Nefrectomie laparoscopică cu extragerea transvaginală a rinichiului. Primul caz realizat în România – premieră naţională
Laparoscopic nephrectomy with transvaginal extraction of the kidney. The first case performed in Romania – national premiere
Abstract
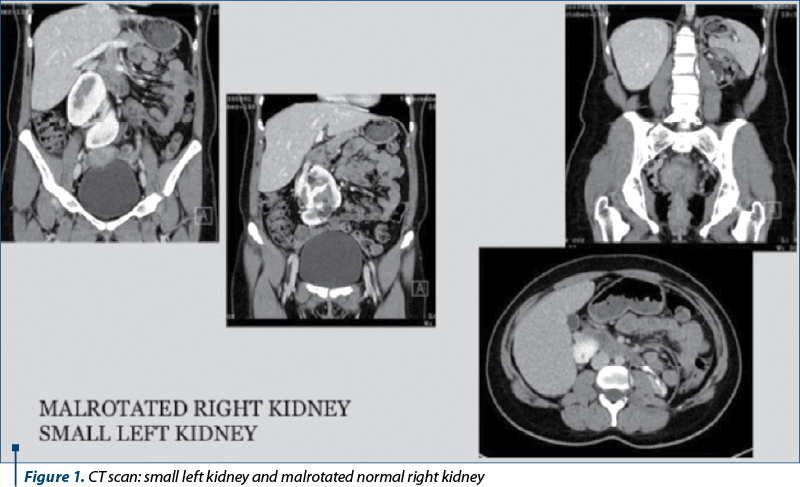
Introduction and objective. We present the case of a 32-year-old female patient who presented in our department (Surgical Department II, “Sfânta Maria” Clinical Hospital, Bucharest) with hypertension due to a small kidney. CT scan revealed a small left kidney and malrotated right kidney, without other pathology; the creatinine level was 0.9 mg%, and renal scintigraphy showed less than 10% function for this kidney. We planned to do the first laparoscopic nephrectomy with transvaginal extraction of the specimen in our country, Romania. Method. We placed the patient in extended flank position. The approach was transperitoneal, with standard trocar placement. After the completion of the primary laparoscopic nephrectomy, we placed the specimen in Douglas pouch. The patient was placed in supine lithotomy position. A transverse posterior colpotomy was performed transvaginally at the apex of the fornix. The peritoneum was opened under laparoscopic view. The specimen was extracted intact transvaginally. The posterior colpotomy was repaired transvaginally. Results. The operative time was 90 minutes. Blood loss was minimal (less than 100 ml). No intraoperative or postoperative complications occurred. The patient was discharged after three days. Hypertension was controlled after nephrectomy without other antihypertensive drugs. The cosmetic aspect was excellent, and the sexual life was perfect after one month. Conclusions. Laparoscopic nephrectomy with transvaginal extraction of the kidney is a feasible and a cosmetically attractive technique, especially for young female patients.Introduction and objective. We present the case of a 32-year-old female patient who presented in our department (Surgical Department II, “Sfânta Maria” Clinical Hospital, Bucharest) with hypertension due to a small kidney. CT scan revealed a small left kidney and malrotated right kidney, without other pathology; the creatinine level was 0.9 mg%, and renal scintigraphy showed less than 10% function for this kidney. We planned to do the first laparoscopic nephrectomy with transvaginal extraction of the specimen in our country, Romania. Method. We placed the patient in extended flank position. The approach was transperitoneal, with standard trocar placement. After the completion of the primary laparoscopic nephrectomy, we placed the specimen in Douglas pouch. The patient was placed in supine lithotomy position. A transverse posterior colpotomy was performed transvaginally at the apex of the fornix. The peritoneum was opened under laparoscopic view. The specimen was extracted intact transvaginally. The posterior colpotomy was repaired transvaginally. Results. The operative time was 90 minutes. Blood loss was minimal (less than 100 ml). No intraoperative or postoperative complications occurred. The patient was discharged after three days. Hypertension was controlled after nephrectomy without other antihypertensive drugs. The cosmetic aspect was excellent, and the sexual life was perfect after one month. Conclusions. Laparoscopic nephrectomy with transvaginal extraction of the kidney is a feasible and a cosmetically attractive technique, especially for young female patients.
