Eficacitatea factorilor neurotrofici în tratamentul cazurilor cu demenţă mixtă, vasculară şi Alzheimer, cu multiple comorbidităţi
The efficacy of neurotrophic factors in the treatment of cases with mixed vascular and Alzheimer’s dementia, with multiple chronic comorbidities
Abstract
Alzheimer’s disease is the most common cause of dementia worldwide, its prevalence continuing to grow, partially due to the aging of population. This neurodegenerative disease process is characterized, classically, by the histopathological hallmark of β-amyloid plaque deposition and neurofibrillary tangles of hyperphosphorylated tau proteins. Frequently, concomitantly with the neurodegenerative pathology, a cerebrovascular pathology is associated. The clinical diagnosis may be difficult, but diagnostic methods have been introduced and have been proven to be accurate in supporting the clinical diagnosis. On the other hand, given the advanced age of patients, the increased degree of comorbidity with other chronic medical conditions, but also the possible drug interactions raise a number of issues related to the tolerability and safety of drugs used in the treatment of this disease.Keywords
dementia in Alzheimer’s diseasemixed typecomorbiditiesCerebrolysinRezumat
Boala Alzheimer este cea mai comună cauză de demenţă în lume, prevalenţa fiind în continuă creştere, parţial şi din cauza îmbătrânirii populaţiei. Este o boală neurodegenerativă caracterizată prin modificări histopatologice patognomonice: depozite de plăci de β-amiloid şi ghemuri neurofibrilare rezultate din hiperfosforilarea proteinelor tau. Frecvent, concomitent cu patologia neurodegenerativă se asociază şi o patologie cerebrovasculară. Diagnosticul clinic poate fi dificil, însă noi metode diagnostice au fost introduse şi s-au dovedit a fi precise în susţinerea diagnosticului clinic. Pe de altă parte, având în vedere vârsta înaintată a pacienţilor, gradul crescut de comorbiditate cu alte afecţiuni medicale cronice, dar şi posibilele interacţiuni medicamentoase ridică o serie de probleme legate de tolerabilitatea şi siguranţa medicamentelor folosite în tratamentul acestei boli.Cuvinte Cheie
demenţă în boala Alzheimertipul mixtcomorbidităţiCerebrolysinIntroduction
The incidence of neurodegenerative diseases has increased as a direct result of the increasing life expectancy. By far, Alzheimer’s disease is the most common neurodegenerative disorder in the general population, with age being the primary risk factor(1). However, mixed dementia, Alzheimer’s dementia and vascular dementia (VD) are the most frequent types of dementia, which could be related to each other(2). Considering the advanced age of affected individuals, burdened by a diversity of chronic medical comorbidities, besides the efficacy, the practitioners must be concerned about the tolerability and safety of the medications used to treat cognitive impairments(3). So far, the available treatments approved by the Food and Drug Administration (FDA) have shown their limits in improving cognitive symptoms and, consequently, the quality of life of the affected patients(4). Therefore, new agents with a different mechanism of actions are needed to cover these unmet needs.
Case study
A 73-year-old Caucasian female with a long history of intermittent psychiatric treatment, affirmative for depression and anxiety symptoms, and with a previous psychiatric admission for recurrent depressive disorder, was taken by her husband to the emergency department of the Timişoara Psychiatric Clinic for a mixed clinical picture consisting of depressive and cognitive impairment symptoms. Based on psychometric testing corroborated with neuroimaging investigations (MRI), she was diagnosed with dementia in Alzheimer’s disease, atypical or mixed type. The case is a complex one, due to the multitude of psychiatric and chronic medical comorbidities, such as cerebrovascular and metabolic diseases associated with an impressive number of complications affecting different organs. During the hospitalization, besides the specific psychiatric and medical treatment, the patient also benefited from Cerebrolysin® injectable treatment in a total dose of 100 ml (10 ml/day). Both clinical evolution and psychometric measures showed a significant improvement in the cognitive symptoms. Cerebrolysin® has proved excellent efficacy and tolerability in elderly patients concomitantly suffering from several chronic medical conditions.
Medical family history
-
Father – essential hypertension and hypercholes-terolemia.
-
Mother – coronary artery disease.
Psychiatric and medical history
-
Recurrent depressive disorder, current severe episode without psychotic symptoms.
-
Sedative and hypnotic harmful use.
