Agregometria în diagnosticul sindroamelor hemoragipare
Aggregometry in the diagnosis of hemorrhagiparous syndromes
Abstract
Platelet aggregation is one of the first stages in blood coagulation and it represents the phenomenon of interplatelet association under the action of released pro-aggregation factors (ADP, PG, Tx). Platelet agglomeration and union occurs when a blood vessel is injured. The study of platelet function allows assessing both the thrombosis risk and the bleeding risk. Also, it is possible to diagnose platelet disorders due to genetic abnormalities such as Glanzmann thrombasthenia and von Willebrand disease. If an abnormal aggregation pattern is noticed, it is recommended to perform the verification and assessment on another occasion within a time frame specified by the investigator. If aggregation tests are constantly abnormal and it is verified that the patient does not take medicines or substances known to interfere with platelet function, then other complementary tests should be performed.Keywords
plateletsthrombocyteaggregationvon Willebrand factorGlanzmann thrombastheniaplatelet stimulationRezumat
Agregarea trombocitelor este una dintre primele etape în coagularea sanguină şi reprezintă fenomenul de asociere intertrombocitară sub acţiunea unor factori proagreganţi expulzaţi (ADP, PG, Tx). Aglomerarea şi unirea trombocitelor – plachete sanguine – are loc atunci când este lezat un vas de sânge. Prin studiul funcţiei plachetare poate fi evaluat atât riscul de tromboză, cât şi riscul de sângerare. De asemenea, poate fi pus diagnosticul afecţiunilor trombocitului datorate unor anomalii genetice precum trombastenia Glanzmann şi boala von Willebrand. Dacă se observă un model anormal de agregare, se recomandă verificarea şi evaluarea cu o altă ocazie la un interval stabilit de investigator. Dacă testele de agregare sunt persistent anormale şi se verifica faptul că pacientul nu ia medicamente sau substanţe cunoscute care interferează cu funcţia trombocitară, trebuie să se efectueze şi alte teste complementare.Cuvinte Cheie
trombocitplachete sanguineagregarefactorul von Willebrandtrombastenia Glanzmannstimulare trombocitară
Hemostasis defects can be grouped in two categories: bleeding and thrombosis. Factors usually involved in these phenomena are: blood vessel, von Willebrand factor (vWF), platelets, coagulation factors, natural anticoagulants, plasminogen, plasminogen activators and inhibitors (Figure 1).
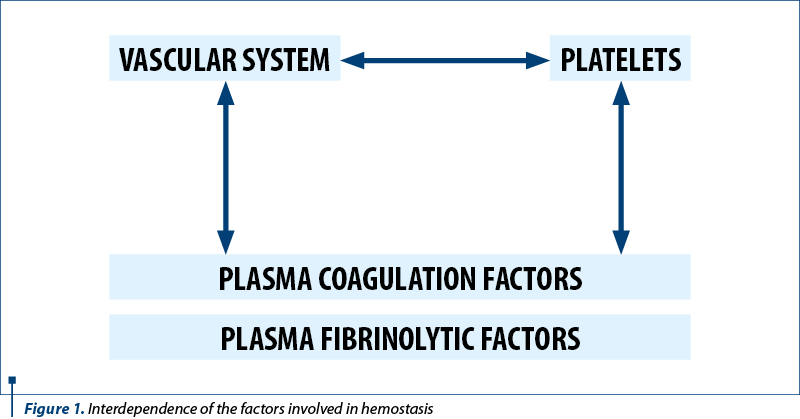
The intact endothelial cell has the functional capacity when stimulated by contact with traces of thrombin or activated platelets to produce antithrombotic substances which will restrict or inhibit the formation of platelet aggregates. The existence of ectonuclease (an enzyme fixed on the endothelium) will transform the ADP released from the platelet aggregates into AMP which decreases/inhibits the aggregation.
