Importanţa cunoştinţelor şi a comportamentului pacienţilor după diagnosticarea cancerului de sân
The significance of patient’s knowledge and behavior after breast cancer diagnosis
Abstract
Breast cancer is the most frequent neoplasia in females, accounting for approximately 26% of all newly diagnosed neoplasia, and the second cause of death after lung cancer. Every year, over 8,900 new cases of breast cancer are diagnosed in Romania, of which 1,800 are in advanced stages of the disease. In our country, compared to other European countries, breast cancer is diagnosed in stages III-IV (58.4% of patients), while in other countries, new cases of cancer are detected in the early stages of the disease. It is well known that unknowledgement of the illness, ignorance and non-attendance in a timely manner in a specialized service determine an increase in advanced stages, implicitly in mortality. This objective study, based on specialized questionnaires, attempts to define the necessary interventions to promote breast cancer awareness, increase risk-related knowledge and promote screening. It is also intended to encourage proactive behavior, as the family doctor becomes involved in the identification, awareness and monitoring the cancer disease. We would like to highlight the need for the implementation of specialized information programs for the population, mentioning the importance of implementing a national sceening program.Keywords
knowledgeawarenessbreast cancerdisease screeningRezumat
Cancerul mamar este neoplazia cu frecvenţa cea mai mare la sexul feminin, reprezentând aproximativ 26% din toate cancerele diagnosticate anual, fiind a doua cauză de deces după cancerul pulmonar la femei. În fiecare an, în România sunt diagnosticate peste 8.900 de cazuri noi de cancer mamar, dintre care 1.800 sunt în stadii avansate ale bolii. În România, comparativ cu alte state europene, depistarea cancerului mamar se face în stadiile III-IV (58,4% dintre paciente), în timp ce în alte ţări depistarea cazurilor noi de cancer se face în stadiile incipiente ale bolii. Este bine cunoscut faptul că nerecunoaşterea bolii, ignoranţa şi neprezentarea în timp util într-un serviciu specializat determină o creştere a stadiilor avansate, implicit a mortalităţii. Prin acest studiu obiectiv, bazat pe chestionare specializate, se încearcă definirea intervenţiilor necesare pentru a promova conştientizarea cancerului mamar, creşterea cunoştinţelor legate de factorii de risc şi promovarea screeningului. Se urmăreşte şi încurajarea comportamentului proactiv, pe măsură ce se implică şi medicul de familie în procesul de identificare, conştientizare şi monitorizare a bolii neoplazice mamare. Dorim să subliniem necesitatea implementării unor programe informative populaţionale, specializate, menţionând şi importanţa implementării unui program naţional de screening.Cuvinte Cheie
cunoaştereconştientizareneoplasm mamarscreeningul boliiPreamble
Breast cancer is the neoplasia with the highest frequency in women, representing approximately 26% of all annually diagnosed cancers, being the second death cause after lung cancer in women(1). Although the prognosis of primary breast cancer has improved significantly over the last 20 years, a large number of patients will present illness evolution and most of them will die due to this cancer, both in developed countries, as well as in developing countries, such as Romania. On a global scale, millions of cases of breast cancer receive early diagnosis, but nonetheless the mortality rate following this diagnosis of mammary neoplasm is worrying – about 14%.
Although it is known that breast cancer is an invasive and aggressive malady, it was found that its occurrence reduced in older women, but increased in women with ages ranging between 40 and 50 years old. The early detection by self-examination, together with genetic, social and economic factors, and the accessibility of a prompt treatment play an important role in the decrease of mortality and morbidity. It is well known that not recognizing the illness, ignoring it, or failing to receive special care in due time determine an increase of late stage cancers, and implicitly of mortality(2).
Romania, together with Greece and Slovakia are the only countries in the European Union without a national breast cancer screening program, given that in our country the mortality rate due to breast cancer is 25% higher than in the European Union. Each year, in Romania there are diagnosed more than 8,900 new cases of breast cancer, of which 1,800 are in the late stages of the illness. In Romania, as compared to other European countries, the discovery of breast cancer occurs in stages III-IV (58.4% of the patients), while in other countries the new cases of breast cancer are discovered in the incipient stages of the disease.