Keywords
transvaginal surgerylaparoscopic nephrectomyhypertensionRezumat
Introducere şi obiectiv. Prezentăm cazul unei femei de 32 de ani care s-a prezentat în departamentul nostru de la Spitalul Clinic „Sf. Maria”, Bucureşti, cu hipertensiune cauzată de un rinichi mic. Examenul imagistic CT a evidenţiat rinichiul stâng mic şi rinichiul drept cu aspect normal, dar malrotat. Creatinina serică – 0,9 mg%; scintigrafia renală – funcţie renală sub 10%. Am planificat prima nefrectomie laparoscopică, cu extragerea rinichiului transvaginal, efectuată în România. Metodă. Am poziţionat pacienta în decubit lateral drept cu masă flectată sub rebordul costal. Abordul a fost transperitoneal, cu plasarea standard a trocarelor pentru nefrectomia stângă. După realizarea nefrectomiei laparoscopice stângi, am poziţionat rinichiul în fundul de sac Douglas. Ulterior, pacienta a fost repoziţionată ginecologic. Colpotomia posterioară a fost realizată transvaginal. Peritoneul a fost deschis sub control laparoscopic. Specimenul operator a fost extras intact, transvaginal. Colpotomia posterioară a fost reparată transvaginal. Rezultate. Timpul operator a fost de 90 de minute. Pierderea de sânge a fost minimă (mai puţin de 100 ml). Nu s-au înregistrat complicaţii intraoperatorii sau postoperatorii. Pacienta a fost externată după trei zile. Hipertensiunea a fost controlată după nefrectomie, fără a fi necesar tratament antihipertensiv. Aspectul cosmetic a fost excelent, iar viaţa sexuală a fost reluată optimal la o lună postoperatoriu. Concluzii. Nefrectomia laparoscopică cu extragerea rinichiului transvaginal este o tehnică fezabilă şi atractivă din punct de vedere cosmetic la pacientele tinere.Cuvinte Cheie
chirurgie transvaginalănefrectomie laparoscopicăIntroduction
On January 2017, we performed a left-sided laparoscopic nephrectomy with transvaginal extraction of the kidney. From our data and the extensive research of the literature, this is the first procedure of this kind in Romania and we present this case as a national premiere.
Materials and method
We present the case of a 32-year-old female patient who presented in our department with hypertension (180/90 mmHg) due to a small kidney. CT scan revealed a small left kidney and malrotated right kidney without other pathology (Figure 1). The creatinine level was 0.9 mg%, and renal scintigraphy showed less than 10% function for this kidney.
After a meticulous cardiologic and anesthesiologic evaluation, we planned to do the first laparoscopic nephrectomy with transvaginal extraction of the specimen in our country, Romania.
The standard gynecological evaluation was done.
A transvaginal ultrasonography to assess pelvic organs and pathology of the Douglas pouch (fluid collections, pelvic inflammatory disease) was also performed.
The surgical procedure was extensively explained to the patient. She was informed of the innovative nature of such surgery.
The expected outcomes and potential risks and complications were also discussed. The patient was also informed about the available surgical alternatives before the written informed consent was given.
Surgical technique
We placed the patient in extended right flank position. The abdomen, the external genitalia and the vagina were prepared using povidone-iodine solution and the patient was draped to include those areas. Foley catheter and nasogastric tube were inserted.
The approach was transperitoneal with standard trocar placement. The pneumoperitoneum was insuflated with a Veress needle. Only three trocars were used.
First, a 12-mm trocar for the optics was introduced 5 cm lateral and superior to the umbilicus. The second 12-mm trocar was placed at a point midway between the umbilicus and the anterior iliac spine. The third 5-mm trocar was inserted under the left subcostal space(3).
The abdominal cavity was examined and the pelvis was also examined in order to confirm the intraperitoneal viability of a transvaginal delivery of the kidney.
Told’s fascia was opened and we continued with mobilization of the left colon to expose the anterior aspect of the left kidney and ureter.
The left ureter was isolated. The Gerota fascia was opened and the upper pole of the kidney was separated from the adrenal gland.
