Etiopatogenia şi manifestările clinice ale limfoamelor asociate infecţiei cu HIV
Etiopathogeny and clinical characteristics of HIV-associated lymphomas
Abstract
Human immunodeficiency virus (HIV) infection causes dysregulation of cell immunity, which predisposes to the development of cancer, including lymphomas. The lifespan of people diagnosed with HIV has increased over the years and, as a result, malignancies have a larger contribution to morbidity and mortality in HIV-positive population. After the introduction of combination antiretroviral therapy (cART), it was observed that cancer is diagnosed in more than 40% of HIV-positive patients and almost 30% of HIV-related deaths are assigned to malignancy. Compared with general population, HIV-positive population has an increased risk to develop lymphomas. The improvement of survival in HIV-positive patients is the consequence of improved antiretroviral therapy, being more accessible and well tolerated, and the consequence of improved supportive strategies for these patients.Keywords
HIVlymphomacancerRezumat
Infecţia cu virusul imunodeficienţei umane (HIV) este asociată cu dereglări ale imunităţii celulare, care predispun la apariţia neoplaziilor, inclusiv a limfoamelor. Speranţa de viaţă a persoanelor diagnosticate cu HIV s-a îmbunătăţit de-a lungul anilor şi, ca urmare, neoplazia are o contribuţie crescută la morbiditatea şi mortalitatea populaţiei HIV-pozitive. După introducerea terapiei antiretrovirale combinate (cART), s-a observat că incidenţa cancerului este ridicată, mai mult de 40% dintre pacienţii cu HIV fiind diagnosticaţi cu cancer şi aproape 30% din decesele la pacienţii HIV-pozitivi sunt atribuite malignităţii. Faţă de populaţia generală, pacienţii cu HIV prezintă un risc crescut de a dezvolta limfoame. Ameliorarea supravieţuirii la pacienţii HIV-pozitivi este consecinţa îmbunătăţirii terapiei antiretrovirale, fiind mai accesibilă şi bine tolerată şi, de asemenea, este consecinţa unor strategii de suport îmbunătăţite pentru aceşti pacienţi.Cuvinte Cheie
HIVlimfomcancerIntroduction
Human immunodeficiency virus (HIV) infection causes dysregulation of cell immunity, which predisposes to the development of cancer, including lymphomas(1,2). The lifespan of people diagnosed with HIV has increased over the years and, as a result, malignancies have a larger contribution to morbidity and mortality in HIV-positive population. After the implementation of combination antiretroviral therapy (cART), it was observed that cancer is diagnosed in more than 40% of HIV-positive patients and almost 30% of HIV-related deaths are assigned to malignancy(3). In HIV-positive population, the presence of Kaposi sarcoma, advanced cervical cancer and of certain types of lymphomas, such as systemic high-grade B-cell non-Hodgkin lymphoma or primary central nervous system (CNS) lymphoma, is considered pathognomonic for acquired immunodeficiency syndrome (AIDS). Other types of lymphomas, such as Hodgkin lymphoma or follicular lymphoma, are not considered AIDS-defining. The clinical presentation of lymphomas in HIV-positive population is different from lymphomas in HIV-negative patients(4,5).
Epidemiology
Compared with the general population, HIV-positive population has an increased risk to develop lymphomas. For example, a meta-analysis that evaluated over 400,000 patients from 7 cancer registries demonstrated an increased risk from 23 to 350 fold of lymphoma development in HIV-positive patients compared to the general population(6). Also, a study of 47,000 HIV-positive patients receiving antiretroviral therapy reported that 10% of deaths were related to cancer and that non-Hodgkin lymphoma (NHL) was the most common cause of death among these patients(7).
Another population-based study that included 448,258 HIV-positive patients for a period of 16 years, from 1996 to 2012, conducted in the United States, showed an increased risk of NHL, with a standardized incidence ratio of 11.15 compared with the general population(8).
