Combinaţie de agenţi imunoterapeutici utilizată în melanomul metastatic – prezentare de caz
Immunotherapy agents combination in metastatic melanoma – case presentation
Abstract
Malignant metastatic melanoma has an unfavorable prognostic, with an overall survival until recently of 8-12 months. Currently, the overall survival after using immunotherapeutic agents has reached 24 months. This case is important for understanding the possibilities of administering chemotherapy and immunotherapy successively, although we cannot make assessments regarding survival. This case demonstrates the possibility of obtaining a complete remission for the combination ipilimumab (IPI) plus nivolumab (NIVO) followed by chemotherapy. Therefore, this case could support the hypothesis regarding a good combination of immunotherapeutic agents administered after chemotherapy which increases the immunogenicity of tumor cells. Another peculiarity of this case is the onset, after the administration of IPI plus NIVO, of a third-degree toxicity which was completely remitted, and after that the patient received without any toxicity the subsequent chemotherapy of eight series of dacarbazine.Keywords
malignant melanomacomplete remissionimmunotherapyRezumat
Melanomul malign metastatic are un prognostic nefavorabil, cu o supravieţuire globală care până nu demult era de 8-12 luni. Actualmente, prin apariţia agenţilor imunoterapici, supravieţuirea globală a ajuns la 24 de luni. Cazul pe care îl prezentăm, deşi nu putem face aprecieri asupra supravieţuirii, este important pentru înţelegerea posibilităţii de a administra succesiv chimioterapia şi imunoterapia. Acest caz demonstrează posibilitatea obţinerii unei remisiuni complete prin combinaţia ipilimumab (IPI) plus nivolumab (NIVO) urmată de chimioterapie. De asemenea, acest caz susţine ipoteza unui răspuns bun al combinaţiei de agenţi imunoterapeutici administraţi după chimioterapie care ar creşte imunogenicitatea celulelor tumorale. O altă particularitate a evoluţiei cazului este apariţia, după prima administrare de IPI plus NIVO, a unei toxicităţi de gradul al III-lea care s-a remis complet şi a permis administrarea ulterioară de opt serii de dacarbazină.Cuvinte Cheie
melanom malignremisiune completăimunoterapieIntroduction
Melanoma, an aggressive form of skin cancer, resulted from the transformation of melanocytes into malignant cells, is responsible for most of the deaths related to skin cancer(1). The incidence rates for melanoma are increasing. In 2018, in Europe, melanoma was the fifth and eighth type of cancer, with more estimated new cases among females and males, respectively. Most of the melanomas are normally located in the skin, but other locations are possible: eyes, ears, gastrointestinal tract, leptomeninges and oral and genital mucous membranes(2). In Romania, according to the Globocan data, in 2018 we had 1107 new cases of skin melanoma and 438 deaths were related to this type of cancer.
We present a compelling case of a 69-year-old patient, diagnosed with skin melanoma, Clark IV level, in 2018 (pT3NxMx), with multiple metastases few months later after one month of treatment with alpha 2b interferon, which subsequently obtained complete remission after one pre-immunotherapy series of DTIC, one series of dual immunotherapy and 8 series of post-immunotherapy chemotherapy with DTIC. The patient was consulted, investigated, treated and followed-up in our department at the “Prof. Dr. Alexandru Trestioreanu” Institute of Oncology Bucharest, beginning with July 2018 until now.
Case presentation
M.I., aged 68 years old (at the diagnostic moment), was diagnosed in July 2018 with skin malignant melanoma on the right side of the abdominal wall.
The hereditary history doesn’t reveal data which could be correlated with his actual malignancy. From the personal pathological history, we mention a hypercholesterolemia and a chronic ischemic heart disease diagnosed many years ago.
Disease history
After surgical removal (July 2018), the histopathology was malign melanoma, Breslow index 3.8 (pT3a), Clark level IV. The following IHC results confirmed the histopathology.
The initial CT scan of the thorax, abdomen and head (1.08.2018) did not detect lung, liver, brain or other metastases, but highlighted a right axillary lymphadenopathy (sentinel node). The sentinel node procedure was performed after lymphoscintigraphy and was positive at right axillary and inguinal level.