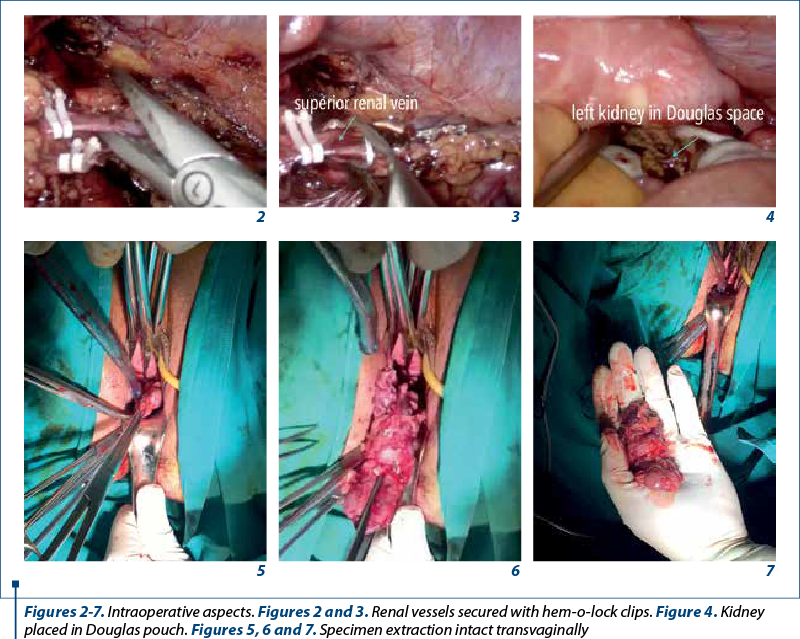
Two left veins and one left artery were also separately isolated, doubled clipped with hem-o-lock clips and divided (Figures 2 and 3).
The left kidney was completely freed and delivered in the Douglas pouch (Figure 4).
The patient was placed in supine lithotomy position. A transverse posterior colpotomy was performed transvaginally at the apex of the fornix.
The peritoneum was opened under laparoscopic view. The specimen was extracted intact transvaginally (Figures 5, 6 and 7). The posterior colpotomy was repaired transvaginally.
Results
The patient received a single dose of first-generation cephalosporin on the operative table.
The operative time was 90 minutes. Blood loss was minimal (less than 100 ml). No intraoperative or postoperative complications occurred.
The patient didn’t require postoperative analgesia. Vaginal pack and Foley catheter were removed on the first postoperative day.
The patient was discharged after three days. Hypertension was controlled after nephrectomy without other antihypertensive drugs. The cosmetic aspect was excellent (Figures 8 and 9) and the sexual life was perfect after one month.
Discussion
Natural orifice translumenal endoscopic surgery (NOTES) has been introduced as a less invasive approach to performing intraabdominal surgery(1,6). Any natural orifice may be used, although the ideal portal remains to be determined. Transvaginal surgery has been performed by gynecologists for decades and there is abundant literature supporting the efficacy and safety using this approach(1). Surgeons have also used the vagina for specimen removal after laparoscopic surgery to minimize the transabdominal incision.
The advantages of transvaginal approach for extracting the kidney are(1,4,6):
-
better cosmesis;
-
expectancy of lower postoperative pain;
-
lower rate of incisional hernias.
The advantages of transabdominal approach are(1):
-
no risk of impairment of sexual function and fertility;
-
no aggression of intimacy;
-
faster recovery.
In 2002, Gill reported a series of 10 laparoscopic nephrectomies followed by vaginal extraction(3).
In 2011, Alcaraz reported a series of 20 living donor laparoscopic nephrectomies with vaginal delivery(4).
However, the technique did not have a great spread, remaining confined to some high specialized centers.
The defenders of the conventional abdominal extraction justified their option with the expectation of lower complication rate, and expressed their concerns about sexual function and fertility(1).
These concerns are probably restraints to the widespread acceptance of transvaginal surgery.
Perioperative complications are negligible when the transvaginal access is created under direct vision(2,3,10) and infections are a rare event(6,9).
The use of transvaginal route to perform a surgical procedure or to remove a surgical specimen is not new.

The general opinion in the literature is that transvaginal approach is the most applied route to extract abdominal or pelvic organs or specimens by virtue of its clinical safety and easy access for opening and closing viscerotomy(1-3,6,7).
The ease of exploration, the cleaning closure and the solution to potential problems have made the transvaginal approach the route of excellence.
The surgical specimen extraction can be done directly or protected with plastic bag(1).
Morcellation is also a commonly used minimally invasive method to extract bulky tissue from the abdomen without extended abdominal incisions(5).
The public perception of the new surgical procedures may not always consider all their potential risks and benefits; however, it is well known the importance of public demand in the evolution of surgical techniques. Population-based surveys found a great acceptance of female public for the transvaginal procedures once safety is assured(4,6).
We want to implement this technique in the future for female cases.