For this reason, over the last few years, numerous studies have been dedicated to understanding this illness at the molecular level, to identify new biomarkers which are important in different stages of the onset and progress of the tumor, but also in the metastasis process. The causes of breast cancer are not yet fully known. Epidemiologic studies regarding the etiology of breast cancer classify the etiological factors in two categories: exogenous and endogenous. Of the exogenous factors, we would like to mention: diet, alcohol, medical procedures, ultraviolet radiations, sexual and reproductive behavior. The category of endogenous factors include: patient’s age, family history, breast density, menarche, number of pregnancies, hormonal substitution therapy.
In the developed countries, the deployment of screening programs leads to the early detection of breast cancer, which determines the decrease of mortality by making choices from a large variety of therapeutic options.
In our country, attempts of raising awareness through media concerning the mammary neoplasm, using flyers and advertising spots, had no major impact within the population. In our country, there is still an opportunistic screening while taking into account the essential elements of a screening program. What we want and wish is an effective screening program.
This paper tries to highlight the level of knowledge regarding mammary neoplasm within women, regardless of the patients’ origin, intellect, age or occupation. Also, we want to emphasize the need of implementing specialized, information programs and, last but not least, the importance of implementing a national screening program.
Materials and method
1. Aim of the research
The research was initiated on a lot of patients diagnosed with breast cancer, admitted in the Third Surgery Departament of the “Prof. Dr. Alexandru Trestioreanu” Institute of Oncology, Bucharest. We started from the assumption that the study will be expanded if the results prove to be significant, considering that such investigations had not been realized in our institute before.
2. Research instruments
The instrument used to gather data was the questionnaire (according to Annex 1).
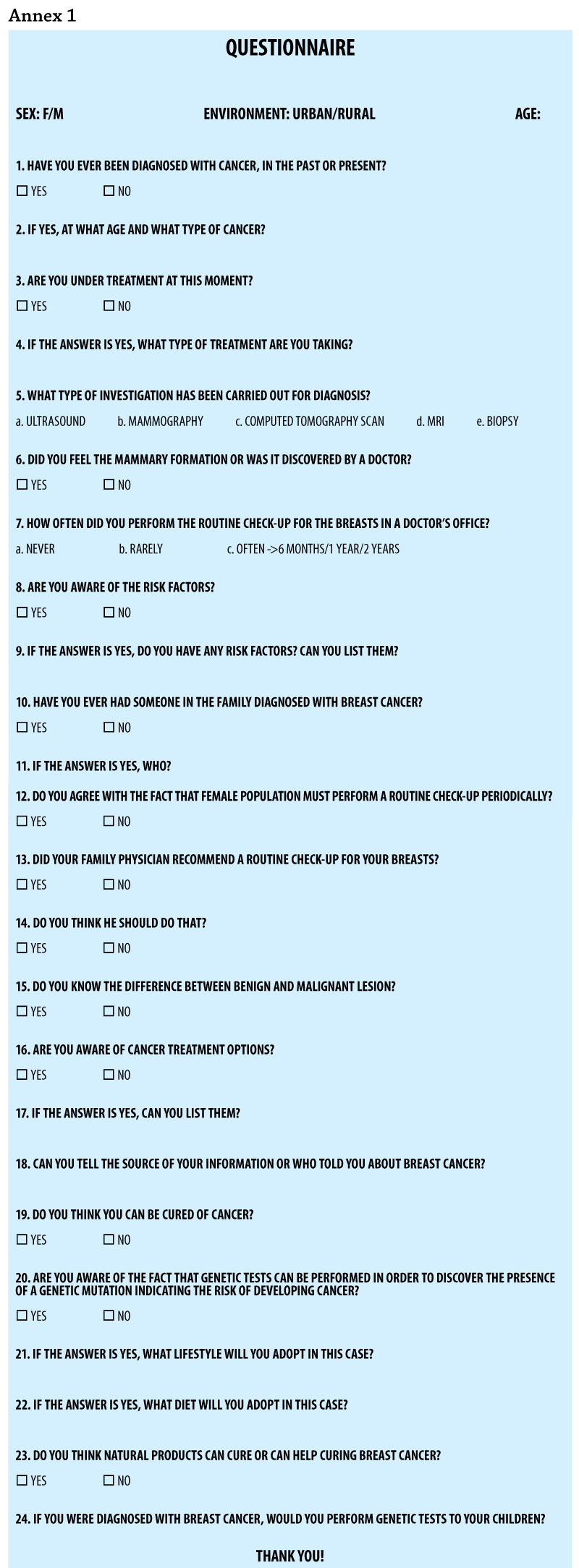
Starting from the hypothesis above, a type of questionnaire was drafted and distributed to a group of 100 test subjects in order to be filled in. Twenty-four questions were asked, choosing carefully the specialized language, the type and order.