On the 27th of August, 2018, the patient underwent surgical removal of the lymphatic block from the right armpit (diagnosed later on the HP bulletin as malignant metastasis) and large postsurgical scar excision from the right abdominal flank which proved to be free of malignant cells on the HP exam. The inguinal block was not identified during surgical intervention and was diagnosed as lymphangitis at this level.
The BRAF analysis was negative for 11 and 15 exons of the BRAF gene.
In November 2018, the patient received the available treatment at that time with Intron® (alpha 2b interferon), 6 doses of 5 millions IU at three days.
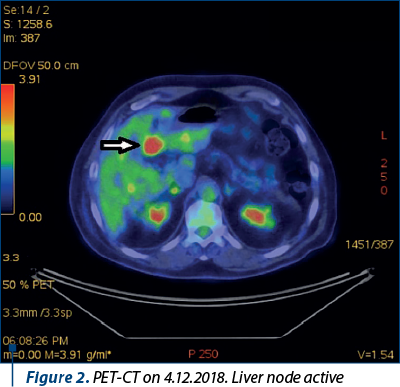
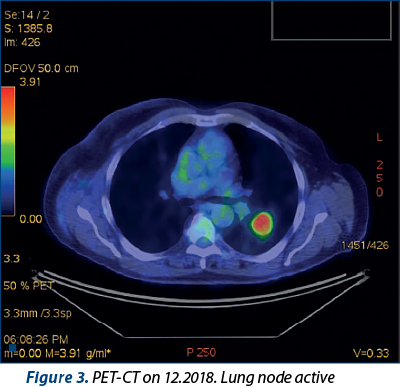
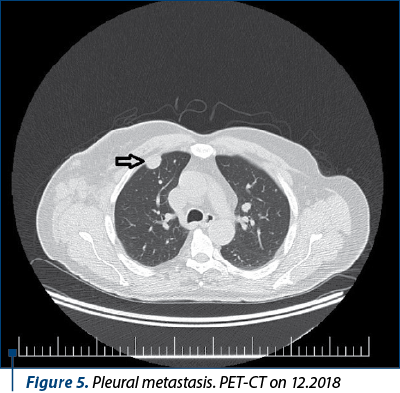
PET-CT scan from December 2018 revealed multiple metabolic active sites (bilateral pleural and lung nodules, lymph node block at the right armpit level, liver, bone and adrenal active nodes) – Figure 1. Head CT did not reveal the existence of metastases. A PET-CT performed on 4.12.2018 (Figures 1, 2, 3 and 5) revealed lung and liver metastases.
At that moment, the patient received chemotherapy with dacarbazine (DTIC). After this dose of chemotherapy, it was administrated the combination of ipilimumab (IPI) plus nivolumab (NIVO). The delay of administration of immunotherapy was due to the fact that in Romania we waited for the approval of immunotherapy with dual blockade, IPI plus NIVO.
After the first dose of IPI plus NIVO, the patient had a third-degree liver toxicity with high elevation of AST (837 U/L) and ALT (1086 U/L), which indicated an immune reaction of the liver of grade III CTCAE. We stopped the immunotherapy and administrated corticosteroid medication. The patient recovered his liver function, reaching normal values of liver enzymes.
In February 2019, due to the third-grade toxicity of the liver, we replaced the immunotherapy with chemotherapy with DTIC 1300 mg i.v., each cycle of 21 days.
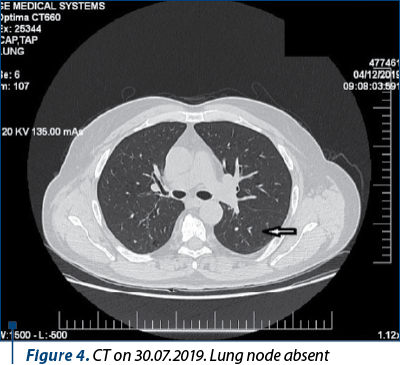
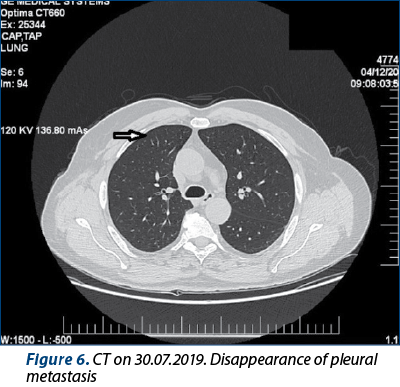
After eight series of DTIC, the CT scan from 30.07.2019 and the bone scintigraphy from 27.08.2019 revealed complete remission. Figures 4 and 6 reveal the disappearance of lung and pleural metastases. Unfortunately, we have no images that show the disappearance of the liver and bone metastases, but only an interpretation bulletin. The CT from July 2019 revealed the complete remission of pleural and lung metastases (Figures 4 and 6).