The aggregation inductors (ADP, serotonin, PAF, TXA2, thrombin) cause membrane changes that lead to grouping of the GPIIb/IIIa complexes with their conformational change which allows fibrinogen and calcium fixation. In the same time, the coagulation factors are fixed to the surface of platelets, triggering the next stage. The white thrombus results in this way, and it grows in size by attracting and activating other circulating platelets. The entire process is under a control which is limiting its growth.
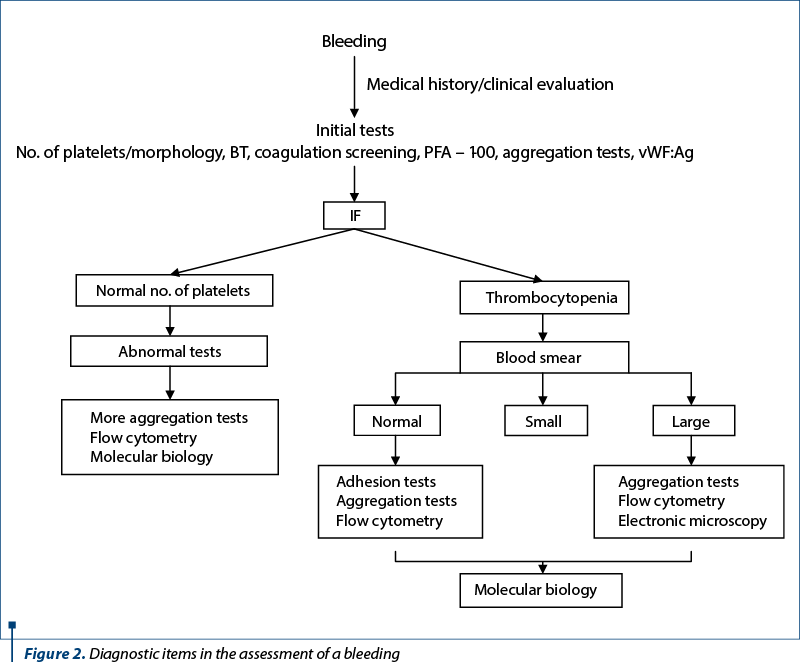
The study of platelet function proves to be the most important diagnostic item in the assessment of a bleeding (Figure 2). Modern investigation methods are applied here with the purpose of assessing both the bleeding risk and the thrombosis risk. The diagnosis of platelet disorders due to genetic abnormalities such as Glanzmann thrombasthenia or von Willebrand disease (vWD) is based on tests such as aggregometry, adhesion tests (PFA – platelet function analyser), or flow cytometry.
Platelet aggregation is one of the first stages in blood coagulation and consists of agglomeration and union of platelets when a blood vessel is injured. In other words, it represents the phenomenon of interplatelet association under the action of released pro-aggregation factors (ADP, PG, Tx).
Platelet aggregation has a mechanism that acts in two stages:
a) platelet activation Þ exposure of GPs which function as receptors for adhesion proteins (e.g., fibrinogen, vWF) Þ adhesion of activated platelets.
b) new layers of platelets are fixed on the initially adhered platelets Þ platelet aggregate.
As a diagnostic value, the aggregometry is a screening test for von Willebrand disease, for diagnosing congenital and acquired well-characterized thrombopathies, as well as for monitoring antiplatelet therapy.
-
ADP ® induces platelet aggregation independent of secretion.
-
EPINEPHRINE (vasopressin) ® explores GPIIb/IIIa.
-
COLLAGEN ® explores the integrity of phospholipids and of membrane receptors, but also arachidonic acid metabolism.
-
RISTOCETIN ® attachment of von Willebrand factor on the platelet receptor.
-
ARACHIDONIC ACID ® explores the Txa metabolism.
-
THROMBIN ® induces platelet aggregation and secretion independent of ADP/prostaglandins.
