cardiace congenitale – experienţa noastră
Daniela-Mariana Manea (Lascoschi), Romina-Marina Sima, Liana Pleș, Anca Daniela Stănescu
Introducere. Malformaţiile cardiace congenitale (MCC) reprezintă cel mai frecvent defect congenital, apărând la 1% până la 5% din nou-născuţii vii. Scopul acestui studiu a fost de a dezvălui car...
Localizare atipică a unui lipom
Alexandru Baroş, Florina Păuleț, Ana Veronica Uzunov, Diana Cristina Secară, Mihaela Iuliana Zaharia, Monica-Mihaela Cîrstoiu
Vulva reprezintă o localizare atipică pentru dezvoltarea unui lipom. Etiologia lipomului rămâne necunoscută, însă factori multipli au fost încriminaţi, precum obezitatea sau trauma. De asemenea, lipomul apare cel mai fre...
Importanţa alimentaţiei echilibrate înainte şi în timpul sarcinii
Heidrun Adumitrăchioaiei
Alimentaţia femeii însărcinate este o parte esenţială a sarcinii pentru o bună dezvoltare materno-fetală. Totuşi, se pare că între 20% şi 30% din totalul femeilor însărcinate la nivel mondial prezintă valori ale micronutrienţilor sub limitele normale. Statusul nutriţional matern preconcepţional şi în ti...
Donarea de organe neonatale – consideraţii etice şi criminalistice la graniţa dintre dramă şi speranţă
Valentin Varlas, Roxana Georgiana Borş, Vlad Dima, Andreea Velișcu, Claudia Mehedințu, Monica-Mihaela Cîrstoiu, Simona Vlădăreanu
Context. Donarea de organe de la nou-născuţi pentru transplant este un eveniment relativ rar, care necesită cunoaşterea corespu...