On 1st of August, 2019, the patient had the nineth and last series of DTIC.
The CT scan from 4.12.2019 corroborated with the abdominal MRI from 29.01.2020 (which infirmed a liver secondary lesion) showed no evolution.
Discussion
In the last years, the treatment strategy for advanced melanoma has progressed. New agents are significantly prolonging the survival of patients with advanced metastatic melanoma(3). These agents are part of targeted therapies – selective inhibitors of the oncogene BRAF and MAPK pathway directly, and immunotherapies – immune checkpoint inhibitors targeting cytotoxic T lymphocyte associated antigen-4 (CTLA-4) and PD-1, like ipilimumab and nivolumab(4). Before these two types of agents, patients with metastatic disease had a median survival between 8 and 12 months. Due to the use of these therapies, the survival period is now at least 24 months(3). Approximately 42-47% of the patients with BRAF mutations treated with targeted therapy have more than 3 years of survival, and 46-53% of the patients treated with immune checkpoint inhibitors have more than 4 years of survival(5).
Even when we compare the systemic immunotherapy that we used before with the new immunotherapeutic agents (CTLA4 and PDL1 inhibitors), we see a big difference in results. Thus, the first immunotherapeutic approaches were cytokine therapy, such as interferon alpha (IFN-a) and interleukin-2 (IL-2). Nonetheless, these agents were not associated with durable responses or enough improvements in survival for the most part of the patients. These therapies were also often associated with severe adverse effects (AEs) and toxicity(6,7).
Somewhat, the same results are reported with chemotherapy as a systemic therapy in advanced melanoma. This therapy is well tolerated, but has low response rates(7). An alkylating agent, dacarbazine (5-[3,3-dimethyl-1-triazenyl]-imidazole-4-carboxamide, or DTIC), is one of the agents used for advanced melanoma. A pooled analysis of 23 randomized, controlled trials showed that the objective response rate (ORR) for 1,390 patients receiving dacarbazine in monotherapy was 15.3%. The vast majority of these responses were partial (11.2% partial responses [PR] and only 4.2 % complete responses [CR])(8). The responses are rarely durable, fewer than 2% of patients treated with dacarbazine alone being alive at 6 years(9).
At our days, dual blockade of CTLA-4 and PD-1 was initially evaluated in a phase I study (CA209-004)(10). This study was amended to include the dose and schedule for nivolumab plus ipilimumab that was later evaluated in phase II (CheckMate 069) and phase III (CheckMate 067) randomized studies. Dual blockade of CTLA-4 and PD-1 improved antitumor response more than either agent alone. The objective response rate (ORR) with the dual blockade in the study CA209-004 was 40%, which was higher than that reported at the time for monotherapy with ipilimumab (11%) or nivolumab (28%)(11,12). In CheckMate 069, the combination led to a better ORR compared with ipilimumab (59% versus 11%)(13,14). Two-year OS rates in CheckMate069 were 64% for the dual blockade versus 54% for ipilimumab, although 62% of patients in the ipilimumab arm received anti-PD-1 treatment upon experiencing progression(14). CheckMate 067 also demonstrated significantly improved progression-free survival (PFS) and ORR for nivolumab plus ipilimumab, as well as nivolumab alone versus ipilimumab alone in patients with previously untreated advanced melanoma(15). At a follow-up of 36 months in CheckMate 067, the 3-year OS rates for nivolumab plus ipilimumab, nivolumab alone, and ipilimumab alone were 58%, 52% and 34%, respectively(16).