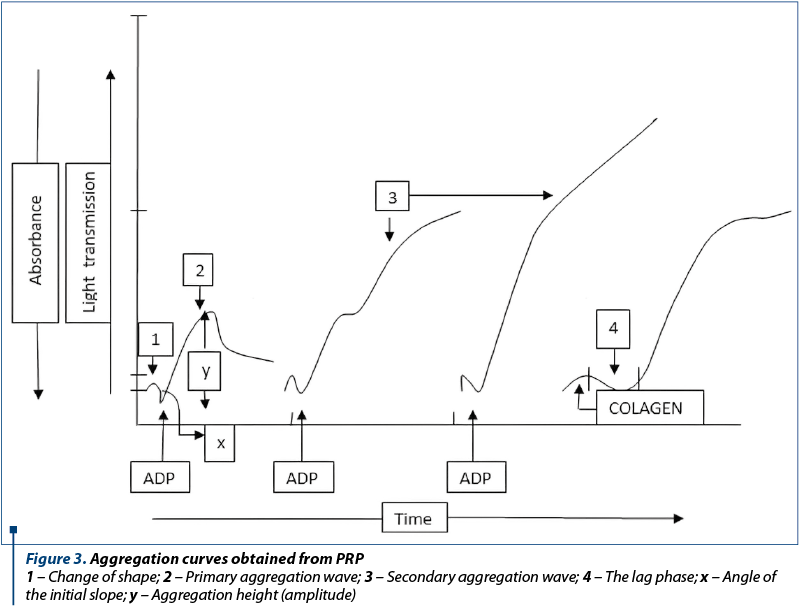
1 – Change of shape; 2 – Primary aggregation wave; 3 – Secondary aggregation wave; 4 – The lag phase; x – Angle of the initial slope; y – Aggregation height (amplitude)
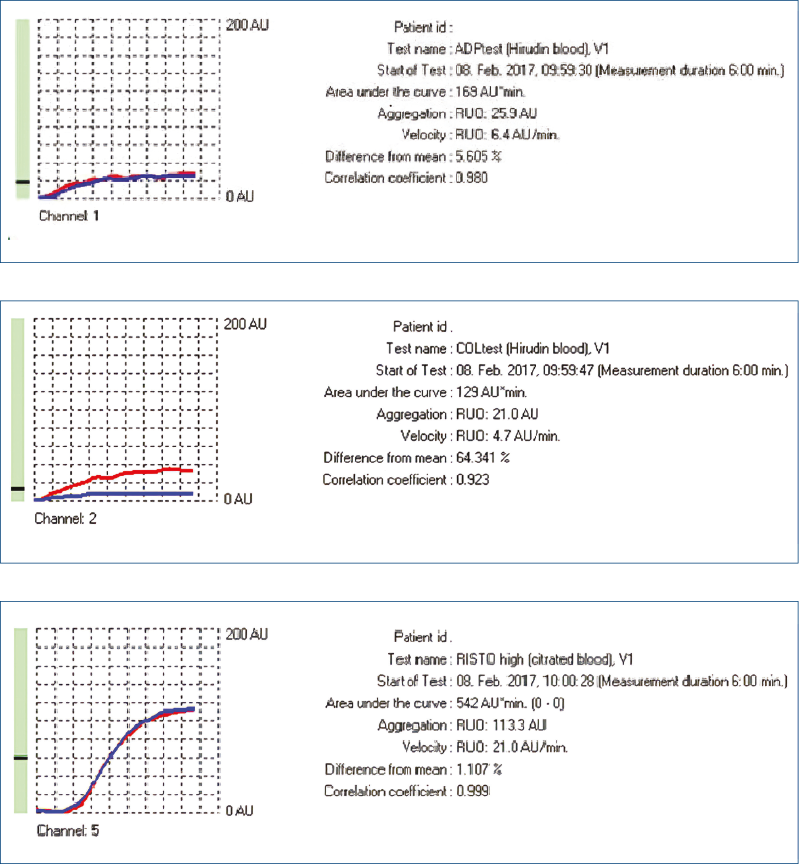
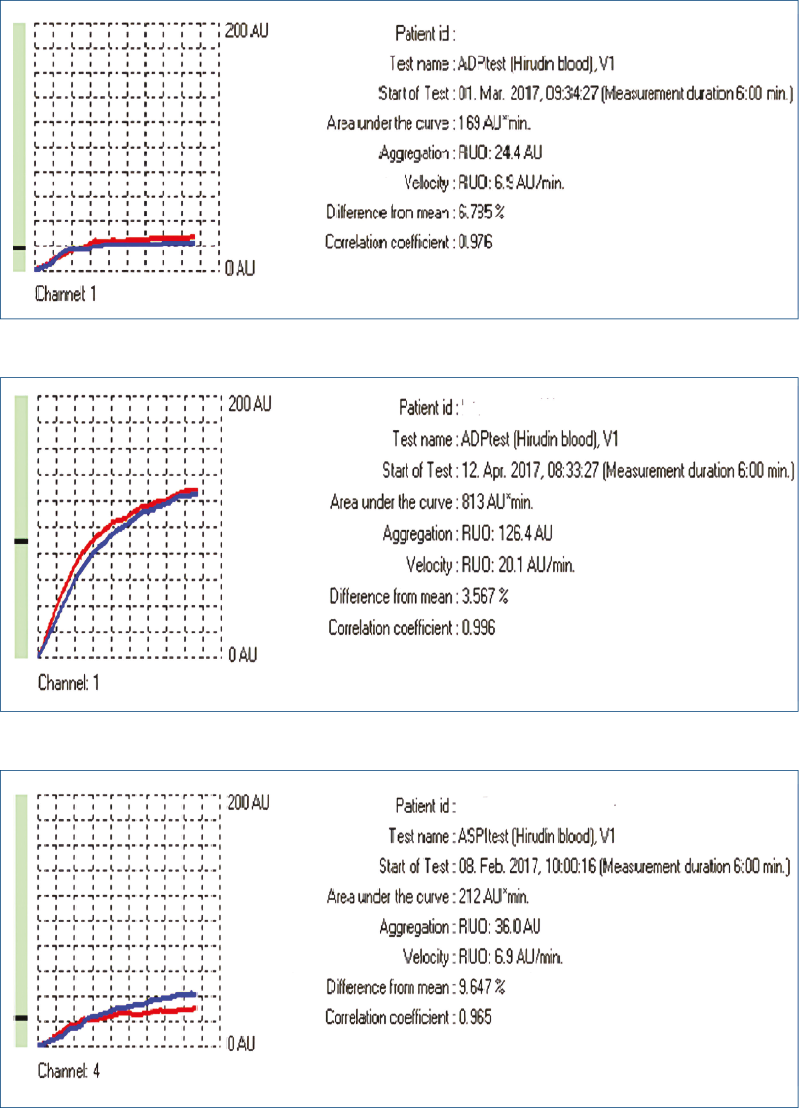
Platelet aggregation has a biphasic pattern at stimulation with ADP and epinephrine (Figure 3). The initial increase is due to primary aggregation as a response to GPIIb/IIIa activation, while the second wave of aggregation is the result of platelet degranulation. Arachidonic acid, collagen and thrombin receptor agonists have a single wave of aggregation. Ristocetin facilitates vWF binding to the GP Ib/IX/V complex, therefore the curve also has two phases of aggregation.
-
The “lag” phase ® shape change of platelets once they are activated.
-
The first wave of aggregation (primary aggregation) ® the direct response of platelets to the aggregating action of the agonist.
-
The second wave of aggregation (secondary aggregation) ® platelet secretion.
-
Normal amplitude of the aggregation curve >60% aggregability.
Hereditary thrombopathies:
A. Hemorrhagiparous thrombocytic dystrophy (Bernard-Soulier syndrome)
B. von Willebrand disease
C. Pseudo-von Willebrand disease
D. Glanzmann thrombasthenia
E. Hereditary deficit of the release reaction:
1. with absent granulations (grey platelet syndrome)
2. with present granulations and activation abnormalities.
