Terapia personalizata în diagnosticul şi tratamentul neoplasmului bronhopulmonar non-microcelular
Robert Pirker
24 Noiembrie 2015Advanced non-small cell lung cancer (NSCLC)
Personalized therapy
Patient-related factors
-
Performance status
-
Co-morbidity, organ functions
-
Age
-
Gender
-
Side effects of drugs
-
Convenience of administration
-
Patient preference
Tumor-related factors
-
Histological subtype
-
Tumor growth
-
Molecular characteristics
Costs, cost effectiveness, value-based judgements
Signature and mutational processes in human cancer
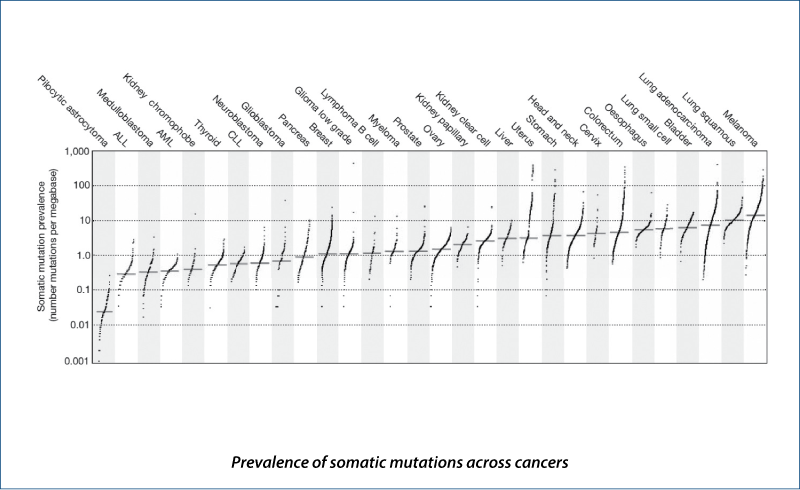
(Alexandrov LB et al. Nature, 2013, 500, 415)
Driver mutations
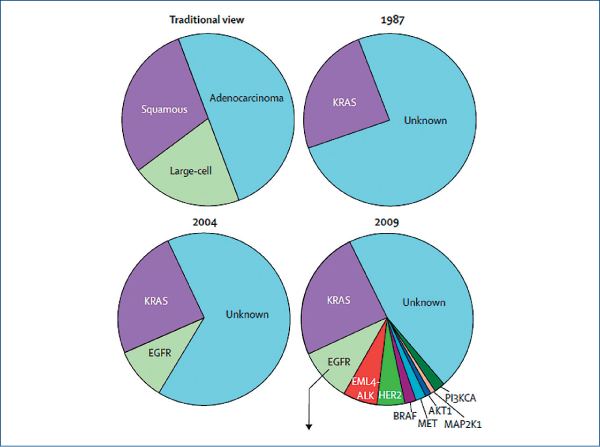
(Pao W and Girard N et al. Lancet Oncol, 2011, 12, 175)
Advanced NSCLC
Status September 2015
EGFR mutation-positive tumors
-
30-60% of Asian patients (adenocarcinomas)
-
10-15% of Caucasian patients (adenocarcinomas)
ALK-positive tumors
-
3-5% of patients (adenocarcinomas)
Tumors without targetable driver mutations
-
Majority of Caucasian patients with advanced NSCLC
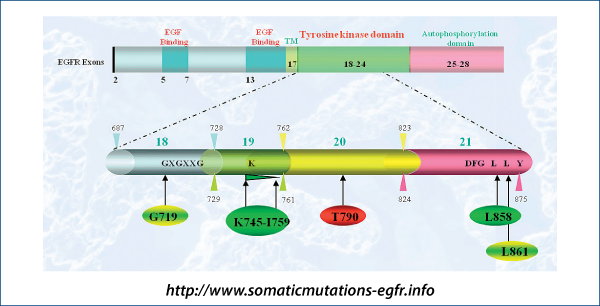
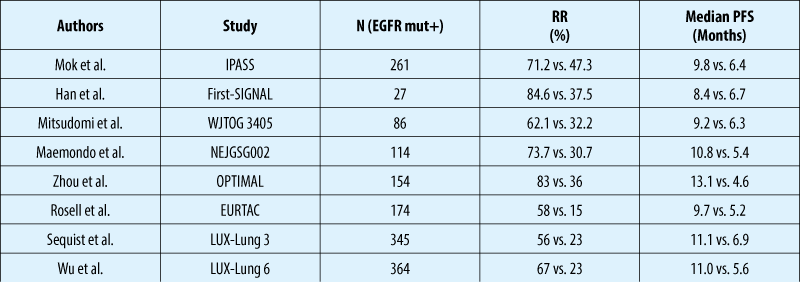
EGFR mutations and response to TKIs
First-line EGFR TKIs vs. chemotherapy in patients with EGFR mutation