In a pooled analysis of randomized phase II and phase III trials of patients who received nivolumab 3 mg/kg plus ipilimumab 1 mg/kg, every 3 weeks with four doses, followed by nivolumab monotherapy 3 mg/kg every 2 weeks (n=409), the authors concluded that the efficacy outcomes seemed similar between patients who discontinued nivolumab plus ipilimumab treatment because of AEs during the induction phase and those who did not discontinue because of AEs. At a minimum follow-up of 18 months, the median progression-free survival was 8.4 months for patients who discontinued the treatment because of AEs during the induction phase and 10.8 months for the patients who did not discontinue because of AEs (p=0.97). The objective response rate was 58.3% for patients who discontinued because of AEs during the induction phase and 50.2% for patients who did not discontinue. The vast majority of grade 3 or 4 AEs occurred during the induction phase, with most of them resolving after appropriate management(17).
In another study, which evaluated the detailed toxic effects and time to treatment failure of patients with melanoma treated with nivolumab plus ipilimumab (intravenous nivolumab [1 mg/kg] and ipilimumab [3 mg/kg] administered every 3 weeks for up to 4 doses, followed by nivolumab [3 mg/kg] every 2 weeks or pembrolizumab [2 mg/kg] every 3 weeks until unacceptable toxic effects, disease progression or complete response), in a prospective cohort of 64 adults with advanced or unresectable melanoma, the authors observed a 91% incidence of clinically significant immune-related AEs, leading to frequent emergency department visits, hospitalizations and systemic immunosuppression, and they concluded that most patients do not tolerate four doses of nivolumab plus ipilimumab, but also that four doses may not be required for the clinical benefit. After a median follow-up of 14 months, there were 27 treatment failures (42%). In the group of 50 patients who were free of treatment failure at 12 weeks, it didn’t appear to be a difference in TTF between those who underwent treatment modification due to toxic effects (n=34) and those who did not modify the treatment for toxic effects(18).
Conclusions
This case argues for a complete remission, in the case of metastatic malignant melanoma, after a single administration of a combination of ipilimumab plus nivolumab. Prior administration of a dacarbazine dose could have a facilitating effect on the response to this combination of immunotherapeutic agents: cytotoxic T lymphocyte-associated antigen 4 inhibitor (ipilimumab) plus PD-1 inhibitor (nivolumab). Chemotherapy could make a (re)activation of tumor-targeting immune responses and can promote such responses to immunotherapeutic agents by increasing the immunogenicity of malignant cells.
Another aspect highlighted by this case is the acute third-degree toxicity (common toxicity criteria) which has completely recovered after stopping the immunotherapy and at the administration of a liver protector. But another problem is also whether the criteria for assessing cytostatic toxicity are applicable in case of immunotherapy.
The patient will be monitored for the duration of remission and survival, a challenge being the treatment indicated in a possible resumption of the disease evolution.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
- Swetter SM, Tsao H, Bichakjian CK, Curiel-Lewandrowski C, Elder DE, Gershenwald JE, Guild V, Grant-Kels JM, Halpern AC, Johnson TM, Sober AJ, Thompson JA, Wisco OJ, Wyatt S, Hu S, Lamina T, Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019; 80, 208–250, https://doi.org/10.1016/j.jaad.2018.08.055.
- Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio M, Gavin A, Visser O, Bray F. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018; 103, 356–387, https://doi.org/10.1016/j.ejca.2018.07.005.
- Ugurel S, Röhmel J, Ascierto PA, Flaherty KT, Grob JJ, Hauschild A, Larkin J, Long GV, Lorigan P, McArthur GA, Ribas A, Robert C, Schadendorf D, Garbe C. Survival of patients with advanced metastatic melanoma: the impact of novel therapies – update 2017. Eur J Cancer. 2017; 83, 247–257, https://doi.org/10.1016/j.ejca.2017.06.028.
- Rubin K. MAPK pathway-targeted therapies: care and management of uniquetoxicities in patients with advanced melanoma. Clin J Oncol Nurs. 2017; 21, 699–709, https://doi.org/10.1188/17.CJON.699-709.
- Ascierto PA, Capone M, Grimaldi AM, Mallardo D, Simeone E, Madonna G, Roder H, Meyer K, Asmellash S, Oliveira C, Roder J, Grigorieva J. Proteomic testfor anti-PD-1 checkpoint blockade treatment of metastatic melanoma with andwithout BRAF mutations. J Immunother Cancer. 2019; 7, 1–8, https://doi.org/10.1186/s40425-019-0569-1.