Aggregation to ADP, collagen, arachidonic acid, and ristocetin
1. If:
-
the response to platelet stimulation with ADP, collagen and arachidonic acid is weak/absent
-
the response to ristocetin is frequently variable ® Glanzmann thrombasthenia (GT).
GPIIb/IIIa measurement is required (GP mutations are described) by flow cytometry.
2. If:
-
the platelet response to stimulation with ADP and collagen is weak/absent
-
normal response to ristocetin.
The platelet response to stimulation with arachidonic acid is assessed:
-
abnormal response ® effect of aspirin/NSAID ingestion (see below – comparative study)
-
normal response ® storage pool disease (SPD).
Dosing the content of ATP-ADP in granules is required.
3. If:
-
n normal response to platelet stimulation with ADP, collagen and arachidonic acid
-
n absence of response to ristocetin.
vWF assessment is required (Ag, Ab dosing):
-
abnormal – corrected with cryoprecipitate ® vWD
-
normal – GPIb measurement by flow cytometry ® Bernard-Soulier syndrome (BSS).
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Awidi A, Maqablah A, Dweik M, Bsoul N, Abu-Khader A. Comparison of platelet aggregation using light transmission and multiple electrode aggregometry in Glanzmann thrombasthenia. Platelets. 2009; 20(5).
- Cattaneo M. Resistance to antiplatelet drugs: molecular mechanisms and laboratory detection. J Thromb Haemost. 2007; Suppl 1.
- Clinical and Laboratory Standard Institute (CLSI) document H58-A. Platelet Function Testing by Aggregometry. Approved Guideline, 2008.
- Gachet C. ADP receptors of platelets and their inhibition. J Thromb Haemost. 2001; 86.
- Mirkhel A, Peyster E, Sundeen J, et al. Frequency of aspirin resistance in a community hospital. Am J Cardiol. 2006; 98.
- Valarche et al. Multiplate whole blood impedance aggregometry: a new tool for von Willebrand disease. J Thromb Haemost. 2011; 9(8).

Imunoterapia unor anumite tipuri de cancere – scurt review
Alexandru Grigorescu
Imunoterapia îmbunătăţeşte abilitatea sistemului imunitar de a elimina celulele canceroase. Există mai multe tipuri de imunoterapie şi fiecare ajută sistemul imunitar prin mecanisme diferite. În această recenzie sunt prezentate principalele tipuri de imunoterapie utilizate în clinică: inhibitori ai punctelor ...
Chimioterapia citotoxică – principii şi indicaţii în cancer
Lucian MIRON
Chimioterapia cancerului este tratamentul sistemic medicamentos care se bazează pe utilizarea unor substanţe care interferează cu metabolismul şi ciclul celular, determinând moartea celulelor maligne(1,2). Scopul principal al tratamentelor cu agenţi chimioterapici este de a preveni celulele canceroas...
Ketamina în doze mici în analgezie – o nouă abordare?
Sorin Buga, Chandana Banerjee, Heather Bitar, Stefanie Mooney, Purvi Patel
Ketamina, aprobată ca agent anestezic în Statele Unite ale Americii, acţionează ca un antagonist pe receptorii N-methyl-D-aspartat (NMDA), care influenţează toleranţa la opioide, dar şi hiperalgezia produsă de către o...
Factorii de risc social şi sănătatea copilului
Vasile Valeriu Lupu, Anca Lupu, Laura Bozomitu
Societatea actuală este caracterizată prin interacţiunea a noi factori, sociali şi de mediu, care au un anumit impact şi asupra sănătăţii copilului. Identificarea acestor factori şi descrierea influenţelor asupra populaţiei pediatrice, la diferite vârste, sunt elemente esenţiale pentru creştere, dezvoltare, p...