The incidence of Hodgkin lymphoma, comparing with non-Hodgkin lymphoma, was unchanged regardless ART use(9).
HIV-related lymphomas are more common in males than in females, independent of cART use(10,11).
After the implementation of cART, the risk of NHL development decreased at first and remained stable over time, the decline being attributed to the improvements in CD4 counts(12,13). The increased proportion of HIV-positive patients who received cART was also associated with changes in the clinical features of HIV-related NHL.
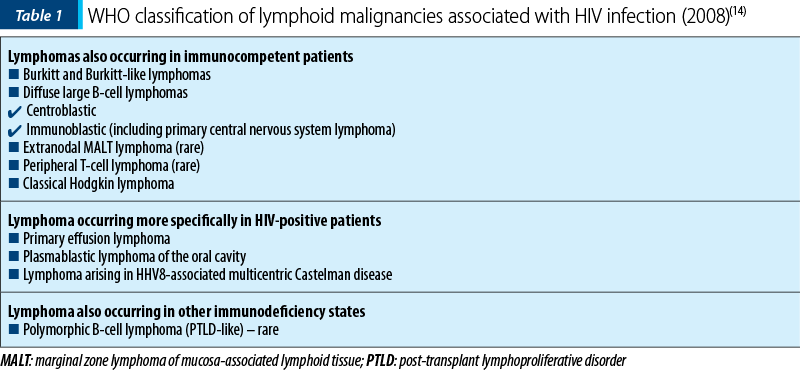
Specific HIV-related NHL, based on location, can be classified into three main categories: systemic NHL, primary central nervous system lymphoma, and primary effusion lymphoma.
Systemic NHL can be further divided into common subtypes described in the World Health Organization (WHO) classification system.
The most common systemic NHL subtypes observed in HIV-positive patients are diffuse large B-cell lymphoma, accounting for 70%, followed by Burkitt lymphoma (20%), indolent B cell lymphoma (10%), plasmablastic lymphoma (approximately 5%), and T-cell lymphoma (3%). Primary CNS lymphoma accounts for 15% of all cases, while primary effusion lymphoma is present in less than 1% of cases(15-17).
Hodgkin lymphoma (HL) is the most common non-AIDS-defining malignancy. The incidence of HL is 15 to 30 times higher than in the general population(12). The characteristics of HL in HIV-positive population include unfavorable histology and mixed cellularity, accounting for 60% of cases in two studies(18,19). The majority of patients with HIV-related HL are Epstein-Barr virus (EBV) positive. Another characteristic is that HL tends to develop early in the history of HIV infection. The relationship between HL and CD4 cell count is not really established, some studies indicating that severe immunosuppression is associated with HL, and others not finding any correlation between CD4 cell count and HL(20,21). The impact of cART on the incidence of HL is also unclear: some studies suggest that the incidence has increased in the cART era(22), and others did not observe a significant change(21,23). Some authors state that the risk of HL may be increased especially in the first months after the initiation of cART(24,25).
Pathogenesis
HIV infection. There is no evidence that HIV infection itself can determine cell transformation, since HIV does not infect directly the lymphoma cells, having mainly an indirect role by immunosuppression, and this is supported by the inverse association between CD4+ cell count and NHL onset(26). It is also observed that the risk of lymphoma remains high even after the widespread use of cART, concluding that the relationship between the immunological state and lymphoma development is much more complex(27,28).
Only recently a possible direct effect of HIV through secreted or transmitted viral proteins has been described: Tat protein of HIV may lead to dysregulation of the protein products of RBL2 (pRb2/p130) and may also increase the angiogenic activities of bFGF and VEGF(29). Also, specific variants of HIV p17 have been found to be associated with the development of lymphoma(30).
