Dificultăţi terapeutice în carcinomul de cantus medial
Therapeutic difficulties in medial canthus carcinoma
Abstract
The cutaneous neoplasms of the medial canthus are at the intersection of several anatomical regions and, at the same time, of several surgical specialties: ENT surgery, plastic surgery, ophthalmology. The ideal ablation of a malignant lesion of the medial canthus implies negative margins and minimal aesthetic and functional deficit. In this article, we review the literature data on therapeutic principles in medial canthus skin tumors, and we present a clinical case of medial canthus basal cell carcinoma with recurrence after two years from the first surgery. The surgery was performed in a mixed team, and the histopathology result was metatypical carcinoma with basal cell areas. The evolution of the case was favorable, without recurrence after five years of clinical and imaging monitoring. We discuss the therapeutic difficulties raised by a tumor case of medial canthus, insisting that the first surgery must be as radical as possible and with negative margins.Keywords
carcinomamedial canthusradical surgeryRezumat
Neoplasmele cutanate de cantus medial se află la intersecţia mai multor regiuni anatomice şi, totodată, a mai multor specialităţi chirurgicale: chirurgie ORL, chirurgie plastică, oftalmologie. Ablaţia ideală a unei leziuni maligne de cantus medial presupune margini negative şi deficit estetic şi funcţional minim. În acest articol vom trece în revistă datele din literatură privind principiile terapeutice în tumorile cutanate de cantus medial şi vom prezenta un caz clinic de carcinom bazocelular de cantus medial recidivat la doi ani de la prima intervenţie chirurgicală. Tratamentul chirurgical s-a realizat în echipă mixtă, iar rezultatul histopatologic a fost de carcinom metatipic cu zone bazocelulare. Evoluţia cazului a fost favorabilă, fără recurenţă la cinci ani de monitorizare clinică şi imagistică. Vom discuta dificultăţile terapeutice pe care le ridică un caz de tumoră de cantus medial, insistând asupra faptului că prima intervenţie chirurgicală trebuie să fie cât mai radicală şi cu margini negative.Cuvinte Cheie
carcinomcantus medialchirurgie radicalăIntroduction
Basal cell carcinoma (CBC) is the most common skin cancer of the eyelid, being most commonly located on the lower eyelid and on the medial canthus(1). In the group of the cutaneous carcinomas of the face, basal cell carcinomas are most commonly found in the upper two thirds of the face, while in the lower third we find squamous cell carcinomas (SCC) more frequently(2). Both histological forms are related to occupational exposure to ultraviolet radiation(3). In periorbital basal cell carcinomas, the risk factors for orbital invasion are: localization to the medial canthus, male sex, advanced age, anterior recurrence, large tumor size, aggressive histologic subtype, perineural invasion(4).
The surgical treatment is the gold standard. It consists of wide ablation, with clear margins checked intraoperatively and the immediate reconstruction of the resulting defect(5). The difficulties derive from the complex anatomical characteristics of the medial canthus and the lateral portion of the nose root. These features explain the high rate of incomplete resection and the risk of recurrence due to the deep extension of the tumor(6). Different methods have been tried by going to the paraffin sections read in 24 hours before the primary coverage of the defect(7).
The alternatives to surgical treatment are cryosurgery and laser therapy – indicated in very small lesions, limited to the skin as a depth(5). The dermatological treatment by Mohs’ “chemo-surgery” with the extemporaneous microscopic control of the ablation is described as well(5). Also, contact radiation therapy and monoclonal antibodies may represent therapeutic variants in selected cases(2).
The surgical treatment in the carcinomas of the medial canthus with orbital invasion consists in orbital exenteration, which is the treatment of choice(6). The preservation of the eyeball can be tempted in selected patients(8). Radiotherapy and chemotherapy are adjuvant therapies for advanced cases, but may also have a curative visa in cases considered inoperable, but without maintaining a functional eyeball(9).
The prognosis of basal cell carcinomas of the medial canthus is reserved, being difficult to achieve the oncological radicality with a functional and aesthetically acceptable result for the patient(1,3). The therapeutic success consists in the lack of recurrence, the conservation of a functional eyeball and a good quality of life(4).
Case report
We present the case of a 47-year-old female patient from the rural area, with a long occupational exposure to the sun (in agriculture). The patient was diagnosed with CBC of the medial canthus of the right eye, operated 8 years ago in a plastic surgery department from another hospital, and she presented affirmative local recurrence after two years from the surgery. At the clinical examination, she presented an ulcerous-infiltrative lesion at the internal angle of the right eye, with tear fistula through the tumor invasion of the underlying tear sac. We also observed a discrete facial asymmetry through the tumor invasion of the origin of the dilator of the nostril and upper lip lift muscle (Figure 1).

