Îngrijirile paliative în stadiul de sfârşit al vieţii în bolile oncologice
Palliative care for end-of-life stage in oncologic disease
Abstract
End-of-life status is a chapter of palliative care that raises interest in the scientific world, but also in medical practice. There is some controversy in the definition and terminology of the terminal state (end-of-life). In this article, we focused on the study of these issues by Canadian researchers, and their study brings important clarifications for practice. We briefly described the main symptoms of the terminal state and their treatment. This article also highlights the role of communication with both the patient and his family at the end-of-life stage. Another aspect, not to be neglected in practice, is the state of bereavement.Keywords
end of lifepalliative carebereavementRezumat
Starea terminală este un capitol al îngrijirilor paliative care suscită interes pentru lumea ştiinţifică, dar şi în cadrul practicii medicale. Există unele controverse în definirea şi diagnosticul stării terminale. În acest articol ne-am oprit asupra interpretării acestor probleme de către cercetătorii canadieni, studiul lor aducând clarificări importante pentru practică. Am descris pe scurt şi principalele simptome ale stării terminale şi tratamentul lor. De asemenea, articolul subliniază rolul comunicării în starea terminală, atât cu pacientul, cât şi cu familia sa. Un ultim aspect prezentat, dar care nu trebuie neglijat în practică, este starea de doliu.Cuvinte Cheie
stare terminalăîngrijire paliativădoliuIntroduction
The definition of the end-of-life care is the following: “Care given to people who are near the end of life, and have stopped treatment to cure or control their disease. End-of-life care includes physical, emotional, social and spiritual support for patients and their families. The goal of end-of-life care is to control pain and other symptoms, so that the patient can be as comfortable as possible. End-of-life care may include palliative care, supportive care and hospice care”(1).
How to explain to the patient: the term “end of life care” can be interpreted as negative and final; however, it is important to realise that receiving this kind of care doesn’t mean that death is imminent or that the medical teams have given up on patient care. “At this challenging time, accessing care can be a very positive step. There will be the support to manage symptoms and maintain comfort and wellbeing, which will maximise joy and fulfilment”(2).
We must emphasize at the begining of this article that the discussion with the family is very important and has at least the same importance as the discussion with the patient.
The family must have a close contact and communication with the physician and the medical staf when the patient is at the end of life. The therapists must guide the family members in this difficult moment, with empathy and wisdom resulted from their experience. Each death experience is unique, individualized according to the attachment to the dying person, and can affect the medical care staff.
The most frequent question addressed to the oncologist is: “How long would the patient live?” The best answer to this request is to explain in simple terms the significance of each sign that appears: the respiratory changes, the skin color modification, the pulse weakening, the drowsiness etc. These explanations can help and guide the family in deciding on the time spent with the patient and on his wish to say goodbye(3-5).
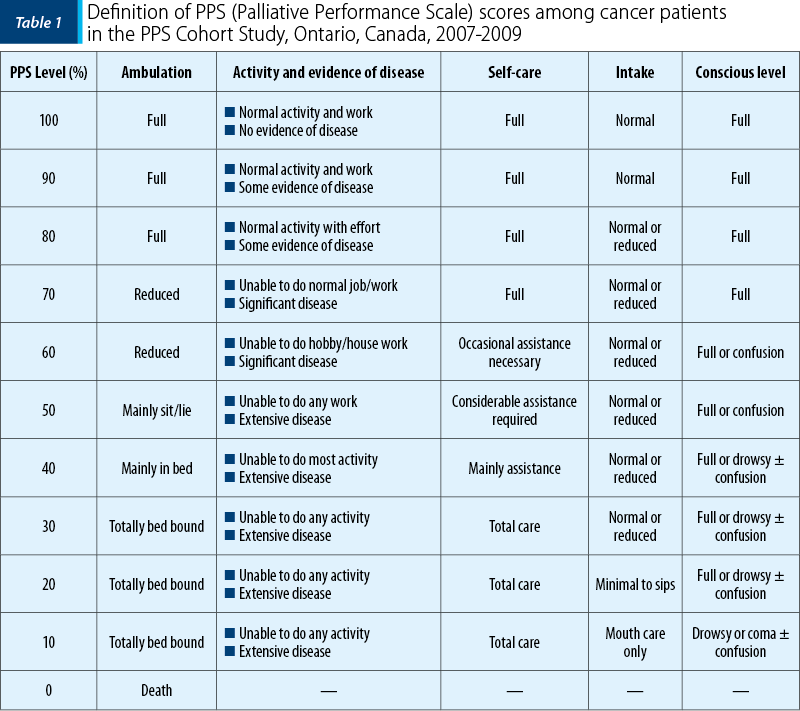
Diagnosis of end-of-life
The investigators of this study assigned patients to one of the four states:
-
Stable (PPS score: 70-100).
-
Transitional (PPS score: 40-60).
-
EOL (PPS score: 10-30).
-
Dead (6).