-
Type 2 diabetes mellitus with renal and neurological complications.
-
Essential (primary) hypertension.
-
Chronic ischemic heart disease.
-
Generalized and unspecified atherosclerosis.
-
Obesity due to excess calories.
-
Mixed hyperlipidemia.
Living and working conditions
The patient is living in a rural environment together with her husband, in appropriate conditions. Reportedly, she has a good marriage, her husband is supportive and provides her with appropriate care. They had two children together, which at the moment are working abroad. Currently she is retired, after working for 10 years as a seamstress and another 10 years as a pastry chef.
Alcohol and tobacco use
Nonsmoking, drinking alcohol occasionally (based on self-report).
Physical examination
General appearance – fully conscious, grade 2 obesity (BMI = 39.86).
Vital signs – BP = 130/85 mmHg, HR = 81 b/min, t = 36.4 ˚C.
Cardiovascular – normal heart sounds, no added sounds or murmurs.
Respiratory – bilateral equal air entry with normal vesicular breathing.
Gastrointestinal – no abdominal pain, she denies changes in stool frequency and consistency.
Neurological – discreet paraparesis gait, positive Babinsky reflexes bilaterally, diminished patellar and Achilles reflex, adiadochokinesia; mild dysarthria, dyscalculia, dysgraphia, dyslexia, mild mixed dysphasia; parkinsonism with resting tremors, positive cogwheel rigidity and Noica signs; extrapyramidal hypertonia, shuffling gait, camptocormia and decreased arm-swing.
Psychiatric examination
-
Appearance: cooperative attitude, moderate neglect of self-hygiene, psychomotor retardation, decreased mimicry and gestures expressiveness, slightly slurred speech with lack of spontaneity and productivity, mild impairment of prosody.
-
Moderate disorientation, especially to space, with some degree of fluctuation in sensorium mainly during the evening (as the specific treatment progressed, these fluctuations improved).
-
Perception: multiple somatic complaints, especially atypical painful symptoms.
-
Mood: mixed depression and anxiety alternating with transitory periods of irritability.
-
Affect: pathological crying, anhedonia.
-
Difficulty in concentration and calculation.
-
Predominantly, impairment of recent memory and mild difficulties with remote memory.
-
Slow thinking, the patient speaks only when questions are asked, difficulties of abstract thinking, poverty of the informational content of thinking, secondary hypochondria, delusion of prejudice secondary to memory impairment.
-
Lack of spontaneity, curiosity and interests, with stereotypies and perseveration of thoughts and behaviors.
-
Insight: partially present.
Investigations
Nerve conduction velocity test (NCV): 40 m/s.
Blood tests: cholesterol = 234 mg/dl, creatinine = 2.1 mg/dl, uric acid = 8.1 mg/dl, blood sugar level =171 mg/dl.
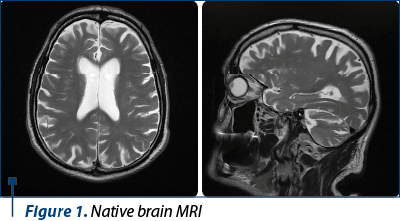
Native brain MRI: the brain MRI (native, without contrast medium) revealed in the T2 and FLAIR sequences a few hyperintense bilateral lesions. Some of them presented correspondence on the DWI sequences; the imaging was suggestive for old ischemic lesions (situated in the white brain matter, in the carotid arteries territories) and a few acute left frontal infarcts, with a maximum diameter of 5 mm.
The ventricles were symmetric. The patient presented diffuse periventricular white matter and pontine lesions, and moderate diffuse cerebral atrophy predominantly bifrontal. Also, the cisterna magna was enlarged. The vascular imaging revealed the presence of rapid flux. In addition, the MRI displayed a right eye lensectomy (Figure 1).
