Leziunile carioase şi tratamentul acestora la molarii primi permanenţi
Dental caries and their treatment in first permanent molars
Abstract
The present paper reviews the main aspects of the carious process in first permanent maxillary and mandibular molars, as well as the important functions they perform. The characteristics related to the moment of eruption are mentioned, also the morphological and topographic aspects that favor the dental caries in these molars. The article presents the modalities of odontal restoration of carious lesions, other therapeutic approaches, as well as the implications of incorrect restorative treatments.Keywords
first permanent molardental cariescoronal restorationRezumat
Articolul de față trece în revistă principalele aspecte privind afectarea prin procese carioase a molarilor primi permanenți, maxilari și mandibulari, cât și funcțiile importante pe care aceștia le îndeplinesc. Sunt menționate caracteristicile legate de momentul erupției şi aspecte morfologice și topografice care favorizează afectarea prin carie a acestor molari. Sunt prezentate modalitățile de restaurare odontală a leziunilor carioase, celelalte opțiuni terapeutice, precum și implicațiile tratamentelor restauratoare incorecte.Cuvinte Cheie
molar prim permanentcarie dentarărestaurare coronarăThe first permanent molars erupt at the age of 6-7 years, distal to the second primary molars. The mandibular first molar eruption takes place always before the maxillary first molar. They are generally known as “six-year molars”. Starting with this moment of eruption of permanent teeth in oral cavity, children present a mixed dentition on the dental arcades(1). The permanent first molars have a huge importance in dento-maxillary system: they are involved in inter-arcadic relationships, namely Angle’s occlusal relationships, and they contribute to the development of dental arches and restore the proper mastication function affected by the early loss of the temporary teeth. First permanent molars are the teeth most affected by carious processes in the entire oral cavity(2). It is a well-known fact that half of them have dental caries after 3-4 years of life in the oral cavity and about 70% of them are already affected in adolescence(3).
Early affliction by dental caries in first permanent molars is a consequence of:
- The early age of their eruption (at this age the child is not mature and not aware of the importance of proper dental hygiene for all the teeth from dental arcades)(4).
- The lack of information of the parents regarding the existence of the moment of eruption and especially the great importance of the first permanent molar in the occlusion; this lack of information leads to a lack of interest in the health and preservation of this tooth(5).
- The eruption of the first permanent molar takes place without a special symptomatology, it goes unnoticed most of the time and therefore its presence is not observed on the arcade until going to the dentist.
- Very sharp occlusal relief; in time, this relief will change and become more flatten through the dental wear phenomenon. Unfortunately, in the first period of their existence on the dental arcade the occlusal sharp and retentive relief is a decisive factor that contributes to the high affection by dental caries in these teeth.
As mentioned above, the first permanent molars are affected by carious processes from the earliest years of their existence. Unfortunately, the treatment of dental caries at this age (and unfortunately, even in teenagers) cannot be often achieved under the appropriate technical conditions to ensure the complete removal of altered tissues and the avoidance of caries recurrences. Neither the rigorous operator protocol that applies to modern materials by adhesive techniques can be respected in many situations, and so restorations are not performed correctly(6). The failure of these early restorations leads in time to complications:
- Pulpal and periapical complications (acute and chronic pulpal inflammations, acute and chronic apical periodontitis).
- The need for endodontic treatments in children, which can also not be performed rigorously, another source of subsequent periapical complications.
- Fractures of the remaining walls of the cavity as a result of recurrent caries(7).