The specific role of oncogenic viruses – such as Epstein-Barr virus (EBV) and human herpesvirus-8 (HHV-8) – in HIV-related lymphomas pathogenesis is well known, and most lymphomas are associated with these virus infections. Also, the incidence of EBV-associated lymphomas, like Burkitt lymphoma or Hodgkin lymhoma, is still high even after the beginning of ART. The incidence of HHV8-associated primary effusion lymphoma and multicenter Castleman disease remains unchanged by the use of cART(31). It is also known that chronic inflammation could contribute to the development of any cancer, and even in the presence of a long period of viral suppression, inflammatory biomarkers remain at high levels in HIV-positive patients(28,32).
Regarding hepatitis B and C, it is well known the role in the development of NHL in the general population due to B-cell proliferation and to chronic immune activation. In HIV-positive patients ART-treated, the association of hepatitis B or C virus infection and the risk of NHL was observed in a large European study, with a hazard ratio of 1.7(33).
Gene deregulation. Increased expression of BCL-6 is present in more than 70% of HIV-associated lymphomas and in 20% of HIV-associated diffuse large B-cell lymphoma (DLBCL)(34). In DLBCL, a study of patients with and without HIV demonstrated that BCL-6 expression is increased in HIV-positive versus HIV-negative patients (45%, respectively 10%)(35). HIV-associated lymphomas with BCL6 activation and without any other genetic lesions appear to have a better prognosis compared with those BCL-6 negative(36).
MYC translocations are present in 20% of HIV-associated DLBCL and are less common in DLBCL in general population.
Clinical characteristics
Diffuse large B-cell lymphoma is the most frequent HIV-associated lymphoma. It often presents in advanced stages and with B symptoms, and extralymphatic involvement is often present, especially in patients with severe immunosuppression. The prognosis, determined by the International Prognostic Index (IPI), is influenced by multiple factors related to patient, lymphoma and HIV infection. Low CD4 counts have been associated with poor survival in multiple studies, while others have not found an association(37,38). To evaluate the prognosis of HIV-associated lymphoma, an AIDS-related lymphoma IPI has been recently developed, that employs the Age Adjusted-IPI, and an HIV severity score that includes CD4 count, viral load and prior history of AIDS(39).
Burkitt lymphoma (BL) is the second most common type of HIV-associated lymphoma. It usually appears in HIV patients with preserved CD4 count. Extranodal involvement is common, and the incidence of CNS involvement is present in up to 28% of cases. Typically, patients present with poor performance status and high levels of lactate dehydrogenase(28,40). Even after the introduction of cART, the prognosis and survival of BL patients remained poor(41).
Plasmablastic lymphoma (PBL) was first described in the 90s as a rare subtype of DLBCL, with plasmacytoid features, affecting primarily mucosal sites and being common in HIV-positive patients. It is characterized by loss of mature B-cell markers, including CD20, and with an elevated proliferation index, being associated in almost all cases with EBV infection. Up to 50% of the cases present c-MYC translocation, associated with poorer prognostic(42).
Primary effusion lymphoma (PEL) is a rare B-cell lymphoma characterized by effusions that can affect any serosa, pleura, pericardium and peritoneum. Also, a rare solid extracavitary variant has been described. Severe immunosuppression with low CD4+ cell counts is common. The characteristics of PEL are the presence of lymphocyte activation markers, CD30 and CD38, and the absence of normal B-cell markers, CD19 and CD20. HHV8 infection is present in almost all cases, and other HHV8-related malignancies, like Kaposi syndrome or multicentric Castleman disease (MCD), may precede or be present in the same time with PEL(43,44).
Primary central nervous system lymphoma (PCNSL) is a subtype of DLBCL with a post-germinal center phenotype. EBV is almost always present in lymphoma cells and cerebrospinal fluid, compared with HIV-negative population in which is almost always negative(45,46). The clinical findings and standard radiological investigations are not sufficient for a positive diagnosis and it is usually mandatory to have a brain biopsy, but the combination of radiological findings and detectable EBV in cerebrospinal fluid in a severe immunocompromised HIV-positive patient may be sufficient for diagnosis, but only in selected cases(28).