No palpable clinical adenopathy was detected in the cervical lymph nodes. At the palpation of the ulcerous-infiltrative lesion, an extension of the indurated structures at the level of the internal orbital quadrant was detected. The motility of the right eyeball was discreetly limited to the adduction, but also to the abduction, suggesting the infiltration of the right internal eye muscle.
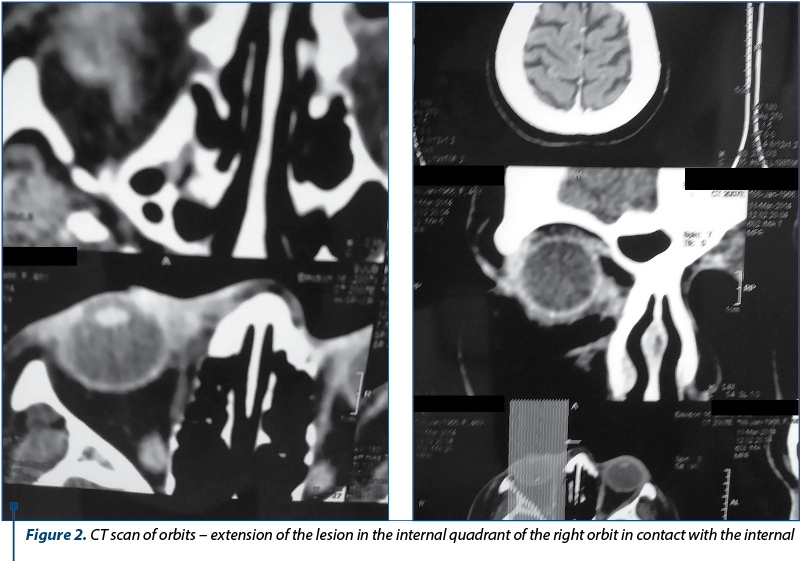
The craniocerebral and orbit CT-scan examination allowed a correct assessment of the tumor and confirmed the invasion into the orbital internal quadrant, in direct contact with the ocular internal right muscle. Also, the lacrimal fossa was occupied by a tumoral content that enhanced with the contrast substance (Figure 2).
We decided to have surgery in a mixed team: ENT surgeon, ophthalmologist and plastic surgeon, under general anesthesia. Tumor ablation was performed within the oncological limits with clear margins (Figures 3 and 4) and we performed the covering of the substance defect with sliding palpebral flaps. The tumor ablation with clear margins (oncological limits) included the lacrimal sac, the medial canthal tendon and orbital fat, the ocular internal muscle being non-macroscopically invaded and only in contact with the tumor mass.


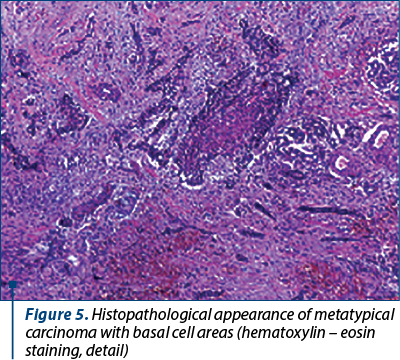
The histopathological result was: metatypical carcinoma, with basal cell areas with a limit of 1 mm in depth (Figure 5).
The tumor board for this patient decided that there was no need for adjuvant therapy.
The local evolution was slowly favorable, with a very good functional result regarding the motility of the eyeball and visual acuity, which were within normal limits at about 14 days postoperatively. We considered the aesthetic result as satisfactory (Figure 6).

The patient was monitored every 6 months during 5 years by clinical examination and CT scan. No local or locoregional relapses were detected.
Discussion
The essential element in the evolution of the patient with CBC of medial canthus is the first surgery, that must be as radical as possible and with negative margins(2,5). Clear margins (oncological limits) are difficult to achieve because of the neighbouring noble structures whose sacrifice leads to aesthetic and functional deficits.
On the other hand, relapse after surgery with positive margins has an increased degree of histopathological and clinical aggression(6). In the case presented by us, the initial histopathological form of CBC turned into metatypical carcinoma, which is a form of transition to SCC, with a higher malignancy, with increased potential for locoregional invasion and distance extension.
The elements of surgical difficulty in the CBC of the medial canthus are related to the need for ablation and re-implantation of the medial canthal tendon, the internal ocular straight muscle, the papyraceous lamina, and the tear duct contents(4).
The surgical technique must ensure the oncological radicality with clear margins, as well as the minimization of the aesthetic and functional deficit, which are sometimes very difficult to achieve.