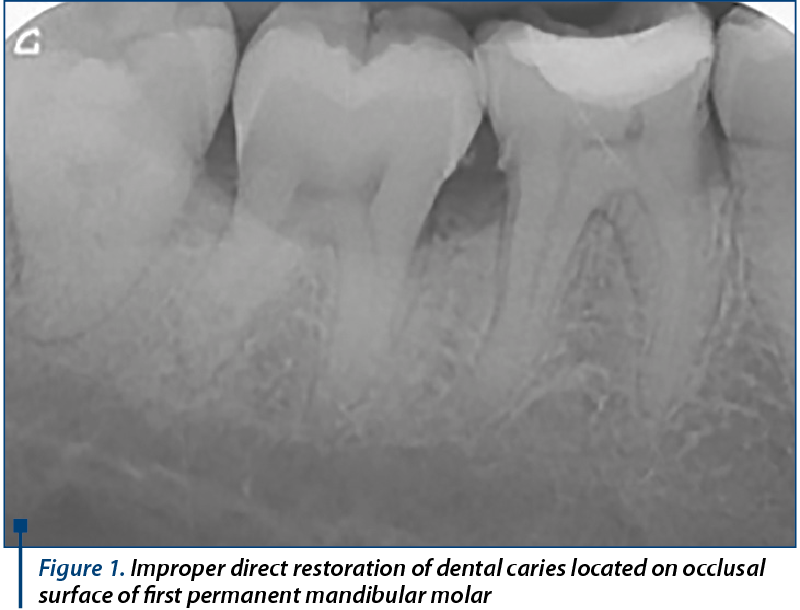
Very often the first permanent molar odontal restorations are achieved without occlusal proper relief, either because the child has not been patient enough for dental treatment, or unfortunately, the dentist did not understand the major importance of dental crown restoration in both his morpho- and functional integrity(8). In fact, restoring the occlusal characteristics is extremely important for these restorations. Unfortunately, the direct restoration of the first permanent molar is often seen as a mere coating of the remaining dental tissue and, in time, the consequence is an important migration of the antagonist tooth, with the mandibular blockage associated with changes in the occlusion plan and malocclusion(9).
Another very frequent situation, especially for the mandibular permanent first molars, is that they are extracted at very early ages as a result of the complications of untreated dental caries. The edentulous space is diminished, but it does not close, and the second permanent molar erupts in a mesial position. At adult age, however, the second molar also suffers a phenomenon of migration by mesial inclination and its periodontal involvement is established. Furthermore, the cohort of complications multiplies, the patients are no longer interested in restoring the edentulous diminished space and the changes of the occlusal relationships lead to the affecting of the adjacent teeth and finally the temporo-mandibular joint is involved.
The first permanent mandibular molar is the most voluminous tooth on both dental arches. It is a molar with two roots (mesial and distal) and a crown with five cusps. The number of channels inside the roots is on average three, with variations between two and four channels.
This is the first permanent tooth that appears in the oral cavity.
The mandibular molar 1 is of particular importance in the dentition due to the following aspects:
- The eruption of the first mandibular molar determines the second important changes in inter-arcadic relationships.
- The mandibular molar has a particularly important role in mastication, determined by its position and occlusal relief.
- The mandibular first molar participates in occlusion stabilization.
- The mandibular first molar contributes to the vertical dimension of occlusion.
- Together with the maxillary first permanent molar, it takes part in an important occlusal mark between the two dental arcades (Angle’s occlusion mark).
Along with the early affliction by dental caries, previously discussed, the specific aspects of odontal pathology related to the mandibular first permanent molar are as follows:
- On the buccal face presents a buccal pit, very retentive, where the carious processes easily started(10).
- The extraction of the first permanent lower molar is difficult, the roots are strong and well implanted in the mandible compact bone.
- Early extraction of the first lower molar is frequent, remains unrestored and determines malocclusion by multiple changes of the occlusal plane by mesial inclination of the second permanent molar and axial migration of the antagonist molar(11).
The first permanent maxillary molar erupts after his counterpart has appeared in oral cavity, also around the age of 6-7 years. It has three roots: two buccal roots (mesiobuccal and distobuccal) and one palatal, and the crown has four cusps. The first maxillary molar holds the most important role in the mastication from all of the upper molars.