Hodgkin lymphoma in HIV patients is usually associated with unfavorable characteristics like advanced stage and extranodal and bone marrow involvement. It is associated with EBV infection in 80-100% of cases. The mixed cellularity is the most common HL subtype. The incidence of HL in HIV-positive patients remained stable or has even increased after the introduction of cART(12). Low CD4 count is cosidered an independent adverse prognostic factor(28,47).
Multicentric Castleman disease is a very aggressive B-cell lymphoproliferative disorder and has an increased incidence in HIV-positive patients(48). It can have various clinical features, affecting lymph nodes, with spleen enlargements, and is associated with B symptoms. Hemophagocytic syndrome is a complication that can appear in the clinical course of the disease. Almost all MCD cases in HIV-positive patients are associated with HHV-8 infection(49).
Conclusions
The improvement of survival in HIV-positive patients is the consequence of improved antiretroviral therapy, being more accessible and well tolerated, and to improved supportive strategies for these patients. Also, the introduction of antiretroviral therapy is associated with a decrease in incidence of toxicities related to therapy of HIV-associated lymphomas. The treatment of patients with HIV-related lymphomas should be the same as in non-HIV lymphoma patients, and clinical trials that included HIV-positive patients with lymphoma showed that responses are identical in both populations, with the observation that a special attention should be granted to cART interaction with chemotherapeutic agents, to potential cumulative toxicities, and to risk for other infections in HIV-positive patients. n
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Conant MA. Management of human immunodeficiency virus-associated malignancies. Recent Results Cancer Res. 1995; 139:423.
-
Akanmu AS. AIDS-associated malignancies. Afr J Med Med Sci. 2006; 35 Suppl:57.
-
Gérard L, Galicier L, Boulanger E, et al. Improved survival in HIV-related Hodgkin’s lymphoma since the introduction of highly active antiretroviral therapy. AIDS. 2003; 17:81.
-
Burgi A, Brodine S, Wegner S, et al. Incidence and risk factors for the occurrence of non-AIDS-defining cancers among human immunodeficiency virus-infected individuals. Cancer. 2005; 104:1505.
-
Shiels MS, Pfeiffer RM, Hall HI, et al. Proportions of Kaposi sarcoma, selected non-Hodgkin lymphomas, and cervical cancer in the United States occurring in persons with AIDS, 1980-2007. JAMA. 2011; 305:1450.
-
Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet. 2007; 370:59.
-
Engels EA, Yanik EL, Wheeler W, et al. Cancer-Attributable Mortality Among People With Treated Human Immunodeficiency Virus Infection in North America. Clin Infect Dis. 2017; 65:636.
-
Hernández-Ramírez RU, Shiels MS, Dubrow R, Engels EA. Cancer risk in HIV-infected people in the USA from 1996 to 2012: a population-based, registry-linkage study. Lancet HIV. 2017; 4:e495.
-
Hleyhel M, Hleyhel M, Bouvier AM, et al. Risk of non-AIDS-defining cancers among HIV-1-infected individuals in France between 1997 and 2009: results from a French cohort. AIDS. 2014; 28:2109.
-
Yanik EL, Achenbach CJ, Gopal S, et al. Changes in Clinical Context for Kaposi’s Sarcoma and Non-Hodgkin Lymphoma Among People With HIV Infection in the United States. J Clin Oncol. 2016; 34:3276.
-
Bower M, Fisher M, Hill T, et al. CD4 counts and the risk of systemic non-Hodgkin’s lymphoma in individuals with HIV in the UK. Haematologica. 2009; 94:875.
-
Silverberg MJ, Lau B, Achenbach CJ, et al. Cumulative Incidence of Cancer among Persons with HIV in North America: A Cohort Study. Ann Intern Med. 2015; 163:507.
-
Biggar RJ, Chaturvedi AK, Goedert JJ, et al. AIDS-related cancer and severity of immunosuppression in persons with AIDS. J Natl Cancer Inst. 2007; 99:962.