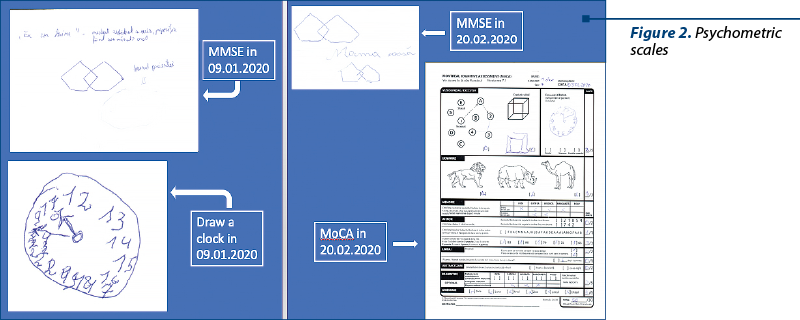
Psychometric scales (Figure 2) – MMSE (Mini-Mental State Examination) – 19 out of maximum 27 (correlated with age and education) in 9.01.2020 (handwriting in Figure 2A is not relevant because it belongs to the resident doctor to whom the patient dictated the sentence) and 27 in 21.02.2020; MoCA (Montreal Cognitive Assessment) – 20 out of maximum 30 in 21.02.2020 (Figure 2B); HAM-D – 28, very severe depression, in 9.01.2020; Beck-Depression Inventory – total score/21: 2.3, meaning severe depression in 9.01.2020, and 1, meaning mild depression in 21.02.2020; CGI-I – 2, meaning much improved, in 21.02.2020.
Positive diagnosis
Dementia in Alzheimer disease, atypical or mixed type, as concluded from the anamnestic data, the history of disease, psychiatric examination, and the paraclinical investigations which comply to the ICD-10 criteria for the aforementioned pathology.
Differential diagnosis
1. Normal aging: through multiple mechanisms, a process of neuronal depopulation takes place in elderly people. The difficulties are not very severe and do not significantly interfere with the patient’s social life and occupations.
2. Vascular dementia (the risk factors for stroke and focal neurological symptoms are present, the progressive deterioration accompanies stroke for a period of time).
3. Pick dementia (memory and concentration impairments, thinking disorders, apathy – abulia background with overlapping outbursts of irritability, instinctual and behavioral disinhibition, anosognosia; frontotemporal atrophy can be observed on brain CT).
4. Parkinson’s dementia (Parkinson’s triad: tremor, bradykinesia and increased muscular tone; the Parkinson’s symptoms appeared at least 12 months before the onset of dementia).
5. Dementia with Lewy bodies (dementia syndrome associated with states of confusion with varying intensity, visual hallucinations and parkinsonian syndrome; the parkinsonian symptoms and dementia occur simultaneously).
6. Huntington’s disease dementia (associated with hypotonic-hyperkinetic syndrome with cognitive impairment and psychotic symptoms).
7. Delirium (acute onset, usually transient, characterized by clouding of consciousness: difficulty maintaining or shifting attention, disorientation, illusions, hallucinatory feelings).
Characteristics: brutal onset, short duration, fluctuations in cognitive impairment during the day, nocturnal exacerbation of symptoms, altered sleep-wake cycle, marked disorders of attention and perception, the immediate memory is specifically disturbed.
Present treatment
Tianeptine 12.5 mg t.i.d., Piracetam® 400 mg b.i.d., trazodone 150 mg 2/3 q.d.p.m., zopiclone 7.5 mg q.d.p.m., sulpiride 50 mg q.d.a.m., Cerebrolysin® 10 ml q.d.a.m. for at least 10 up to 20 days/month, and the treatment of the other medical comorbidities.
Future proposed interventions
Initiating anticholinesterase inhibitor treatment, according to the existing national therapeutic protocols approved by the Romanian Ministry of Health, and continuing the Cerebrolysin® administration at the outpatient psychiatric unit level. Correcting sensory deficits and trying to integrate the patient in a rehabilitation program in a specialized centre (nonpharmacological interventions).
Prognosis
The Alzheimer’s dementia is initially associated with memory impairment that progressively worsens. Over time, the patients with Alzheimer’s dementia can also display anxiety, depression, insomnia, agitation and paranoia. As their disease progresses, the patients come to require assistance with basic activities of daily living, including dressing, bathing and toileting. Eventually, difficulties with walking and swallowing may develop. Feeding may be possible only by gastrointestinal tube, and the difficulty in swallowing may lead to aspiration pneumonia.
The time from the diagnosis to death varies from as little as 3 years to as long as 10 years or more. The patients with early-onset Alzheimer’s dementia tend to have a more aggressive, rapid course than those with late-onset Alzheimer’s dementia. The primary cause of death is the intercurrent illness, such as pneumonia.
Positive prognostic factors: adequate family support – since the last admission, the patient has been compliant to the therapeutic scheme and has presented an improvement in cognitive symptoms, as suggested by the MMSE scale. Negative prognostic factors: associated depression and benzodiazepines harmful use, multiple somatic comorbidities.