The functions of the first upper molar in the dento-maxillary system are as important as its counterpart: together with mandibular first molar it participates in the stabilization of the inter-arcadic relationships and defines the occlusion mark known as Angle occlusion key.
The characteristics of the dental caries occurence and progression in the permanent first maxillary molar are the same as those described in mandibular first molar and are determined by the:
- Early time of eruption on the dental arch.
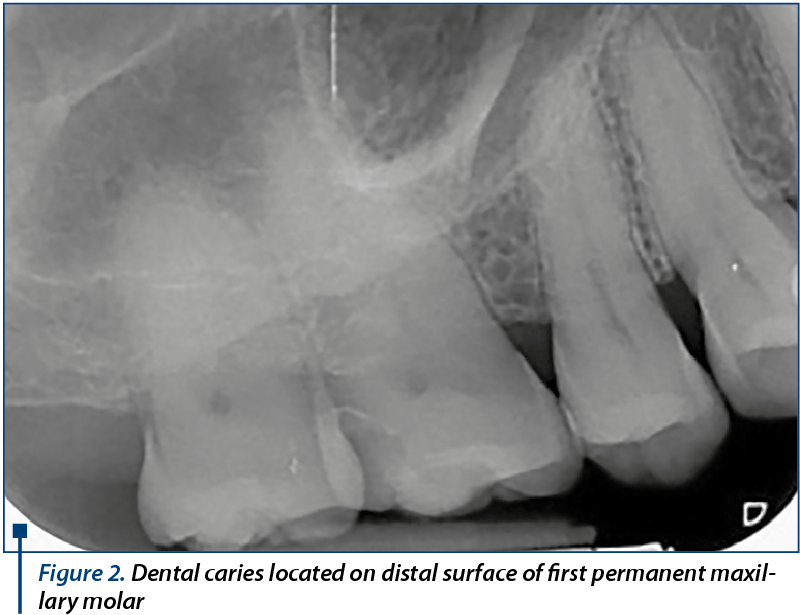
- Retentive occlusal relief with the presence of the distopalatal groove at this level, originating from the distal occlusal area, and which, following an oblique path, ends at the half of the palatal face. This is a very frequent spot where dental caries first appear in first maxillary permanent molar.
The posterior position on dental arcades makes odontal restorative treatments relatively difficult. Statistically, the maxillary first molars are less affected by dental caries than the mandibular first permanent molars, despite the fact that there are very large similarities between them regarding the eruption time and morphological and structural aspects.
The endodontic treatment in the upper first permanent molar is much more difficult to achieve due to root morphology: root canals are curved, difficult to approach and narrow. Any failure of endodontic treatment can unfortunately be complicated with an apical periodontitis and subsequently with odontogenic sinusitis(12).
This aspect of the occurrence of periapical and sinus complications can also be present due to the complete absence of endododontic treatment.
The extraction of the first maxillary permanent molar is easier to achieve than the extraction of the mandibular one because the maxillary bone is more spongy, but accidents of extraction procedure can frequently occur due to close proximity with the maxillary sinus: perforation of the sinus floor and pushing of bone or root fragments into the sinus cavity. In this case, the patient should be reffered to the oro-maxillo-facial surgeon.
Acknowledgements: For this article, all authors have equal contributions.
Bibliografie
- Gheorghiu I. Sănătatea dentară la copii. Editura Universitară „Carol Davila”, București, 2013.
- Iliescu A., Gafar M. Cariologie şi odontoterapie restauratoare. Ed. Medicală, Bucureşti, 2011.
- Srinivasan D, Louis CJ. Evaluation of caries in deciduous second molar and adjacent permanent molar in mixed dentition. J Pharm Bioallied Sci. 2015 Aug;7(Suppl 2):S572-5.
- Burke FJ, Wilson NH, Cheung SW, Mjör IA. Influence of patient factors on age of restorations at failure and reasons for their placement and replacement. J Dent. 2001;29(5):317-24.