-
Raphael M, Said J, Borish B, Ceserman E, Harris NL. Lymphomas associated with HIV infection. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: IARC Press; 2008.
-
Mantina H, Wiggill TM, Carmona S, et al. Characterization of lymphomas in a high prevalence HIV setting. J Acquir Immune Defic Syndr. 2010; 53:656.
-
Guech-Ongey M, Simard EP, Anderson WF, et al. AIDS-related Burkitt lymphoma in the United States: what do age and CD4 lymphocyte patterns tell us about etiology and/or biology? Blood. 2010; 116:5600.
-
Coté TR, Biggar RJ, Rosenberg PS, et al. Non-Hodgkin’s lymphoma among people with AIDS: incidence, presentation and public health burden. AIDS/Cancer Study Group. Int J Cancer. 1997; 73:645.
-
Hentrich M, Berger M, Wyen C, et al. Stage-adapted treatment of HIV-associated Hodgkin lymphoma: results of a prospective multicenter study. J Clin Oncol. 2012; 30:4117.
-
Deeken JF, Tjen-A-Looi A, Rudek MA, et al. The rising challenge of non-AIDS-defining cancers in HIV-infected patients. Clin Infect Dis. 2012; 55:1228.
-
Clifford GM, Rickenbach M, Lise M, et al. Hodgkin lymphoma in the Swiss HIV Cohort Study. Blood. 2009; 113:5737.
-
Frisch M, Biggar RJ, Engels EA, et al. Association of cancer with AIDS-related immunosuppression in adults. JAMA. 2001; 285:1736
-
Powles T, Robinson D, Stebbing J, et al. Highly active antiretroviral therapy and the incidence of non-AIDS-defining cancers in people with HIV infection. J Clin Oncol. 2009; 27:884.
-
Seaberg EC, Wiley D, Martínez-Maza O, et al. Cancer incidence in the multicenter AIDS Cohort Study before and during the HAART era: 1984 to 2007. Cancer. 2010; 116:5507.
-
Lanoy E, Rosenberg PS, Fily F, et al. HIV-associated Hodgkin lymphoma during the first months on combination antiretroviral therapy. Blood. 2011; 118:44.
-
Gotti D, Danesi M, Calabresi A, et al. Clinical characteristics, incidence, and risk factors of HIV-related Hodgkin lymphoma in the era of combination antiretroviral therapy. AIDS Patient Care STDS. 2013; 27:259.
-
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Biological agents. Volume 100B. A Review of human carcinogenesis. IARC Monogr Eval Carcinog Risks Hum. 2012; 100(pt B):1–441.
-
Biggar RJ, Chaturvedi AK, Goedert JJ, Engels EA. AIDS-related cancer and severity of immunosuppression in persons with AIDS. J Natl Cancer Inst. 2007; 99:962–972.
-
Re A, Cattaneo C, Rossi G. HIV and Lymphoma: from Epidemiology to Clinical Management. Mediterr J Hematol Infect Dis. 2019; 11(1):e2019004.
-
De Falco G, Bellan C, Lazzi S, et al. Interaction between HIV-1 Tat and pRb2/p130: a possible mechanism in the pathogenesis of AIDS-related neoplasms. Oncogene. 2003; 22:6214.
-
Dolcetti R, Giagulli C, He W, Selleri M, Caccuri F, Eyzaguirre LM, Mazzuca P, Corbellini S, Campilongo F, Marsico S, Giombini E, Muraro E, Rozera G, De Paoli P, Carbone A, Capobianchi MR, Ippolito G, Fiorentini S, Blattner WA, Lu W, Gallo RC, Caruso A. Role of HV-1 matrix protein p17 variants in lymphoma pathogenesis. Proc Natl Acad Sci USA. 2015; 112:14331–14336.
-
Parka LS, Hernandez-Ramirez RU, Silverberg MJ, Crothers KA, Dubrow R. Prevalence of non-HIV cancer risk factors in persons living with HIV/AIDS. AIDS. 2016; 30:273–291.