After the diagnosis of end of life, the palliative care team should make an advanced care planning (ACP). This has been a difficult topic to address to Romanian people. While the exact reasons are unknown, cultural barriers of geography, language, and health literacy are among some of the challenges.
Based on data from multiple statewide needs assessments, ACP and advanced communication skills training are the most requested interventions by doctors with competence in palliative care(7).
When the malignant disease reaches its final stage, the treatment purpose is no longer the cure of the disease or prolonging the survival. The complete understanding of the physical, spiritual and emotional needs of the patient with advanced cancer also involves the recognition of the terminal stage as an important chapter of oncological practice. The terminal stage can be considered when the weight loss exceeds 8 kg in the last three months, the total protein level is less than 35 g/l and LDH level is above 700 UI/l. The main objective is the simptomatic treatment, the relief of the sufferance and improving the quality of life for both the patient and his family. These involve actions in four directions: physical, emotional, spiritual and social(8).
In the last days of their life, before dying, a large number of patients have one or more of the following symptoms:
-
fatigue or pain (70%)
-
anxiety/agitation/delirium, noisy breathing or wet (60%)
-
dyspnea (20%)
-
nausea and vomiting (10%)(9,10).
The care of terminal stage is multilateral, but is focused on the medical control of physical symptoms, being represented by:
-
the need for an optimal relief of the pain
-
the need to relieve other symptoms that cause sufferance and discomfort
-
the physical care is delivered by doctors and trained medical staff, who exhibit a positive attitude for palliative care
-
respect for the patient’s wishes
-
a trustworthy relation and a good communication between the physician, the family and the patient, allowing to overcome the anxiety and preparing the patient and his family for death(11,12).
The treatment of main symptoms
For most problems of the terminally ill patients, the proper attitude is to use a limited number of drugs administered through rectal route, transdermically or – only when necessary – parenterally.
Pain
Pain continues to be the dominant symptom, anxiogenic, and often suboptimally treated in patients with cancer in final stages. Pain has multiple dimensions and is often described as “total pain”.
The treatment of pain in final stages involves:
-
The constant evaluation of medication and the modification regardless its doses, until the cessation of pain, using the WHO “three-step” treatment scale.
-
Morphine is the most powerful election opioid, and it must be administered until the total pain relief.
-
The optimum dose is the one which leads to the total pain relief, with minimum side effects.
Other symptoms
The other symptoms from the end-of-life stages will be treated as they appear, always taking into account that the main goal is the patient’s comfort, and not prolonging the survival (or the cure of the disease).
-
The symptoms must be rapidly evaluated and treated.
-
The optimal interventions on every symptom will be those with the minimum impact on the quality of life. The oncologist will bear in mind this concept, during each decision, and will avoid those measures that are not absolutely necessary, which can lead either to more sufferance, or speed up the unfavorable evolution.
-
The traditional medicine measures are not recommended, neither the useless laboratory analyses, the clinical exploration, nor the permanent monitoring of vital signs, which are not necessary and decrease the patient’s comfort.
Medication
-
As long as the oral administration route is maintained, it is recommended to be used.
-
When food swallowing is no longer possible, or the gastrointestinal absorption is uncertain, an alternative route will be chosen (transdermal, sublingual, subcutaneous or rectal/vaginal). Sedatives and other essential drugs can be administered intravenously only when this route is immediately accesible.
-
The main goal is to use as few as possible invasive procedures, with the maximum benefit.
-
The final anorexia cannot be controled with forced alimentation; there is no medication effective in this case.
Hydration and nutrition
Hydration and nutrition represent one of the most provocative aspects in the care of terminally ill cancer patients. A natural fact of the end-of-life stage is the patient’s refusal to eat and drink. Although the loss of appetite is a process already installed, lasting for days or weeks, at the end-of-life stage the refusal of food and liquids is total. At this moment, the oncologist, at the family request, is inclined to take intravenous hydric measures or to install an enteral tube.
The terminally ill patients don’t need aggressive nutritional support with these procedures. These measures don’t prolong the survival, don’t ameliorate the nutritional status or the weight loss, and don’t make patients feel stronger. As an effect, the enteral tube and the intravenous perfusions increase the distance between patient and his family. Hunger is seldom a source of discomfort. Some literature data suggest that the reduction of food intake causes a euphoric state of mind simillar to that of a healthy person being in a hurry.
The artificial hydration leads to discomfort and will be used only when the patient complains of being thirsty and he is not capable to drink. Dehydration in the terminal stage decreases the pulmonary secretions, increases the dyspnea, and decreases the urinary debit, with the reduction of urinary incontinence and the minimisation of vomiting(13,14).
Modification of mental status in terminally ill patients
When close to death, the patient seems to enter in another dimension, characterised by a short and transitory altering of his consciousness, before the final and total loss of consciousness. This physical state can manifest through restlessness, sorrow, profound sufferance, even to the point when the patient wants to get out of the bed; if the agitation persists, the patient becomes dyspneic and requires an adequate sedation.
At this moment, the family must be gently warned, in order to understand that this state is a final event, part of the disease – probably due to profound hypoxia – that requires sedation, and not a sign of emotional sufferance or death refusal(15-17).