Case particularity
This is a complex case, due to the multitude of psychiatric and chronic medical comorbidities, such as cerebrovascular and metabolic diseases associated with an impressive number of complications affecting different organs.
Expected outcome of the treatment plan
-
Ameliorating the cognitive impairment symptoms with temporization of cognitive decline as much as possible.
-
Improving her compliance in taking the medicine.
-
Increasing self-autonomy.
-
More social and recreative engagement.
-
Improving the quality of life.
Actual outcome
-
Maintaining the progress achieved in cognitive functioning.
-
Amelioration of depressive and anxiety associated symptoms.
-
A limited degree of mobility.
-
A limited degree of autonomy.
-
Improving the self-motivation in respecting the prescribed regimen and the medication for diabetes.
Discussion
The preexisting long-lasting affective disorders should be considered as a supplementary risk factor for different types of dementia. Sometimes, depressive symptoms may mask the cognitive decline, especially in elderly patients. The cerebrovascular diseases and neurodegenerative diseases often coexist in the same patients and negatively impact each other. Cerebrolysin® improves, at least for a while, the cognitive symptoms related to dementia progression. The cognitive improvement was objectified based on both psychometric measured tests and subjective experiences. Cerebrolysin® does not interact with other medications used to treat chronic physical and psychiatric illnesses.
Conclusions
Cerebrolysin® is a feasible option for treating cognitive impairments in persons with the mixed form of Alzheimer and vascular dementia. Cerebrolysin® should be considered in patients with dementia and several chronic medical comorbidities. Cerebrolysin® has proved a proper safety and tolerability in treating cognitive impairments in dementia patients with a high physical comorbidity. Cerebrolysin® has shown no interaction with the medication prescribed for chronic medical comorbidities and for diabetes complications.
Bibliografie
-
Trevisan K, Cristina-Pereira R, Silva-Amaral D, Aversi-Ferreira TA. Theories of Aging and the Prevalence of Alzheimer’s Disease. Biomed Res Int. 2019 Jun 16;2019:9171424. doi: 10.1155/2019/9171424.
-
Chui HC, Ramirez-Gomez L. Clinical and imaging features of mixed Alzheimer and vascular pathologies. Alzheimers Res Ther. 2015 Feb 27;7(1):21. doi: 10.1186/s13195-015-0104-7.
-
Thyrian JR, Hertel J, Wucherer D, Eichler T, Michalowsky B, Dreier-Wolfgramm A, Zwingmann I, Kilimann I, Teipel S, Hoffmann W. Effectiveness and Safety of Dementia Care Management in Primary Care: A Randomized Clinical Trial. JAMA Psychiatry. 2017 Oct 1;74(10):996-1004. doi: 10.1001/jamapsychiatry.2017.2124.
-
Hessmann P, Dodel R, Baum E, Müller MJ, Paschke G, Kis B, Zeidler J, Klora M, Reese JP, Balzer-Geldsetzer M. Use of antidementia drugs in German patients with Alzheimer’s disease. Int Clin Psychopharmacol. 2018 Mar;33(2):103-110.

Virgil Enătescu şi Alexandru Dan Ilieş
...
Anxietatea – ce, cum, când şi de ce?
Andrei Buciuta
...
Retrospectiva 2020 a evenimentelor ştiinţifice în domeniul psihiatriei şi sănătăţii mintale din România
...
Îmbunătăţirea abilităţilor somatopsihice şi cognitive într-un caz postaccident vascular cerebral tratat cu factori neurotrofici
Gabriela Marian, Brânduşa Ecaterina Focşeneanu, George-Alexandru Stercu, Andrei-Cristian Bondar, Claudiu Pavel, Adrian Ţînţăreanu
Mood disorders along with cognitive decline are frequents symptoms in stroke survivors. ...
Dual diagnosis – an increasingly frequent clinical challenge in psychiatric practice
Virgil Enătescu, Anca Goldiş, Raluka Albu-Kalinovic, Marius Gliga, Adela Bosun, Oana Stepan, Andreea Sălcudean
Contextul clinic în care o tulburare mintală şi de comportament indusă de consumul unei substanţe psihoactive coexistă cu o tulburare psihică, aparţinând unei alte categorii diagnostice conforme cu ma...