Tratamentul carcinoamelor de planşeu oral anterior
Treatment of anterior floor of the mouth carcinomas
Abstract
Although the floor of the mouth carcinomas are inferior as percentage as base of the tongue carcinomas, the surgical treatment should be just as radical, with large safe margins and also with neck management. Due to their anterior position, there are easier to diagnose and the patient’s presentation is also in early stages, not only in late stages. Frequently, a mandible resection is required in order to obtain safe oncologic margins. The prognosis is good, with a higher overall survival rate than in other oral malignancies.Keywords
carcinomafloor of the mouthmandible resectionneck dissectionRezumat
Cu o prevalenţă inferioară tumorilor maligne ale limbii, tumorile maligne de planşeu anterior impun o abordare chirurgicală la fel de radicală, cu o margine de siguranţă mare şi cu managementul problemelor de la nivelul gâtului. Datorită localizării lor anterioare, sunt mai uşor de diagnosticat, iar pacientul se prezintă şi în stadii incipiente, nu doar în stadii tardive. Frecvent, este necesară rezecţia mandibulei, pentru a obţine margini de siguranţă oncologică. Prognosticul este bun, cu o supravieţuire generală mai mare decât în cazul altor malignităţi orale.Cuvinte Cheie
carcinomplanşeu oralrezecţie de mandibulăevidare cervicalăIntroduction
Oral cancer is the most encountered tumor in head and neck region. It usually affects male patients in their 6th decade of life(1), a possible explanation for this gender imbalance being related to smoking and drinking, which are more frequent in men. It is age-related, the 5th and 6th decade of life seems to be the most encountered, but in the last years there is a growing tendency in younger adults (30-40 years old, below 30).
Also, strong relations are emerging concerning HPV infection and oral carcinoma, especially the 16th subtype seems to be involved in cancer pathology(2). What is sure is that HPV in oncologic patients is a negative prognosis factor.
Diagnosis
Before developing cancer tumors, patients can present with mucosal lesions such as leukoplakia, erythroplakia or a combination of the two.
Sometimes the onset is missed by the doctor or the patient, as it can mimic numerous benign conditions, but as it develops, the signs of malignancy are more pronounced (solid mass, infiltrative, ulcerated lesion), and it will generally present in one of the two main stages: exophytic or endophytic.
The early treatment leads to better overall survival rate, even up to 80% higher than in advanced stages(3).
For radiological assessment of the cancer patients, the most implied methods are CT scanning for bony invasion and MRI for muscles involvement and to accurately determine the cervical metastasis. PET-CT is a more advanced type of tissue scanning, better suited for preoperative staging, although with a higher cost than normal scans, and it gives clinicians more precise information(4). Cervical metastasis, due to a higher intake of glucose, can be easier detected, as many PET diagnosed occult metastases proved to be malignant at the histological (HP) report, but sometimes negative masses in PET scan were also found to be positive at the HP examination. It is not a total bullet proof investigation, but is a powerful tool when dealing with cancer patients.
Treatment and prognosis
Anterior floor of the mouth malignant tumors are found in less percentage than tongue tumors, accounting for approximately 10% of the oral cancers(5). The treatment implies a surgical phase and adjuvant oncological therapy. Even late stages can be surgically cured and the remaining defects reconstructed with the aid of free flaps. The prognosis depends on the negative resection margins(6), thus having a safe oncological margin of more than 5 mm and lack of margin dysplasia. Even though there are free margins but the dysplasia is present, the risk of tumor relapse increases by up to 50%.
Because there are situated in the proximity of the lingual cortex, in many cases an en bloc mandible resection should be performed even in earlier stages. Usually, a continuity sparing resection is performed; a segmental resection in moderate stages would not grant an extra benefit regarding the oncologic prognosis, but it will inflict a greater impairment for the patient due to muscle attachment loss(7). In early stages, the cervical metastases are not that frequent, but in advanced tumors the neck must be carefully checked. When the diagnosis is N0 for cervical metastasis, depending on the tumor pattern, an elective neck dissection can be performed (SOH dissection), considered to have the same benefits as a radical dissection(8). Most of the cervical metastases are found in the first three lymphatic levels, so a SOH neck dissection will provide a proper outcome. Adjuvant radiotherapy and chemotherapy are performed when positive margins are found, or the tumor has a vascular or neural proliferation. Regarding the cervical metastases, adjuvant therapy is applied when there is a positive carcinoma involvement, irrespective of capsule integrity(9). Radiotherapy as first therapy is employed in advanced stages where surgical cure cannot be performed, as a palliative treatment or for tumor conversion.
The prognosis depends on patient’s age; younger patients under 45 years old have a higher 5-year survival rate, but this is also dependant on the moment of the surgical cure(10). The cervical metastases lead to a decrease in the 5-year survival rate by up to 50%.
The most frequent histological type is squamous cell carcinoma; almost 90% are moderated and well differentiated subtypes(11).
Although in the European Union the mortality due to oral cancer is decreasing, in Romania it seems to be rather opposite, a 10% increase being recorded in the last years(12).