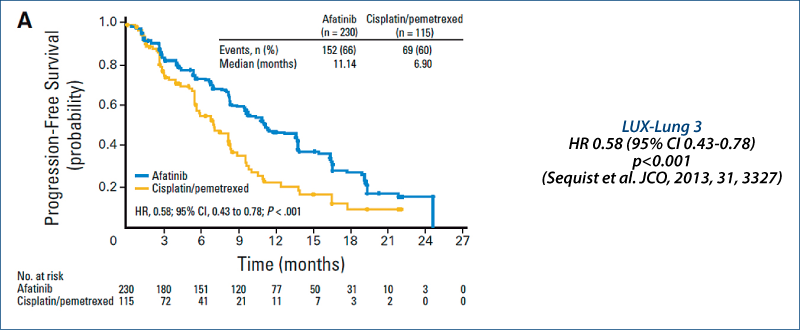
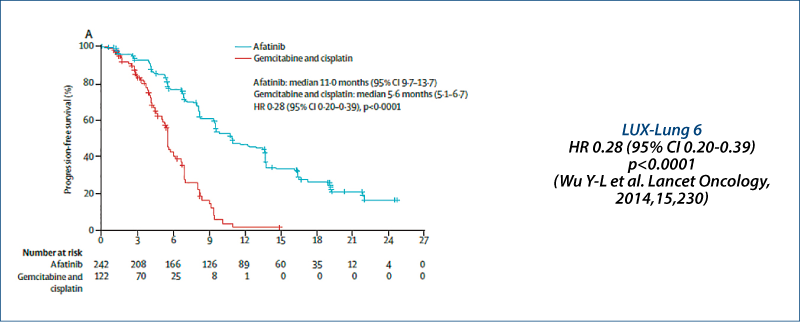
LUX-Lung 3 and LUX-Lung 6: PFS
Independent review
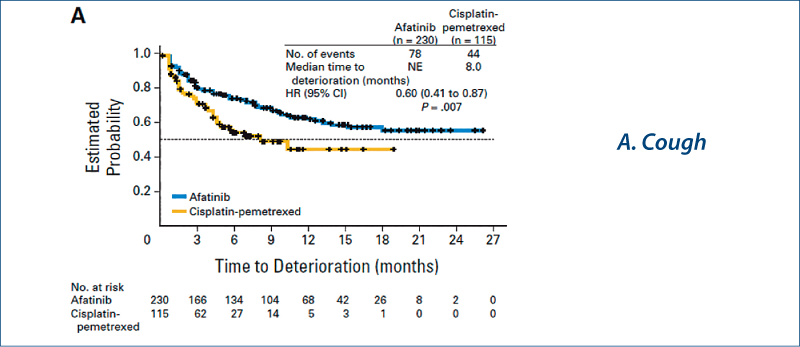
LUX-Lung 3: Quality of life
(Yang JC-H et al. JCO, 2013, 31, 3342)
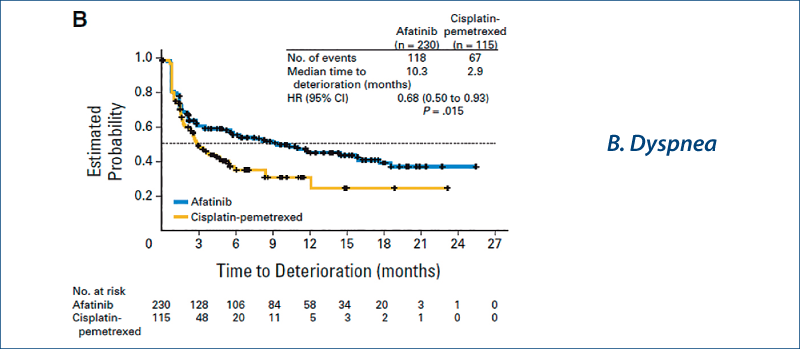
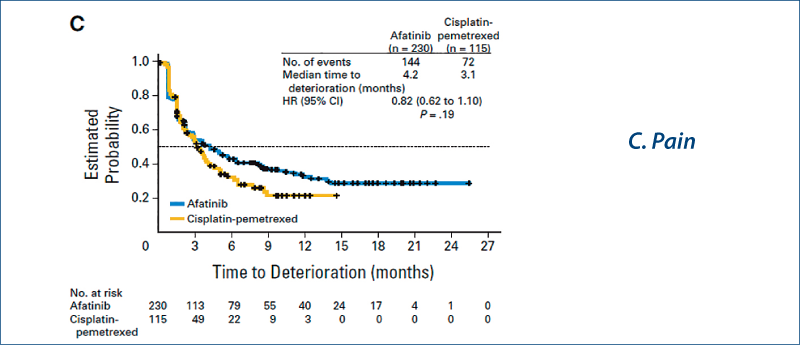
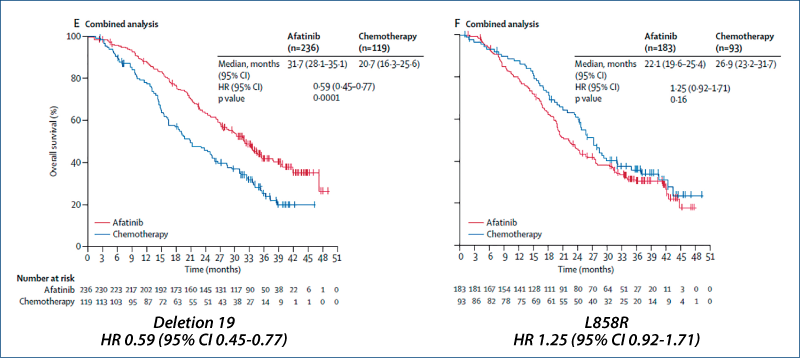
Afatinib vs chemotherapy for EGFR mutation-positive lung adenocarcinoma:
LUX-Lung 3 and LUX-Lung 6
(Yang JC-H et al. Lancet Oncol, 2015, 16, 141)
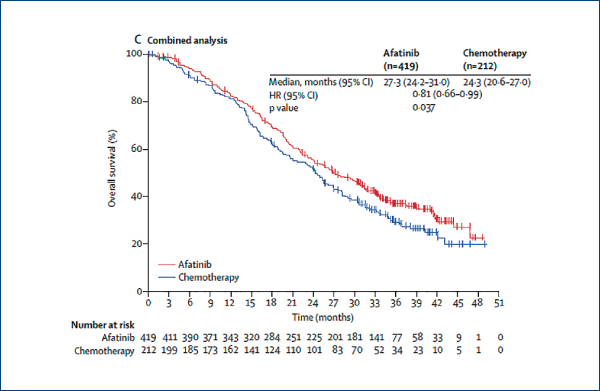
Afatinib vs. chemotherapy for EGFR mutation-positive lung adenocarcinoma:
LUX-Lung 3 and LUX-Lung 6
(Yang JC-H et al. Lancet Oncol, 2015, 16, 141)
Lung cancer
Molecular diagnosis in Europe
EGFR mutation testing has been established
-
European Workshop (Pirker R et al., JTO 2010, 5, 1706)
-
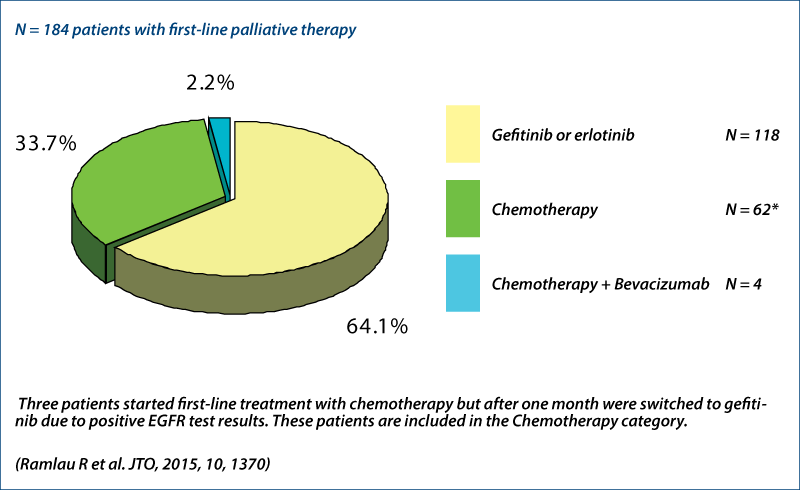
INSIGHT project (Ramlau R et al., JTO 2015, 10, 1370)
Routine KRAS testing in some countries, e.g. Hungary
-
FR TKIs are approved only for KRAS wild-type patientsEG
-
EGFR analysis only in KRAS wild-type patients
ALK analysis
-
IHC screening
-
FISH
French experience (Barlesi F et al., ASCO 2014)
EGFR mutation status
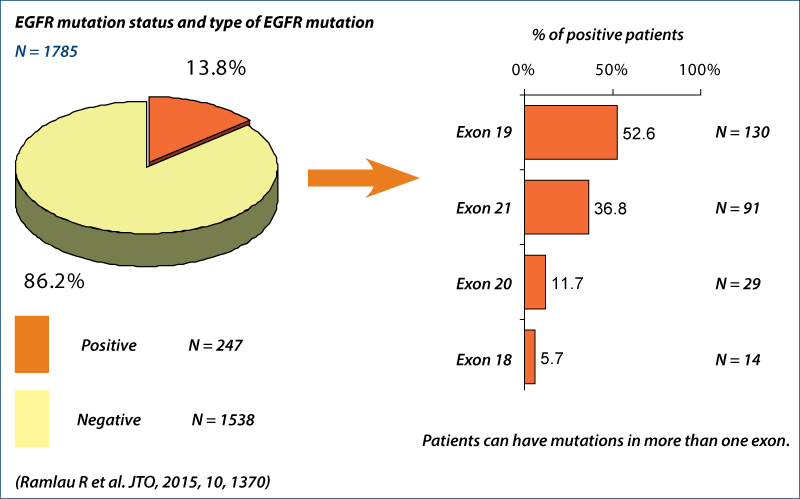
First-line therapy
Adenocarcinoma with exon 19 deletion