- Wapniarska K, Buła K, Hilt A. Parent’s pro-health awareness concerning oral health of their children in the light of survey research. Przegl Epidemiol. 2016;70(1):59-63, 137-40.
- Eskandarian T, Baghi S, Alipoor A. Comparison of Clinical Success of Applying a Kind of Fissure Sealant on the Lower Permanent Molar Teeth in Dry and Wet Conditions. J Dent (Shiraz). 2015 Sep;16(3):162-8.
- Mjör IA, Toffenetti F. Secondary caries: a literature review with case reports. Quintessence Int 2000;31(3): 165–79.
- Popa M.B. Estetică în Odontoterapia Restauratoare. Ed. Univ. „Carol Davila”, Bucureşti, 2006.
- Gosnell ES, Thikkurissy S. Management of dental caries and esthetic issues in the pediatric patient. J Calif Dent Assoc. 2013 Aug; 41(8):619-29.
- Borowska-Strugińska B, Żądzińska E, Bruzda-Zwiech A, Filipińska R, Lubowiecka-Gontarek B, Szydłowska-Walendowska B, Wochna-Sobańska M. Prenatal and familial factors of caries in first permanent molars in schoolchildren living in urban area of Łódź, Poland. Homo. 2016 Jun; 67(3):226-34.
- Cobourne MT, Williams A, Harrison M. National clinical guidelines for the extraction of first permanent molars in children. Br Dent J. 2014 Dec 5; 217(11):643-8.
- Badarne O, Koudstaal MJ, van Elswijk JF, Wolvius EB. Odontogenic maxillary sinusitis based on overextension of root canal filling material. Ned Tijdschr Tandheelkd. 2012 Oct; 119(10):480-3.

Consideraţii epidemiologice şi corelaţia cu complicaţiile gripei la copii în sezonul 2016-2017
Anca Tudor, Mădălina Tomozei, Delia Vlad, Monica Luminos
Pe parcursul epidemiei de gripă din sezonul 2016-2017 mulţi pacienţi pediatrici au necesitat internare pentru complicaţiile gripei, în special cele respiratorii. În acest articol ne vom îndrepta atenţ...
„Măşti cu ecou” - un proiect terapeutic pentru copiii hipoacuzici din România
Magdalena Cernea, Mădălina Georgescu, Alexandra Neagu, Violeta Stan
Articolul prezintă rezultatele proiectului național „Măști cu ecou”, un proiect de terapie prin joc și dramaterapie, desfășurat în România în perioada ianuarie - septembrie 2017. ...
Otomastoidita cronică supurată colesteatomatoasă cu multiple complicaţii - caz clinic
Celesta Drăgulescu, M. Chițac, A. Weisman, Cristina Ancuța, Cătălina Sandu, Diana Deaconu, B. Petrescu
Autorii prezintă un caz de otomastoidită cronică supurată colesteatomatoasă reacutizată cu multiple complicații (pareză facială periferică dreaptă, fistulă Gelle, abces extradural, retroauricular, occ...
Consideraţii epidemiologice şi corelaţia cu complicaţiile gripei la copii în sezonul 2016-2017
Anca Tudor, Mădălina Tomozei, Delia Vlad, Monica Luminos
Pe parcursul epidemiei de gripă din sezonul 2016-2017 mulţi pacienţi pediatrici au necesitat internare pentru complicaţiile gripei, în special cele respiratorii. În acest articol ne vom îndrepta atenţ...
Restaurarea coronară cu rășini compozite utilizând „stamp technique” – prezentare de caz
Irina-Maria Gheorghiu, Mihai Mitran, Loredana Mitran, Alexandru-Andrei Iliescu
Restaurarea directă a pierderilor de substanță dură dentară apărute ca urmare a leziunilor carioase este realizată la ora actuală cu ajutorul materialelor adezive, între care rășinile compozite ocupă...