Case 1
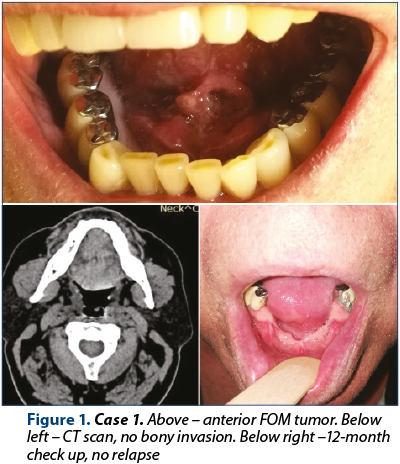
A 63-year-old patient presented for a floor of the mouth (FOM) swelling, with a 3-month duration. The patient had an ulcerated fixed tumor mass with irregular shape and borders, with pain on palpation, without any clinical signs of cervical metastasis. The MRI exam showed a 3/2 cm tumor in the median anterior FOM, without muscle infiltration and no cervical masses. A biopsy was taken (squamous carcinoma) and an en bloc resection with marginal mandible resection was performed, with primary closure. The HP exam: moderately differentiated squamous cell carcinoma stage II, T2NoMxG2. At the 12-month follow-up, no sign of relapse was noted locally and cervical.
Case 2
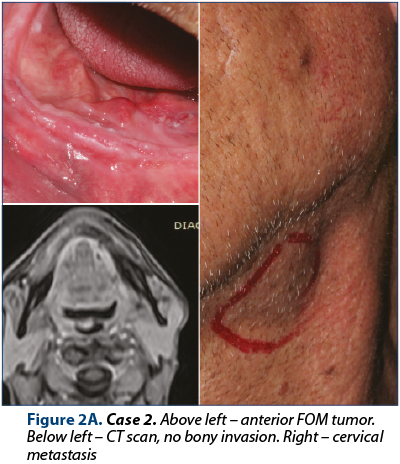
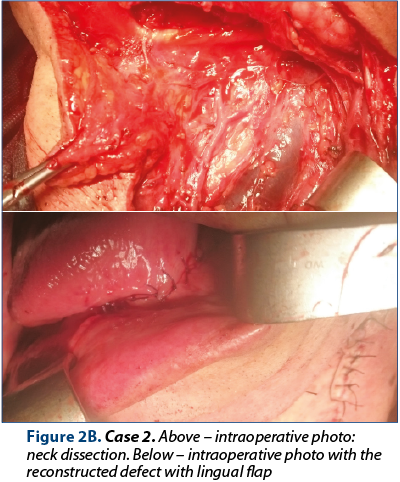
A 71-year-old patient was sent to our department by an ENT colleague for an anterior FOM mass with cervical lymph node involvement. The patient had a 25/30 mm solid mass situated in the anterior FOM, exophytic and ulcerated, that seemed to infiltrate the underlying muscles, with ipsilateral cervical node metastasis. CT scan showed an anterior FOM tumor without bony invasion, but in close contact with the mandible, and left cervical metastasis. A biopsy was performed – squamous cell carcinoma. An intraoral en bloc resection was performed with mandible partial resection and neck dissection, primary closure with lingual flap. The HP exam: moderately differentiated squamous cell carcinoma stage III, T2N1MxG2. Adjuvant oncologic treatment was performed. The patient is tumor-free after 18 months.
Case 3
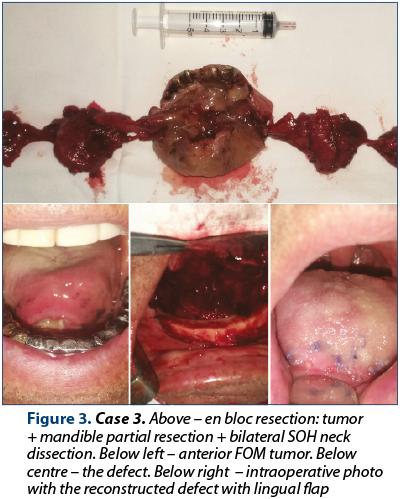
A 73-year-old patient was sent to our department by the general practitioner for an anterior FOM mass, recently developed. A 4/3 cm tumor was observed in the anterior FOM, solid, exophytic, ulcerated, with irregular borders, with lingual alveolar mucosa invasion, without cervical nodes clinically present. The CT scan showed an anterior FOM mass, with muscle involvement, without bone invasion, without node metastasis. A biopsy was performed – squamous cell carcinoma. A pull-through approach was performed, with en bloc resection, with mandible marginal resection, bilateral SOH neck dissection, primary closure with lingual flap. The HP exam: moderately differentiated squamous cell carcinoma stage IVA, T2N2cMxG2. Adjuvant oncologic treatment was performed. The patient is tumor-free after 12 months.