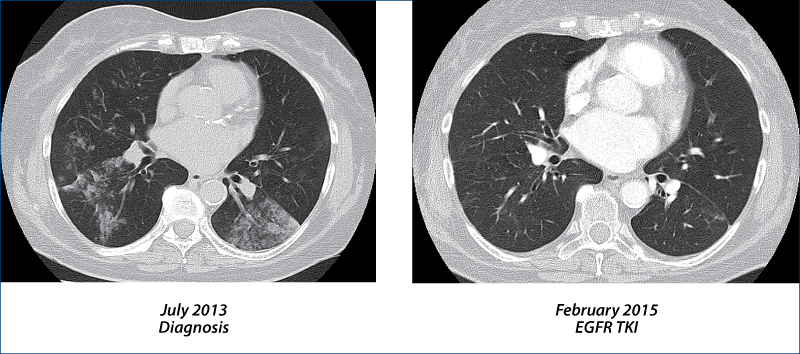
EGFR TKI-resistant NSCLC
(Camidge R et al. Nat Rev Clin Oncol, 2014, 11, 473)
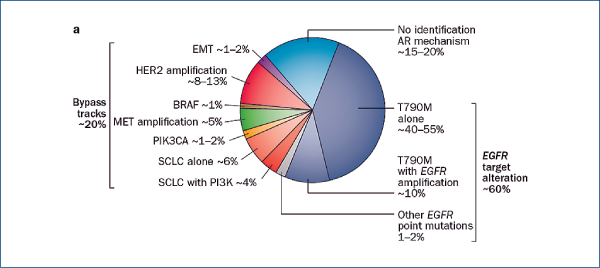
Treatment at time of TKI resistance
Re-biopsy
Treatment
-
Third generation EGFR TKI
- AZD9291, rociletinib (CO-1686), HM61713
-
Switch to chemotherapy with potential re-challenge with TKIs after chemotherapy
-
Continue with TKI
-
Add local therapy to TKI
-
Add chemotherapy to TKI
-
Afatinib plus cetuximab
AZD9291 in EGFR inhibitor-resistant NSCLC
(Jänne PA et al. NEJM, 2015, 372, 1689)
Selective third generation TKI
EGFR mutation-positive patients with acquired resistance to EGFR TKIs (NCT01802632)
Dose escalation and dose expansion cohorts
20-240 mg AZD9291 once daily
Patients (n=253)
Female 62%
Asian 62%
Adenocarcinoma 96%
Prior TKIs median 2 (range 1-5)
Prior chemotherapy 80%
T790M 62%
AZD9291 in EGFR inhibitor-resistant NSCLC
(Jänne PA et al. NEJM, 2015, 372, 1689)
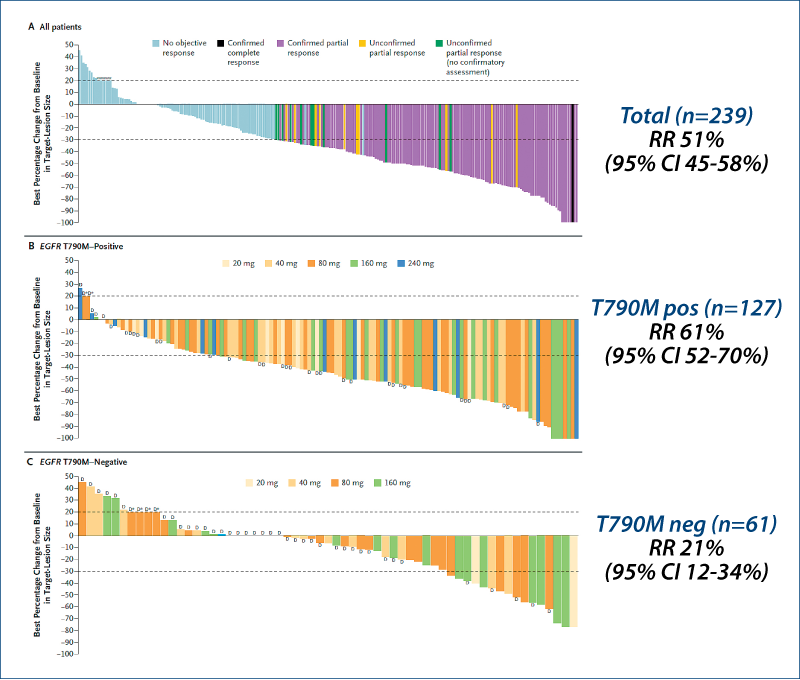
AZD9291 in EGFR inhibitor-resistant NSCLC
(Jänne PA et al. NEJM, 2015, 372, 1689)
No dose-limiting toxicity
AE any grade (grade 3-5)
Diarrhea 47% (2%)
Rash 40% (1%)
Dry skin 20% (0)
Puritus 19% (0)
Paronychia 17% (<1%)
Nausea 22% (<1%)
Decreased appetite 21% (1%)
Fatigue 17% (1%)