3. Grouping
The size of the group was set to 100 patients admitted in the Third Surgery Departament of the “Prof. Dr. Alexandru Trestioreanu” Institute of Oncology, Bucharest. We think that the number of enrolled patients is enough for this type of study and that the selected subjects were representative for obtaining the necessary information.
4. Gathering data
The questionnaires were distributed in the department, accompanied by an annex in which we explained the significance of this study, at the same time bringing insurance that the confidentiality of the supplied data shall be fully observed. The answer rate was 100%, which proves the significance given by the subjects to the approached issues and which led to obtaining enough information to finalize the study.
Results
Regarding the 100 patients included in the study, there is a heterogeneous distribution per age group and origin. In Figure 1 it is shown the distribution per age groups as follows: 30-40 years – 12 patients (12%); 41-50 years – 20 patients (20%); 51-60 years – 24 patients (24%); 61-70 years – 32 patients (32%), and over 70 years – 12 patients (12%).

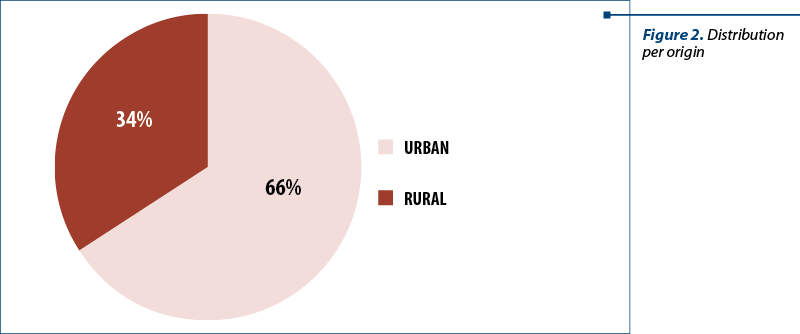
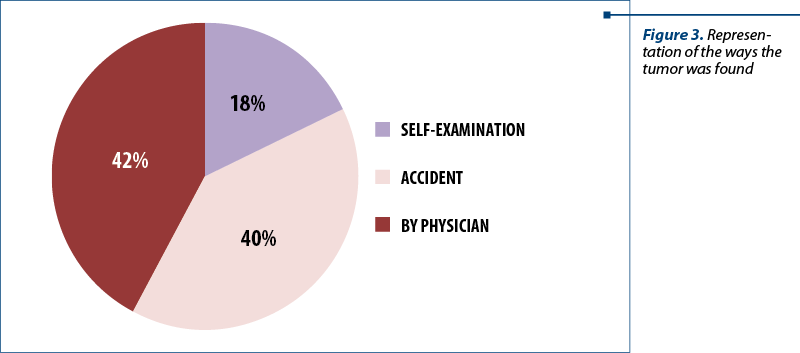
Regarding the average origin distribution, 34% of the patients (34) were from rural areas, and 66% from urban areas (66 patients) – Figure 2. When asked how they found the lesion (Figure 3), 42 patients (42%) claimed the lesion was found following specialty medical consultation, 40 patients found it accidently, and 18 patients (18%) found it by periodic self-examination of the breast.
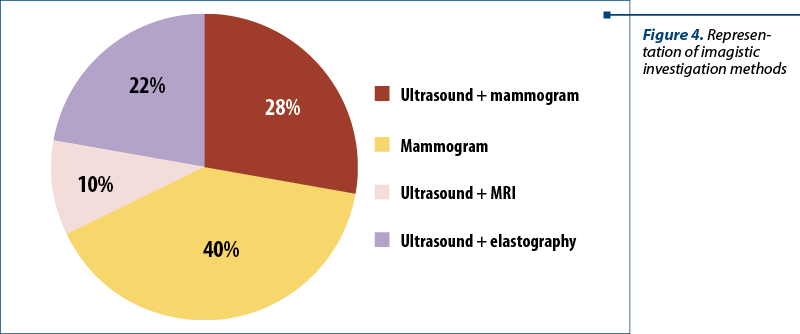
Following the question about the way the tumor was discovered, there was the question regarding the confirmation of the tumor formation existence and the orientation towards a preliminary diagnosis, so in Figure 4 there are represented the imagistic diagnosis methods.