-
Hunt PW. HIV and inflammation: mechanisms and consequences. Curr HIV/AIDS Rep. 2012; 9:139–147.
-
Wang Q, De Luca A, Smith C, et al. Chronic Hepatitis B and C Virus Infection and Risk for Non-Hodgkin Lymphoma in HIV-Infected Patients: A Cohort Study. Ann Intern Med. 2017; 166:9.
-
Gaidano G, Capello D, Carbone A. The molecular basis of acquired immunodeficiency syndrome-related lymphomagenesis. Semin Oncol. 2000; 27:431.
-
Chao C, Silverberg MJ, Xu L, et al. A comparative study of molecular characteristics of diffuse large B-cell lymphoma from patients with and without human immunodeficiency virus infection. Clin Cancer Res. 2015; 21:1429.
-
Hoffmann C, Tiemann M, Schrader C, et al. AIDS-related B-cell lymphoma (ARL): correlation of prognosis with differentiation profiles assessed by immunophenotyping. Blood. 2005; 106:1762.
-
Rossi G, Donisi A, Casari S, Re A, Cadeo G, Carosi G. The International Prognostic Index can be used as a guide to treatment decisions regarding patients with human immunodeficiency virus-related systemic non-Hodgkin lymphoma. Cancer. 1999; 86:2391–7.
-
Lim ST, Karim R, Tulpule A, Nathwani BN, Levine AM. Prognostic factors in HIV-related duffuse large B-cell lymphoma: before versus after highly active antiretroviral therapy. J Clin Oncol. 2005; 23:8477–82.
-
Barta SK, Xue X, Wang D, Lee JY, Kaplan LD, Ribera JM, Oriol A, Spina M, Tirelli U, Boue F, Wilson WH, Wyen C, Dunleavy K, Noy A, Sparano JA. A new prognostic score for AIDS-related lymphomas in the rituximab-era. Haematologica. 2014; 99:1731–37.
-
Spina M, Tirelli U, Zagonel V, Gloghini A, Volpe R, Babare R, Abbruzzese L, Talamini R, Vaccher E, Carbone A. Burkitt’s lymphoma in adults with and without human immunodeficiency virus infection: a single-institution clinicopathologic study of 75 patients. Cancer. 1998; 82:766–74.
-
Lim ST, Karim R, Nathwani BN, Tulpule A, Espina B, Levine AM. AIDS-related Burkitt’s lymphoma versus diffuse large-cell lymphoma in the pre-highly active antiretroviral therapy (HAART) and HAART eras: significant differences in survival with standard chemotherapy. J Clin Oncol. 2005; 23:4430–8.
-
Delecluse HJ, Anagnostopoulos I, Dallenbach F, Hummel M, Marafioti T, Schneider U, Huhn D, Schmidt-Westhausen A, Reichart PA, Gross U, Stein H. Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood. 1997; 89:1413–20.
-
Nador RG, Cesarman E, Chadburn A, Dawson DB, Ansari MQ, Sald J, Knowles DM. Primary effusion lymphoma: a distinct clinicopathologic entity associated with the Kaposi’s sarcoma-associated herpes virus. Blood. 1996; 88:645–56.
-
Chen YB, Rahemtullah A, Hochberg E. Primary effusion lymphoma. Oncologist. 2007; 12:569–76. doi: 10.1634/theoncologist.12-5-569.
-
Skiest DJ, Crosby C. Survival is prolonged by highly active antiretroviral therapy in AIDS patients with primary central nervous system lymphoma. AIDS. 2003; 17:1787–93.
-
Remick SC, Diamond C, Migliozzi JA, Solis O, Wagner H, Jr, Haase RF, Ruckdeschel JC. Primary central nervous system lymphoma in patients with and without the acquired immune deficiency syndrome: a retrospective analysis and review of the literature. Medicine (Baltimore). 1990; 69:345–60.