AE grade 3-5 32%
AE gr 3-5 drug-related 13%
SAE 22%
SAE drug-related 6%
AZD9291: Clinical studies in EGFR
mutation-positive NSCLC
AURA phase I/II study
AURA 2
-
Phase II trial
AURA 3
-
Phase III trial AZD9291 vs. platin-based chemotherapy in second-line therapy
FLAURA
-
Phase III trial AZD9291 vs. gefitinib or erlotinib in first-line therapy
ADAURA
-
Phase III trial AZD9291 vs. placebo as maintenance therapy
ASTRA
-
AZD9291 in early access program
Rociletinib in EGFR-mutated NSCLC
(Sequist LV et al. NEJM, 2015, 372, 1700)
Selective irreversible 3rd generation drug (activating and T790 mutations)
Phase I study in previously treated patients with EGFR mutation-positive disease (NCT01526928)
CO-1686 free base form up to 900 mg twice daily
CO-1686 hydrogen bromide form 500-1000 mg twice daily
Patients (n=130)
-
Female 77%
-
Asian 15%
-
Prior therapies median 4
-
Prior TKI median 2
-
T790M 57%
Rociletinib in EGFR-mutated NSCLC
(Sequist LV et al. NEJM, 2015, 372, 1700)
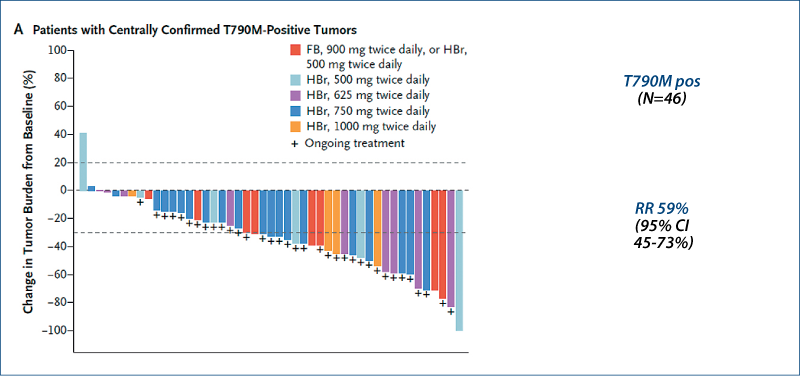
Rociletinib in EGFR-mutated NSCLC
(Sequist LV et al. NEJM, 2015, 372, 1700)
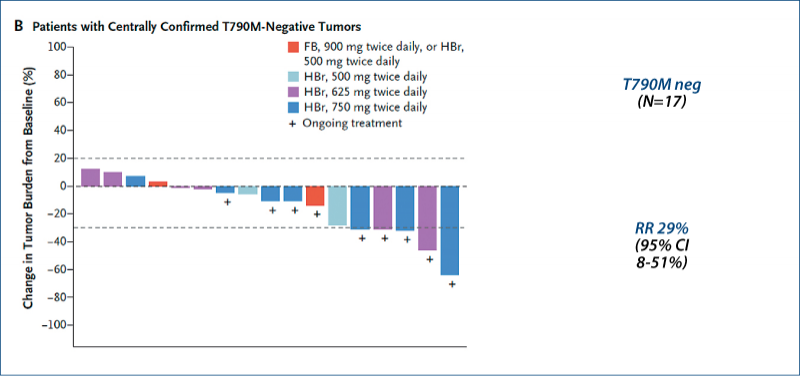
Rociletinib in EGFR-mutated NSCLC
(Sequist LV et al. NEJM, 2015, 372, 1700)
Dose-limiting toxicities were <33% at all dose levels.