- Lugowska I, Teterycz P, Rutkowski P. Immunotherapy of melanoma. Wspolczesna Onkol. 2017; 2, 61–67, https://doi.org/10.5114/wo.2018.73889.
- Bhatia S, Tykodi SS, Thompson JA. Treatment of metastatic melanoma: an overview. Oncology (Williston Park). 2009; 23, 488–496, http://www.ncbi.nlm.nih.gov/pubmed/19544689.
- Lui P, Cashin R, Machado M, et al. Treatments for metastatic melanoma: Synthesis of evidence from randomized trials. Cancer Treat Rev. 2007; 33:665–680.
- Hill GJ 2nd, Krementz ET, Hill HZ. Dimethyl triazeno imidazole carboxamide and combination therapy for melanoma (IV). Late results after complete response to chemotherapy (Central Oncology Group protocols 7130, 7131, and 7131A). Cancer. 1984; 53:1299–1305.
- Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013; 369:122-133.
- Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010; 363:711-723 [Erratum: N Engl J Med. 2010; 363: 1290,].
- Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012; 366:2443-2454.
- Postow MA, Chesney J, Pavlick AC, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015; 372:2006-2017.
- Hodi FS, Chesney J, Pavlick AC, et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial. Lancet Oncol. 2016; 17:1558-1568.
- Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015; 373:23-34.
- Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017; 377, 1345–1356.
- Schadendorf D, Wolchok JD, Hodi FS, et al. Efficacy and Safety Outcomes in Patients with Advanced Melanoma who Discontinued Treatment with Nivolumab and Ipilimumab Because of Adverse Events: A Pooled Analysis of Randomized Phase II and III Trials. J Clin Oncol. 2017 Dec 1; 35(34): 3807–3814.
- Shoushtari AN, Friedman CF, Navid-Azarbaijani P, et al. Measuring Toxic Effects and Time to Treatment Failure for Nivolumab Plus Ipilimumab in Melanoma. JAMA Oncol. 2018;4(1):98–101. doi:10.1001/jamaoncol.2017.2391.

Limfomul nodal de zonă marginală – etiopatologie, diagnostic şi tratament
Lidia Felicia Mihai
Limfomul nodal de zonă marginală este un tip rar de limfom non-Hodgkin indolent. Acesta afectează în principal ganglionii limfatici, dar prezintă aspecte histologice similare cu limfomul splenic de zonă marginală sau cu limfomul marginal extranodal, de obicei fără a afecta alte structuri. Cu toate aceste...
Reguli pentru manipularea citostaticelor folosite în boala canceroasă
Alexandru Grigorescu
Manipularea citostaticelor utilizate în tratamentul cancerului incumbă cunoaşterea şi respectarea unor reguli stricte de transport, diluţie şi administrare. De asemenea, accidentele care pot apărea prin scurgeri ale soluţiilor de citostatice (contaminarea) trebuie prevenite, iar manevrele de decont...
Mezoteliom malign pleural la un pacient fără expunere la azbest
Samuel Bodoarcă, Diana Belciu (Bodoarcă), Diana Leonte, Irina Strâmbu
Mezoteliomul malign pleural reprezintă o formă agresivă de malignitate, de obicei legată de expunerea la azbest şi apărând la câteva decenii după expunere. Prezentăm cazul unui bărbat de 73 de ani, fără expunere aparentă...
Mezoteliom malign pleural la un pacient fără expunere la azbest
Samuel Bodoarcă, Diana Belciu (Bodoarcă), Diana Leonte, Irina Strâmbu
Mezoteliomul malign pleural reprezintă o formă agresivă de malignitate, de obicei legată de expunerea la azbest şi apărând la câteva decenii după expunere. Prezentăm cazul unui bărbat de 73 de ani, fără expunere aparentă...
Este urografia-CT cea mai bună metodă de evaluare a tumorilor renale asociate cu rinichiul în potcoavă?
Oana M. Rizea, Cristina Al. Nicolae, Ioana G. Lupescu
Obiectivul studiului nostru este de a discuta şi ilustra metodele imagistice utilizate pentru un diagnostic complet al leziunilor tumorale renale asociate celei mai frecvente anomalii de fuziune ren...