Conclusions
Transvaginal extraction is an effective and minimally morbid technique for removing the intact kidney after laparoscopic nephrectomy(1-3,6,7). The lack of experience in vaginal surgery and the apprehension of long-term effects on sexual function and fertility can be obstacles to the widespread of this technique(1). Morcelation is another alternative for specimen retrieval without the need of wound enlargement(5). Laparoscopic nephrectomy with transvaginal extraction of the kidney is a feasible and cosmetically attractive technique especially for young female patients(2,3). To our knowledge, this is the first of laparoscopic nephrectomies performed in Romania (the surgery was performed on 27.01.2017) in which the extraction route was transvaginal.
Consent: The written informed consent was obtained from the patient for the publication of this case report.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Noguera JF, Martín G, Muñoz JM, Melero M, Sánchez R, Valdivia J, Bruna M, Salvador A, Zaragoza C. Transvaginal approach for nongynecologic intraperitoneal procedures. Int J Cl Med. 2014; 05:1417-29.
-
Breda G, Silvestre P, Giunta A, Xausa D, Tamai A, Gherardi L. Laparoscopic nephrectomy with vaginal delivery of the intact kidney. Eur Urol. 1993; 24:116-7.
-
Gill IS, Cherullo EE, Meraney AM, Borsuk F, Murphy DP, Falcone T. Vaginal extraction of the intact specimen following laparoscopic radical nephrectomy.J Urol. 2002; 167:238-41.
-
Alcaraz A, Musquera M, Peri L, Izquierdo L, García-Cruz E, Huguet J, et al. Feasibility of transvaginal natural ori ce transluminal endoscopic surgery-assisted living donor nephrectomy: is kidney vaginal delivery the approach of the future? Eur Urol. 2011; 59:1019-25.
-
Milad MP, Milad EA. Laparoscopic morcellator-related complications. J Minim Invasive Gynecol. 2014; 21:486–491.
-
Rattner D, Kalloo A. ASGE/SAGES working group on natural orifice translumenal endoscopic surgery. Surg Endosc. 2006; 20:329–33.
-
Gill IS, Advincula AP, Aron M, et al. Consensus statement of the consortium for laparoendoscopic single-site surgery. Surg Endosc. 2010; 24:762–8.
-
Tanaka M, Sagawa T, Yamazaki R, Myojo S, Dohi S, Inoue M. Evaluation of transvaginal peritoneal surgery in young female patients. Surg Endosc. 2013; 27:2619-24.
-
Box GN, Bessler M, Clayman RV. Transvaginal access: current experience and potential implications for urologic applications. J Endourol. 2009; 23:753–7.
-
Dauleh MI, Townell NH. Laparoscopic nephroureterectomy for malignancy: vaginal route for retrieval of intact specimen. Br J Urol. 1993; 72:667–8.

Caracteristicile neonatale după transfer de embrioni fresh sau congelaţi la paciente normogonadotrope, tinere şi sănătoase
Annamaria Virginaş, Bogdan Cârstea, Szidonia Koszeghi, Istvan Barna Nagy, Zolna Virginas, Tamas Korosi, Gabor Vajta
Scop. A evalua dacă transferul de embrioni congelaţi (FET) are efecte benefice asupra greutăţii nou-născutului, comparativ cu tran...
Diagnosticul adenomiozei uterine la pacientele de vârstă reproductivă
Livia Cosma, Corina Gică, George Iancu, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu, Nicolae Gică
Adenomioza uterină este o patologie ginecologică ce este caracterizată de prezenţa insulelor ectopice de ţesut endometrial în miometru. Această boală afectează 20% dintre femeile de vârstă reproduc...
Consideraţii privind abordarea multidisciplinară a tumorilor uterine de tip STUMP
Romina-Marina Sima, Iulia Mărgărit, Anca Daniela Stănescu, Liana Pleș
Introducere. Abrevierea „STUMPs” semnifică tumori uterine netede cu potenţial de malignizare incert, din grupul tumorilor musculare uterine netede (SMT) care nu pot fi diagnosticate cu certitudine ca fiind benign...
Methylation testing: is this the new frontier in cervical cancer screening?
Anca Potecă, Rina Limani, Labinota Kondirolli, Maria Olinca, Elvira Brătilă, Mihai Mitran
Cancerul de col uterin reprezintă o problemă critică de sănătate publică, existând provocări permanente privind screeningul şi detectarea timpurie a leziunilor, afectând ratele de mortalitate la nivel global. ...
Prenatal diagnosis of micrognathia
Calina Maier, Diana Folea, Radu Vlădăreanu, Raluca Tocariu, Marcela Şerban, Mihai Mitran, Elvira Brătilă
Early detection of micrognathia during prenatal care is crucial to mitigate the associated risks and prevent unforeseen emergencies requiring invasive procedures, like tracheostomy....