Adverse events (all grades)
Hyperglycemia 36%
Nausea 31%
Fatigue 24%
Diarrhea 20%
Decreased appetite 15%
Rash <1%
Hyperglycemia was well managed with oral hypoglycemics and/or dose reduction.
Recommended phase II dose: 750 mg twice daily
3rd generation EGFR tyrosine kinase inhibitors
Summary
Targeting EGFR-activating mutations and T790M mutation while sparing wild-type EGFR
Response rates around 60%
AZD9291
-
Phase III trials: AURA 3, FLAURA, ADAURA
-
ASTRA: Early access program
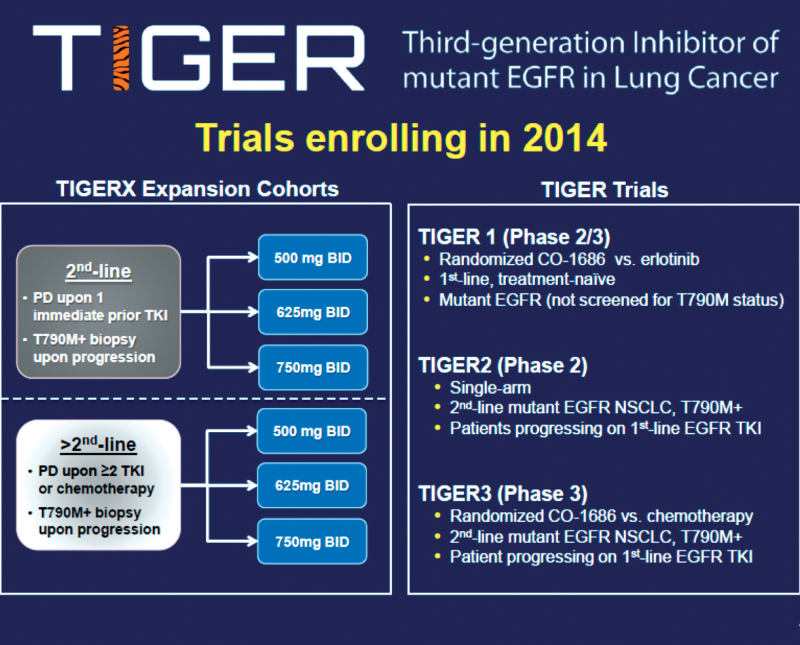
Rociletinib (CO-1686)
-
TIGER trials
HM61713
Crizotinib in advanced NSCLC
EML4-ALK-positive NSCLC

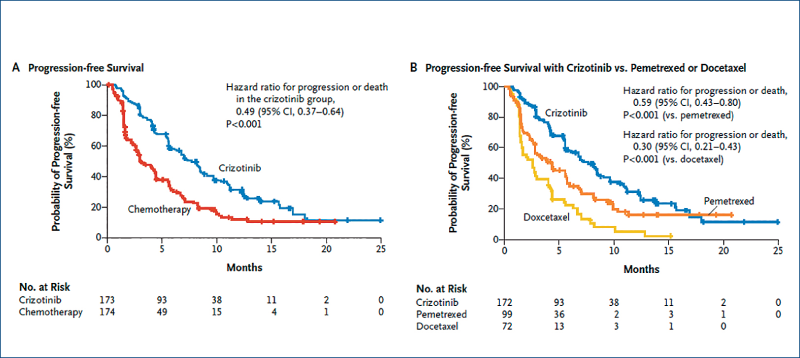
Crizotinib versus chemotherapy in advanced ALK-positive NSCLC: Profile 1007
(Shaw A et al. NEJM, 2013, 368, 2385)
Patients (n=347) pre-treated with chemotherapy
Crizotinib docetaxel or pemetrexed
Response rate 65% 20%
PFS median 7.7 months 3 months
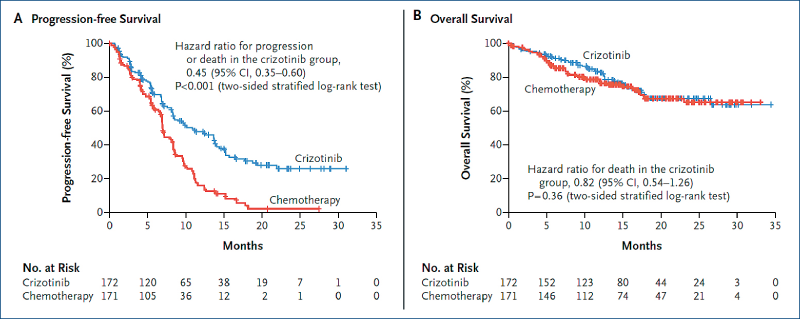
First-line crizotinib versus chemotherapyin ALK-positive NSCLC: Profile 1014
(Solomon BJ et al. NEJM, 2014, 371, 2167)
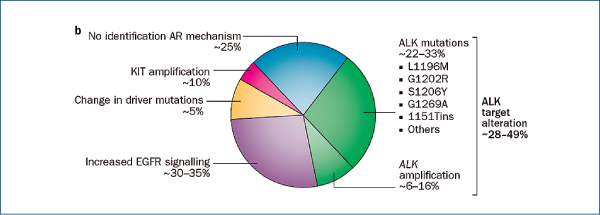
Crizotinib-resistant NSCLC
(Camidge R et al. Nat Rev Clin Oncol, 2014, 11, 473)
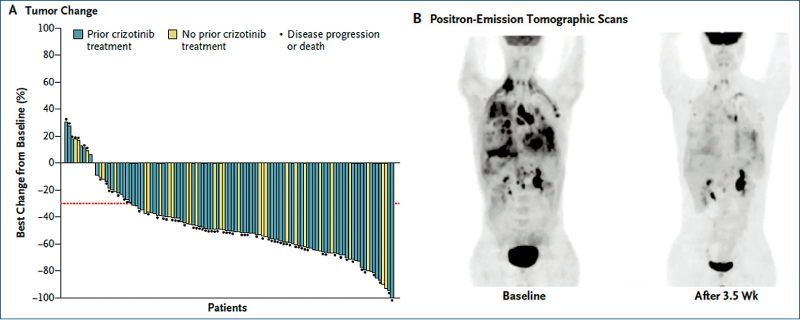
Ceritinib in ALK-rearranged NSCLC
(Shaw A et al. NEJM, 2014, 370, 1189)
Advanced NSCLC
Palliative 1st line chemotherapy
Platinum-based doublets with 3rd generation drug
(vinorelbine, gemcitabine, paclitaxel, docetaxel, pemetrexed, nab-paclitaxel); 4-6 cycles
Symptom relief in approximately 50-60%
1-year survival rate increased by absolute ~10%
Improvement of quality of life (?)