Conclusions
Early stage anterior FOM carcinoma without lymph node involvement can be safely managed with intraoral surgical resection and primary closure or reconstruction with local flaps. In late disease, the approach is combined oral and cervical, or cervical by pull-through procedure, addressing the tumor and the lymph nodes. Adjuvant oncologic treatment is performed, respective of node involvement and tumor pattern and margins.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Lavelle CL, Scully C. Criteria to rationalize population screening to control oral cancer. Oral Oncol. 2005 Jan; 41(1):11-6.
- Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev. 2005; 14:467-75; PMID:15734974; http://dx.doi.org/10.1158/1055-9965.EPI-04-0551.
- Abdo EN, Garrocho Ade A, Barbosa AA, Oliveira EL, Franca-Filho L, Negri SL, et al. Time elapsed between the first symptoms, diagnosis and treatment of oralcancer patients in Belo Horizonte, Brazil. Med Oral Patol Oral Cir Bucal. 2007;12(7):E469–73.
- Hong HR, Jin S, Koo HJ, Roh JL, Kim JS, Cho KJ et al. Clinical values of (18) F-FDG PET/CT in oral cavity cancer with dental artifacts on CT or MRI. Journal of Surgical Oncology. 2014; 110(6), 696–701. http://doi.org/10.1002/jso.23691
- Ariyoshi Y, Shimahara M, Omura K et al. Epidemiological study of malignant tumors in the oral and maxillofacial region:survey of member institutions of the Japanese Society of Oral and Maxillofacial Surgeons, 2002. Int J Clin Oncol. 2008; 13:220–228.
- Pfister DG, Ang K, Brockstein B, Colevas AD, Ellenhorn J, Goepfert H, et al. NCCN practice guidelines for head and neck cancers. Oncology (Williston Park). 2000; 14:163-194.
- Munoz Guerra MF, Naval Gias L, Campo FR, Perez JS. Marginal and segmental mandibulectomy in patients with oral cancer: a statistical analysis of 106 cases. J Oral Maxillofac Surg. 2003; 61:1289-1296.
- Yu S, Li J, Zhang W et al. Efficacy of supraomohyoid neck dissection in patients with oral squamous cell carcinoma and negative neck. Am J Surg. 2006; 191:94–99.
- Yeh SA. Radiotherapy for head and neck cancer. Semin Plast Surg. 2010; 24(2):127-36.
- Pontes FS, Carneiro JT Jr, Fonseca FP, da Silva TS, Pontes HA, Pinto Ddos S Jr. Squamous cell carcinoma of the tongue and floor of the mouth: analysis of survival rate and independent prognostic factors in the Amazon region. J Craniofac Surg. 2011 May; 22(3):925-30. doi: 10.1097/SCS.0b013e31820fe1cb.
- Zakai MA, Ali SM, Aziz M, Islam T. Etiology of Oral cancer/Squamous Cell carcinoma in oral cavity. Ann Abbasi Sha-heed Hosp Karachi Med Dent Coll. 2003 Jun; 8 (1): 48-52.
- Bonifazi M, Malvezzi M, Bertuccio P, Edefonti V, Garavello W, Levi F, et al. Age-period-cohort analysis of oral cancer mortality in Europe: the end of an epidemic? Oral Oncology. 2011; 47(5), 400–407. http://doi.org/10.1016/j.oraloncology.2010.06.010

Abstracte Forum ORL.ro 2019
Lista rezumatelor lucrărilor susţinute in cadul celei de-a XI-a ediţii a Forumului ORL.ro 2019...
Aspectul endoscopic al procesului uncinat
Vlad Andrei Budu
Apofiza unciformă (procesul uncinat) reprezintă lamela anterioară a etmoidului (first lamella), fiind primul reper abordabil chirurgical endoscopic în timpul etmoidectomiei. În mod obişnuit, procesul uncinat se vizualizează prin medializarea cornetului mijlociu, dimensiunea sa permiţând ventilaţia meatului me...
Anomaliile neevolutive de structură ale smalţului dentar
Andrei Kozma, Ioana Monica Teodorescu, Cristian Teodorescu
Prin această lucrare ne propunem prezentarea succintă a anomaliilor neevolutive de structură ale smalţului din punct de vedere clinic şi a etiologiei acestora, precum şi conştientizarea medicului dentist şi a pacienţilor...
Lamboul bicoronal în traumatologia craniofacială
Vladimir Sorin Ibric-Cioranu, Vlad Petrescu Seceleanu
Leziunile calvariei şi orbitei din traumatologia craniofacială reprezintă urgenţe medico-chirurgicale, adeseori timpul chirurgical trebuind să fie de primă intenţie. Lamboul bicoronal reprezintă un abord chirurgical ce facilitează expunerea adecvată a regiunilor frontotemporale şi etajelor superior şi m...
Tratamentul cancerului oral periimplantar
Vladimir Sorin Ibric-Cioranu, Vlad Petrescu Seceleanu, Vlad Andrei Budu
Odată cu creşterea accceptării de către populaţie a tratamentelor implanto-protetice, se va remarca o amplificare a incidenţei carcinoamelor scuamoase mucozale periimplantare. În fazele incipiente, diagnosticu...