-
Castillo JJ, Bower M, Brühlmann J, Novak U, Furrer H, Tanaka PY, Besson C, Montoto S, Cwynarski K, Abramson JS, Dalia S, Bibas M, Connors JM, Furman M, Nguyen ML, Cooley TP, Beltran BE, Collins JA, Vose JM, Xicoy B, Ribera JM HIV-Associated Hodgkin Lymphoma in the cART Era Study Group. Prognostic factors for advanced-stage human immunodeficiency virus-associated classical Hodgkin lymphoma treated with doxorubicin, bleomycin, vinblastine, and dacarbazine plus combined antiretroviral therapy: a multi-institutional retrospective study. Cancer. 2015; 121:423–31.
-
Fajgenbaum DC, Ruth JR, Kelleher D, Rubenstein AH. The collaborative network approach: a new framework to accelerate Castleman’s disease and other rare disease research. Lancet Haematol. 2016; 3:150–2.
-
Oksenhendler E, Boutboul D, Fajgenbaum D, Mirouse A, Fieschi C, Malphettes M, Vercellino L, Meignin V, Gérard L, Galicier L. The full spectrum of Castleman disease: 273 patients studied over 20 years. Br J Haematol. 2018; 180:206–16.

Predispoziţia la transformare din sindrom mielodisplazic în leucemie acută – prezentare de caz
Iuliana-Maria Nicorescu, Minodora Onisâi, Mihaela Găman, Iuliana Iordan, Lidia Felicia Mihai, Andreea Crăciunescu, Mihai Ciochinaru, Ana Maria Vlădăreanu
Sindroamele mielodisplazice (SMD) sunt un grup de boli clonale ale celulei stem hematopoietice, caracterizate de mielodisplazie şi...
Managementul tratamentului şi urmărirea pacienţilor cu melanom malign în perioada pandemiei de COVID-19
Daniela Zob, Cornelia Niţipir, Laura Mazilu, Gabriela Niculai, Alina Moldovan, Lidia Kajanto, Andra-Iulia Suceveanu, Radu Florin, Silviu VOINEA, Viorel Savin, Amalia Constantinescu, Alexandru Grigorescu, Raluca Ioana Mihăilă, Dana Lucia Stănculeanu
Melanomul este o problemă de sănătate publică, prin incidenţa sa în creştere şi prin vârsta mică la diagnostic. Există trei sub...
Managementul tratamentului şi urmărirea pacienţilor cu cancer de sân în perioada pandemiei de COVID-19
Daniela Zob, Dana Lucia Stănculeanu, Mădălina Drăgănescu, Laura Mazilu, Cornelia Niţipir, Amalia Constantinescu, Gabriela Niculai, Adelina Silvana Gheorghe, Andreea-Daniela Gheorghe, Alexandru BLIDARU
Cancerul mamar ocupă locul întâi în privinţa tipurilor de neoplazie întâlnite la sexul feminin la nivel global, fiind a doua cau...
Predispoziţia la transformare din sindrom mielodisplazic în leucemie acută – prezentare de caz
Iuliana-Maria Nicorescu, Minodora Onisâi, Mihaela Găman, Iuliana Iordan, Lidia Felicia Mihai, Andreea Crăciunescu, Mihai Ciochinaru, Ana Maria Vlădăreanu
Sindroamele mielodisplazice (SMD) sunt un grup de boli clonale ale celulei stem hematopoietice, caracterizate de mielodisplazie şi...
Managementul tratamentului şi urmărirea pacienţilor cu cancer de sân în perioada pandemiei de COVID-19
Daniela Zob, Dana Lucia Stănculeanu, Mădălina Drăgănescu, Laura Mazilu, Cornelia Niţipir, Amalia Constantinescu, Gabriela Niculai, Adelina Silvana Gheorghe, Andreea-Daniela Gheorghe, Alexandru BLIDARU
Cancerul mamar ocupă locul întâi în privinţa tipurilor de neoplazie întâlnite la sexul feminin la nivel global, fiind a doua cau...