(NSCLC Collaborative Group. BMJ 1995;311:899-909
NSCLC Meta-Analyses Collaborative Group. J CO 2008;26:4617-25)
Performance status affects outcome.
Elderly patients and patients with poor PS also benefit.
-
Well tolerated protocols
-
Enhanced supportive care
Chemotherapy of advanced NSCLC
Recent developments
Novel cytotoxic drugs
Customized chemotherapy based on biomarkers
Changes in administration and/or schedule
-
Oral administration
-
Chronic administration of low doses at regular intervals (metronomic chemotherapy)
Combination with targeted therapies
-
Angiogenesis inhibitors
Bevacizumab
Ramucirumab
Nintedanib
-
Anti-EGFR monoclonal antibodies
Cetuximab
Necitumumab
Bevacizumab in advanced non-squamous NSCLC
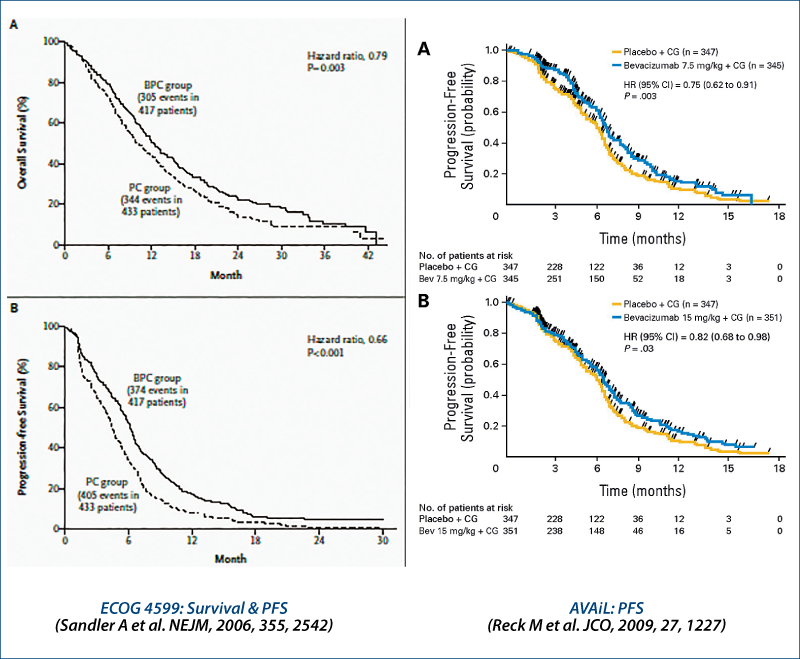
1st line chemotherapy ± EGFR antibodies: survival
1st line chemo ± necitumumab in squamous NSCLC - overall survival
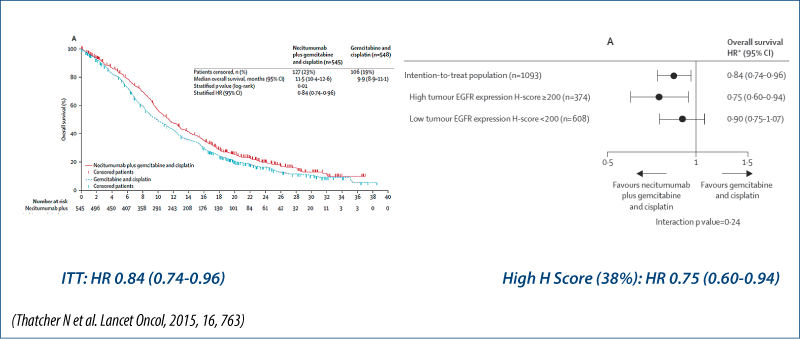
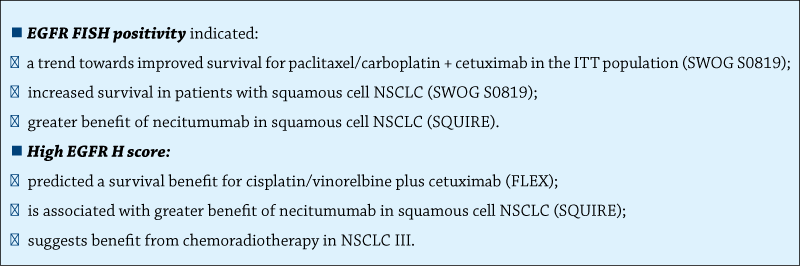
Survival based on biomarkers
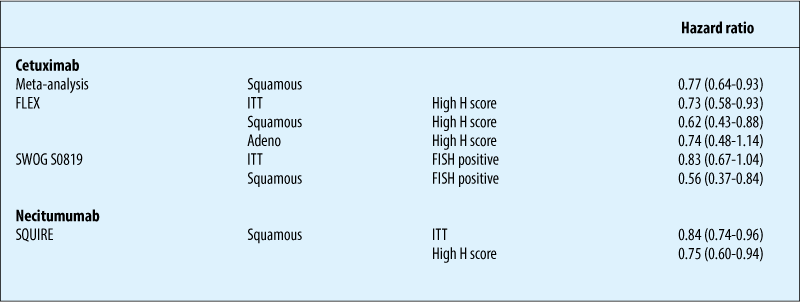
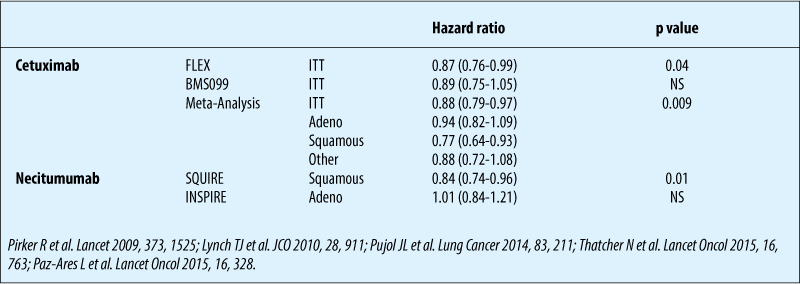
Chemotherapy ± anti-EGFR antibodies: biomarkers
Summary
Maintenance therapy: Phase III trials
Vinorelbine (Westeel V et al. JCNI, 2005, 97, 499)
Gemcitabine
-
CECOG (Brodowicz T et al. Lung Cancer, 2006, 52, 155)
-
US-Studie (Belani CP et al. JCO, 2010, 28, 15s (Abstr 7506))
-
IFCT-GFPC (Perol M et al. JCO, 2012, 30, 35160)
Pemetrexed
-
JMEN (Ciuleanu T et al. Lancet, 2010, 374, 1432)
-
PARAMOUNT (Paz-Ares L et al. Lancet Oncol, 2012, 13, 247)
-
AVAPERL (Barlesi F et al. JCO, 2013, 31, 3004 & Ann Oncol, 2014, 25, 1044)
Erlotinib
-
SATURN (Cappuzzo F et al. Lancet Oncol, 2010, 11, 521)
-
IFCT-GFPC (Perol M et al. JCO, 2012, 30, 3516)
Beva + Erlo (ATLAS) (Johnson BE et al. JCO, 2013, 31, 3926)