Conclusions
The most common cutaneous carcinomas of the medial canthus are basal cell carcinomas. The election treatment of medial canthus CBC is surgical and frequently requires a multidisciplinary team. The first surgery must be radical. Frozen sections examination, with control of safety clear margins, is mandatory. The recurrence after surgery with positive margins results in increased aggressiveness of histology and evolution of the tumor. The adjuvant therapy in this type of carcinoma has limited indications and efficacy.
Conflict of interests: The authors declare no conflict of intersts.
Bibliografie
- Yin MT, Merritt HA, Sniegowski M, Esmaeli B. Eyelid and Ocular Surface Carcinoma: diagnosis and management. Clin Dermatol. 2015 Mar-Apr; 33(2):159-69.
- Sagili S, Yin V, Esmaeli B, O’Donnel B, Eckstein R, Mallotra R. Squamous Cell Carcinoma of the Caruncula. Ophthalmic Plast Reconstr Surg. 2015 Jul-Aug; 31(4): e80-2.
- Gonzalez F, Garcia A. Periocular basal cell carcinoma. Arch Soc Esp Oftalmol. 2005 May; 80(5):275-82.
- Leibovitch I, McNab A, Sullivan T, Davis G, Selva D. Orbital invasion by periocular basal cell carcinoma. Ophthalmology. 2005 Apr; 112(4):717-23.
- Sun MT, Wu A, Figueira E, Huilgol S, Selva D. Management of periorbital basal cell carcinoma with orbital invasion. Future Oncol. 2015 Nov; 11(22):3003-10.
- Iuliano A, Strianese D, Uccello G, Diplomatico A, Tebaldi S, Bonavolonta G. Risk factors for orbital exenteration in periocular Basal Cell Carcinoma. Am J Ophthalmol. 2012 Febr; 153(2):238-241.
- Khandwala MA, Laichan SA, Chang BY, Habib M, Chakrabarty A, Cassells-Brown A. Outcome of periocular basal cell carcinoma managed by overnight paraffin section. Orbit. 2005 Dec; 20(4):243-7.
- Madge SN, Khine AA, Thaller VT, Davis G, Malhotra R, McNab A, O’Donnel B, Selva D. Globe-sparing surgery for medial canthal Basal Cell Carcinoma with anterior orbital invasion. Ophthalmology. 2010 Nov; 117(11):2222-8.
- Papadopoulou C, Solbach MC, Lorenz B, Luciani F. Treatment Options for Basal Cell Carcinomas of the Medial Canthus. Klin Monbl Augenheilkd. 2016 Jan; 233(1):38-43.

Restaurarea directă în zona frontală a distrucţiilor dentare coronare – prezentare de caz
Irina-Maria Gheorghiu, Loredana Gheorghiu, Mihai Mitran, Sânziana Scărlătescu, Alexandru Iliescu, Paula Perlea
Acest articol prezintă o temă de actualitate în domeniul medicinei dentare restaurative: restaurarea directă a distrucţiilor dentare coronare în zona frontală a arcadelor dentare. Aceasta se poate...
Abordarea audiologică a pacientului cu tinitus
Anca Modan, Mădălina Georgescu
În marea majoritate a cazurilor, tinitusul este subiectiv, fiind definit ca percepţia doar de către pacient a unor sunete involuntare, care nu au un corespondent real în mediul sonor înconjurător şi sunt percepute într-una dintre urechi sau în tot capul. Impactul acestor sunete asupra pacientului variaz...
Ameţeala indusă de anxietate
Cristina-Maria Goanţă, Vlad Andrei Budu, Andreea Stănciulescu, Gabriela Muşat, Mădălina Georgescu
Tulburările de anxietate reprezintă forma de boli mintale cel mai frecvent întâlnită în SUA, afectând 40 de milioane de adulţi cu vârsta de peste 18 ani, sau 18,1% din populaţie, în fiecare an. Aceste afecţiuni sunt tra.../32 - Maxillomandibular skeletal repositioning and the upper airways.webp)
Repoziționarea scheletală maxilomandibulară și căile respiratorii superioare: rezultate funcționale în cazurile de chirurgie ortognatică
Remus Chirciu, Matei Dumitru, Bogdan Bănică, Mircea Laslău, Rareş Oancă, Lorena Păun, Ionuț Costin, Daniela Vrînceanu
Repoziționarea scheletală maxilomandibulară (MSR) modifică relațiile spațiale ale limbii, palatului moale și pereților faringieni ...
Septoplastia endoscopică – indicaţii, avantaje și dezavantaje
Bianca Buleandra, Simona Georgescu, Remus Chirciu, Rareș Oanca, Lorena Păun, Ionuț Costin, Miruna Bratiloveanu, Ioana Eftime, Mihai Dumitru, Daniela Vrînceanu
Septoplastia endoscopică este o tehnică modernă, minim invazivă, utilizată pentru corectarea deviațiilor septale, oferind o vizua...