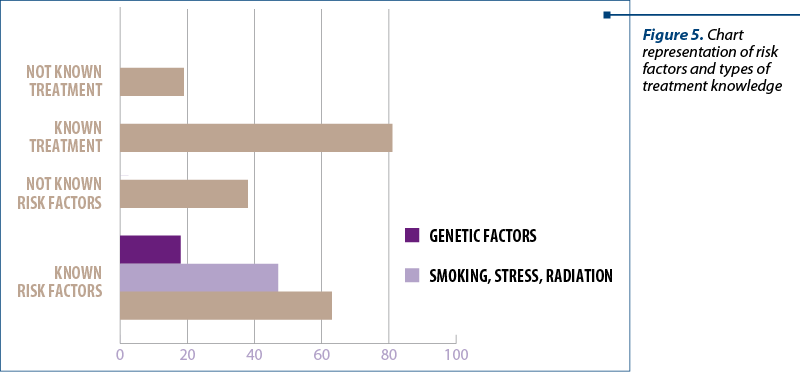
After the detection of the mammary nodule formation, the patients were asked if they knew the risk factors for the occurrence of mammary neoplasm and the types of treatment approached. The patients gave the following answers: 32 patients knew the risk factors, of which 24 knew the usual risk factors for all neoplasia, and only 8 knew the existence of hereditary factors; 18 patients could not name any risk factors. Of the total of 100 patients, 8 patients could not state the type of treatment approached (Figure 5).
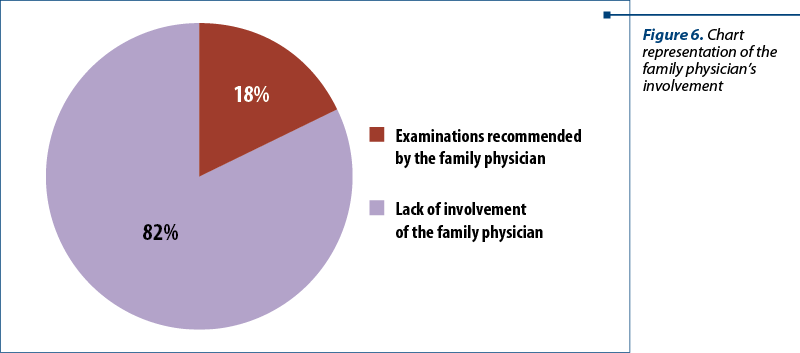
The interest of family physicians in the prevention and early detection of breast cancer is deficient, claimed 82% of the patients (Figure 6).
As the support of decision-making factor is absolutely necessary in the deployment process of innovative procedures and methods in the activity of any entity, the research shows mainly the patients’ opinion regarding the need for involvement by the family physician. This is an essential part of the primary assistance in order to advise and guide the patient towards secondary assistance care – specialized medical care. Secondary care has an essential role in the early detection of malignant lesions, coordination of specialized treatment according to staging, and patient guidance for psychological and nutritional support.
Ninety-six percent of the patients claimed that the family physician plays an important role by performing periodic check-ups and guiding the patients to perform specialty imagistic examinations according to medical protocols.
When asked about the information source on the identified neoplasm, 50 patients claimed that the source was the internet, 16 patients found out from acquaintances, and 34 patients from specialty medical professionals (Figure 7).

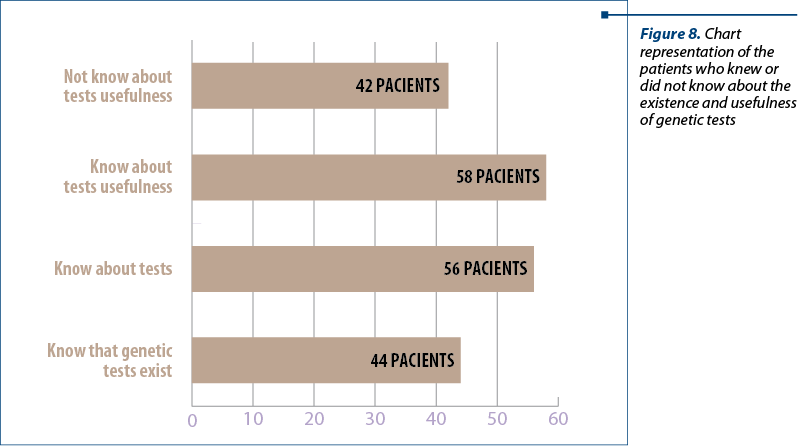
When asked about the existence of genetic tests and their usefulness in treatment personalization, in the follow-up, as well as the involvement of family risks, 44 patients admitted knowing about the existence of the tests and 58 knew about their usefulness (Figure 8).