Gefitinib (INFORM) (Zhang L et al. Lancet Oncol, 2012, 13, 466)
Palliative therapy in pre-treated patients
Docetaxel
(Shepherd FA et al. JCO, 2000, 18, 2095; Fossella FV et al. JCO 2000, 18, 2354)
Pemetrexed (non-squamous NSCLC)
(Hanna N et al. JCO, 2004, 22, 1589)
Erlotinib
(Shepherd FA et al. NEJM, 2005, 353, 123)
Crizotinib in ALK-positive tumors
(Shaw A et al. NEJM, 2013, 368, 2385)
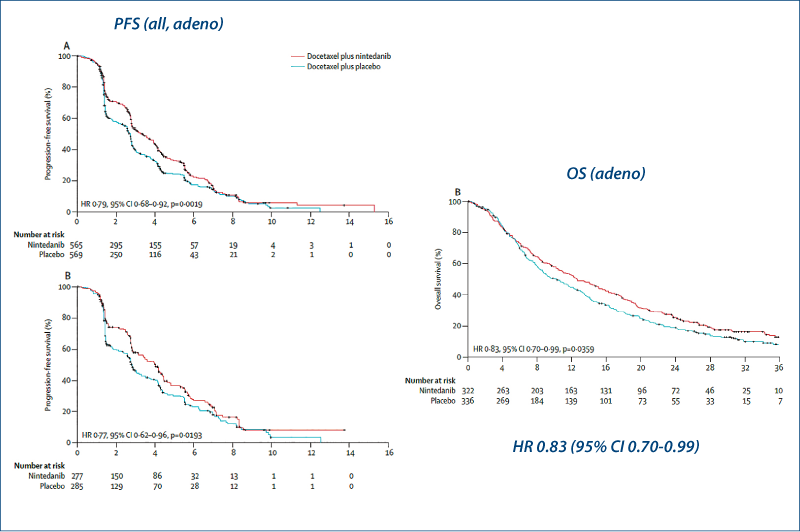
Docetaxel plus nintedanib
(Reck M et al. Lancet Oncol, 2014, 15, 143)
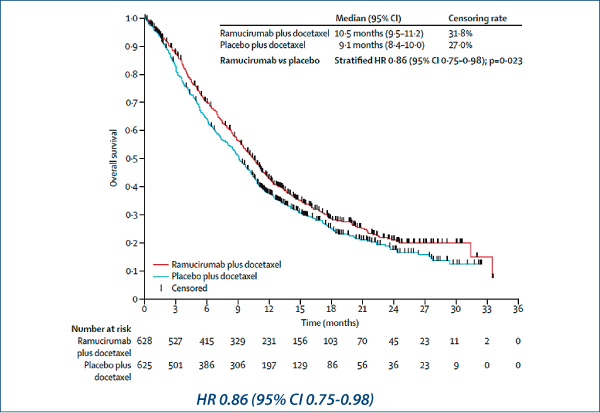
Docetaxel plus ramucirumab
(Garon EB et al. Lancet, 2014, 384, 665)
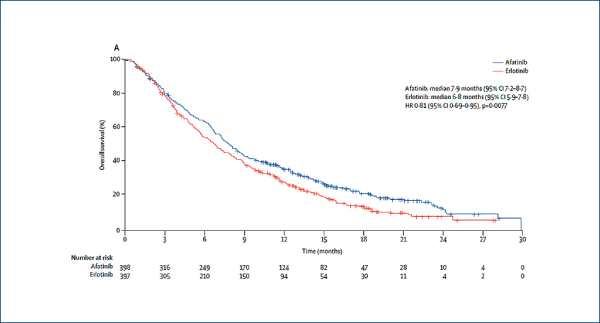
Afatinib in squamous cell NSCLC
(Soria J-C et al. Lancet Oncol, online 6 July 2015)
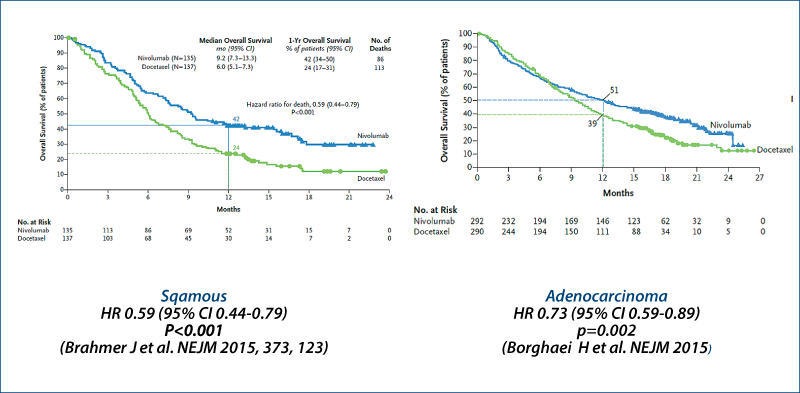
Nivolumab
(Brahmer J et al. NEJM, 2015, 373, 123; Borghaei H et al. NEJM, online 27 Sept 2015)
Docetaxel ± nintedanib: LUME-Lung 1
(Reck M et al. Lancet Oncol, 2014, 15, 143)
Docetaxel ± ramucirumab: REVEL
(Garon EB et al. Lancet 2014, 384, 665)
Afatinib versus erlotinib in squamous cell carcinoma of the lung: LUX-Lung 8
(Soria J-C et al. Lancet Oncol, 2015, online July 6)
Immune checkpoint inhibitors in advanced NSCLC
(Helissey C et al. Curr Opin Oncol, 2015, 27, 108)
Anti-CTLA4
-
Ipilimumab
-
Tremelimumab
Anti-PD-1
-
Nivolumab
-
Pembrolizumab
Anti-PD-L1
-
BMS-936559
-
Atezolizumab (MPDL3280A)
-
Tremelimumab (MEDI4736)
-
Avelumab (MSB0010718C)
Others
Nivolumab vs. docetaxel in advanced NSCLC Survival
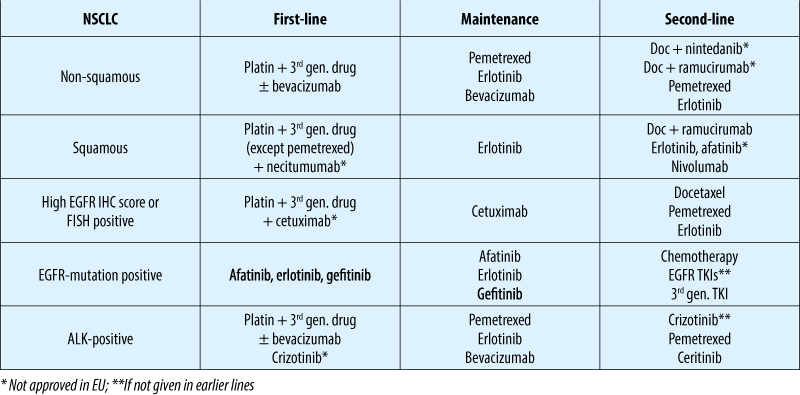
Advanced NSCLC: treatment options (10/2015)

Identificarea de noi markeri moleculari pentru predicţia răspunsului sau a recidivei în leucemia cronică mieloidă, la pacienţi trataţi cu inhibitori de tirozin kinază