The alimentation of the patients is different: 58 patients preferred the protein diet, 22 patients preferred the Mediterranean diet, and 20 patients only ate vegan food. When asked about adopting new eating habits after receiving the breast cancer diagnosis, 68 patients took on the vegan diet, 18 patients maintained their protein diet, and 14 patients adopted the Mediterranean one.
Discussion
As the occurrence of breast cancer is increasing worldwide, the understanding of knowledge, attitude and behavior of women involved in breast cancer screening is essential. Screening is the first step towards early finding of cancer. Developed countries have been proving this for decades by deploying specialized programs and by the existence and intensification of information campaigns regarding this pathology(3,4).
In our country, it was attempted the organization of sensitization sessions and campaigns in order to inform women about breast cancer, but these were insufficient. Despite that, no studies were performed in order to examine the knowledge, attitude and post-campaign practices in the afferent target group.
Our study – still in the early stages and just initiated in the Third Surgery Department – tries to show some useful aspects: the understanding, knowledge, clinical symptoms identification for this illness, and the need to visit the physicians’ offices without fear.
By this objective study, based on specialized questionnaires, it is attempted the definition of interventions necessary to promote the awareness on mammary neoplasm, increase knowledge on the risk factors and promote screening, but at the same time, it is intended to encourage the proactive behavior of the family doctor which must become involved in the identification, awareness, and monitoring of the neoplastic breast disease.
Knowing about breast cancer, the regular screening with mammography investigations, and self-examination of the breast are expected to be associated with the previous decision to seek for medical care. Solid, specialized knowledge will also be associated with more involvement in the treatment process and with the achievement of better results(5). The patients of this study have reported limited knowledge regarding breast cancer; they were not associated with the stage upon diagnosis or in the treatment decision, thus being unable to have an active role in the matter.
The results obtained through specialty studies indicated an increase in knowledge regarding breast cancer in women who used the internet, as opposed to those who talked about it with adequate, advised medical staff(6). This also resulted from our study.
According to the results obtained in our research, the contribution of the physician in the improvement of knowledge wasn’t highly significant, as expected, thus being suggested that his role needs to be more important in the medical education, for the patient to absorb the information.
The diagnosis and treatment of mammary neoplasm affect the lifestyle and dietary behavior of patients due to states of confusion, desperation and depression. Many patients become easy targets for the “pseudo-oncologic” industry by replacing or improving the oncologic treatment with food supplements or extreme dietary strategies. This can be encouraged by family members, acquaintances or online environment(7). Scientific literature which studied the impact of nutrition in oncologic patients claims that the modifications of cellular metabolism which occurred following the carcinogenesis cannot be treated by diets and food supplements. As such, Otto Warburg and Pavlides have demonstrated that in order to fight the malignant metabolism, patients with breast cancer must have a low carbohydrates diet (40-50%), slightly altered protein input (25-35%), and small lipids input (15-20%)(8).
Also, the WHEL study performed by Pierce and col., and the study developed by Willet and col. proved that vegetarian and/or vegan diets did not increase the life expectancy and did not lead to a better therapeutic response(9,10). This proves the development over time of a tumor resistance despite the administration of adequate treatment according to the type of tumor(11). These subjects will be approached in a more comprehensive study.
Conclusions
Our general findings suggest that it is imperiously necessary the approach of knowledge regarding breast cancer among women regardless of their intellectual level or their origin. Also, an essential role for this, but also for the emotional support, can be that of the family physician as an initial factor in the primary assistance, without reducing the supportive role of the family. These efforts can have a positive impact on the early-stage diagnosis of mammary neoplasm, treatment guidance, improvement of the quality of life, and on returning the individual back into society.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Ries LAG, Melbert D, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2004. Bethesda, MD: National Cancer Institute, 2007.
- Clark CR, Baril N, Kunicki M, Johnson N, Soukup J, Ferguson K, Lipsitz S, Bigby J. Addressing social determinants of health to improve access to early breast cancer detection: results of the Boston REACH 2010 Breast and Cervical Cancer Coalition Women’s Health Demonstration Project. J Womens Health. 2009; 18:677–690
- Nissen MJ, Tsai ML, Blaes AH, Swenson KK. Breast and colorectal cancer survivors’ knowledge about their diagnosis and treatment. J Cancer Surviv. 2012; 6:20–32.