Ana Manuela Crişan
Lucrarea reprezintă teza de doctorat a Dr. Ana Manuela Crişan. Cuprinde o parte generală, în care sunt aduse actualizări ale cunoştinţelor în domeniul leucemiei mieloide cronice(LMC) - de la criterii ...
Faslodex in second line of hormonal treatment of advanced breast cancer - case report
Alexandru Grigorescu
Acest caz se referă la o pacientă cu cancer mamar avansat local şi cu metastaze osoase multiple. Pacienta a suferit o intervenţie chirurgicală paliativă (mamectomie de toaletă), radioterapie şi chimioterapie. Ulterior s-a instituit terapia cu un inhibitor de aromatază de generaţia a III-a. După reluarea evolu...
Carcinom bazocelular al unghiului intern al orbitei - prezentare de caz
Bogdan Mircea Măciuceanu-Zărnescu, Elena-Cristina Zeca, Mădălina-Elena Iordache, Iulia Persinaru, Dragoş Cinteză, Raluca Berheci, Ioan Lascăr
Carcinomul bazocelular este una dintre cele mai comune neoplazii cutanate la nivel mondial. Această lucrare prezintă cazul unui pa...
Tratamentul paliativ şi suportiv în cancerul bronhopulmonar avansat
Alexandru Grigorescu
Lucrarea caută să prezinte concis aspecte esenţiale în terapia paliativă şi suportivă a cancerului bronhopulmonar avansat. Se face distincţia între terapia paliativă care abordează pacientul din punctele de vedere esenţiale ale fiinţei umane: fizic, informaţional, emoţional, spiritual şi social, faţă de terap...
Radicalitate versus funcţionalitate în chirurgia oncologică colorectală
Petru Radu, Mircea Brătucu, Dragoş Garofil, Vlad Paic, Mihai Zurzu, Florian Popa, Victor Strâmbu
Ultimele trei decade ale secolului XX au adus o schimbare importantă în abordarea multidisciplinară a cancerului colorectal. De la intervenţii chirurgicale de mare amploare, a căror singură raţiune er...