- Spittler CA, Pallikathayil L, Bott M. Exploration of how women make treatment decisions after a breast cancer diagnosis. Oncol Nurs Forum. 2012; 39: E425–433.
- Chen JY, Diamant AL, Thind A, Maly RC. Determinants of breast cancer knowledge among newly diagnosed, low-income, medically underserved women with breast cancer. Cancer. 2008; 112:1153–1161.
- Maly RC, Leake B, Silliman RA. Breast cancer treatment in older women: impact of the patient physician interaction. J Am Geriatr. Soc. 2004; 52:1138–1145.
- Greene J, Hibbard JH. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J Gen Intern Med. 2012; 27:520–526.
- Pavlides S, Whitaker-Menezes D, Castello-Cros R, Flomenberg N, Witkiewicz AK, Frank PG, Casimiro MC, Wang C, Fortina P, Addya S, Pestell RG, Martinez-Outschoorn UE, Sotgia F, Lisanti MP. The reverse Warburg effect: aerobic glycolysis in cancer associated fibroblasts and the tumor stroma. Cell Cycle. 2009 Dec; 8(23):3984-4001.
- Key TJ, Fraser GE, Thorogood M, Appleby PN, Beral V, Reeves G, Burr ML, Chang-Claude J, Frentzel-Beyme R, Kuzma JW, Mann J, McPherson K. Mortality in vegetarians and nonvegetarians: detailed findings from a collaborative analysis of 5 prospective studies. Am J Clin Nutr. 1999 Sep; 70 (3 Suppl): 5,16S-5,24S.
- Pierce JP, Stefanick ML, Flatt SW, Natarajan L, Sternfeld B, Madlensky L, Al-Delaimy WK, Thomson CA, Kealey S, Hajek R, Parker BA, Newman VA, Caan B, Rock CL. Greater survival after breast cancer in physically active women with high vegetable-fruit intake regardless of obesity. J Clin Oncol. 2007 Jun 10; 25(17):2345-51.
- Daenen LG, Cirkel GA, Houthuijzen JM, Gerrits J, Oosterom I, Roodhart JM, van Tinteren H, Ishihara K, Huitema AD, Verhoeven-Duif NM, Voest EE. Increased Plasma Levels of Chemoresistance-Inducing Fatty Acid 16:4(n-3) After Consumption of Fish and Fish Oil. JAMA Oncol. 2015 Jun 1; 1(3):350-8.

Abstracts for National Conference of Medical Oncology – 19th edition
...
Aspecte CT şi IRM în mielomul multiplu cu compresie medulară – o suită de cazuri
Mihaela Buzoianu, Mugur C. Grasu, Ioana G. Lupescu
Implicarea coloanei vertebrale în mielomul multiplu (MM) poate cauza compresia măduvei spinării (CMS), care este o urgenţă oncologică manifestată prin durere, paralizie şi duce adesea la dizabilităţi, având un impact pro...
Obezitatea şi cancerul de sân
Iuliana Pantelimon, Tiberiu Tebeică
Această lucrare reprezintă o analiză a principalelor studii din literatura de specialitate privind mecanismele moleculare majore în ceea ce priveşte evoluţia neoplasmului mamar la pacienţii obezi. Astfel, mecanismele moleculare fundamentale descrise în literatura respectivă sunt descrise astfel: principalel...
Obezitatea şi cancerul de sân
Iuliana Pantelimon, Tiberiu Tebeică
Această lucrare reprezintă o analiză a principalelor studii din literatura de specialitate privind mecanismele moleculare majore în ceea ce priveşte evoluţia neoplasmului mamar la pacienţii obezi. Astfel, mecanismele moleculare fundamentale descrise în literatura respectivă sunt descrise astfel: principalel...
Melanomul malign ocular – corelaţia evoluţiei clinice cu parametrii biologici şi imunologici
Păsărică Mihai Adrian, Dragosloveanu Christiana Diana Maria, Maria Iuliana Gruia, Gabriela Murgoi, Schmitzer Speranţa, Alexandru Grigorescu
Melanomul malign, deşi relativ mai puţin frecvent comparativ cu restul neoplaziilor cutanate, este responsabil de cele mai multe ...