Communication in end-of-life care
Communication about the end-of-life care issues, in line with patients’ and relatives’ readiness and preferences, is essential. This task will become the responsibility of generalists, as well as of the specialist in palliative care providers, and therefore supporting clinicians with this important responsibility should be a priority for practitioners, researchers and policy makers. Although there are potential barriers to opening end-of-life care discussions, it is important to recognise that many of the qualities most valued by patients and relatives are the core, non-specialist communication skills relevant in all fields of medicine – sensitivity and empathy, within holistic, individualised care. It is therefore important not to let the specific sensitivities of palliative care discussions, as highlighted in the literature, deter clinicians from providing all these important opportunities. Sources of support have been developed, and work within this field is ongoing. However, a better understanding of how we define and measure good communication in end-of-life care is essential for future progress(18).
Bereavement support
The provision of bereavement support is an essential component of palliative care team, which is explicitly acknowledged in several seminal national and international publications such as World Health Organization, 2004. While bereavement support is integral to palliative care, it is typically insufficiently resourced, underresearched, and not systematically applied. It may therefore be considered “the forgotten child” of the palliative care family. Traditional views of bereavement are being challenged in contemporary view of thanatology. Grief following bereavement is not a psychiatric disorder, but a normal emotional reaction to loss. However, while loss and grief are fundamental to human life, the course and consequences of bereavement will vary for each individual. For highly resilient individuals, acute grief may be limited to a few weeks, and for most people their grief subsides over time (Bonanno and Kaltman, 2001). For a subgroup of individuals (around 10-15%), the symptoms of distress following the death of a family member or friend are more intense and persistent (Prigerson et al., 1996, 2009; Latham and Prigerson, 2004). Known variously as “complicated grief” (Prigerson et al., 1996; Shear et al., 2011) or “prolonged grief disorder” (Boelen and Prigerson, 2007), this condition can be associated with severe mental and physical health problems such as insomnia, substance misuse, depression, depressed immune function, hypertension, cardiac problems, cancer, suicide, and work and social impairment(19).
Conflict of interests: The author declares no conflict of interests.
Bibliografie
- https://www.cancer.gov/publications/dictionaries/cancer-terms/def/end-of-life-care
- https://myhometouch.com/articles/what-does-end-of-life-care-mean
- Michaud L, Burnand B, Stefelt F. Taking care of terminally ill cancer patients: delirium as symptom of terminal disease. Ann Oncol. 2004; 15 (Suppl 4): iv 199–iv 203.
- Nuland SB. How We Die. New York, Knopf, 1994.
- Twycross RG, Lack SA. Therapeutics in Terminal Cancer, 2nd Edition, Churchill Livingstone, 1990.
- Sutradhar R, Seow H, Earle C, Dudgeon D, Atzema C, Husain A, Howell D, Liu Y, Sussman J, Barbera L. Modeling the Longitudinal Transitions of Performance Status in Cancer Outpatients: Time to Discuss Palliative Care. J Pain Symptom Manage. 2013 Apr; 45(4):726-34.
- https://www.cancer.gov/about-cancer/advanced-cancer/planning/end-of-life-hp-pdq#section/_3
- Miron L. Îngrijirea pacientului cu stare terminală. In: Miron L (ed). Elemente de nursing în cancer, ediţia a II-a, Ed. „Gr. T. Popa” Iaşi, 2018; 651-657.
- Krouse RS, Kamal AH. Specialized care of terminally ill. In: DeVita VT Jr. Lawrence TS, Rosenberg SA (eds). DeVita, Hellman, and Rosenberg’s Cancer Principles and practice of oncology, 11th edition, Wolters Kluwer, 2019; 2242-2247.
- Lister S, Douherty L (eds). End of life. In: The Royal Marsden Manual of Cancer Nursing Procedures. Wiley Blackwell, 2019; 403-415.
- Murphy M, Gross T. Final Hours. In: Neuton S, Hickey M, Brant JM (eds). Mosby’s Oncology nursing advisor. A comprehensive guide to clinical practice, Second edition, Elsevier, 2017; 413-420.
- Heidrich DE. Palliative and end of life. In: Itano JK (ed). Core curriculum for oncology nursing, 5th edition, Elsevier, 2016; 515-530.
- Kamal AH. Palliative medicine for cancer. In: ASCO–SEP® Medical Oncology Self-Evaluation Program, 6th edition, 2018; 248-263.
- Miron L, Stratulat TA. Tratamentele paliative în oncologie. In: Miron L (ed). Oncologie generală, ediţia a III-a, Ed. „Gr. T. Popa” Iaşi, 2016; 399-430.
- Fins JJ. A palliative ethic of care Clinical wisdom at life’s end. Jones and Bartlett Publisherd’s, 2006.
- Kaye P. Notes on symptom control in hospice and palliative care. Educational Institute, Essex, 1992.
- Kubler-Ross E. On death and dying. New Zork, MacMillan, 1969.
- Brighton LJ, Bristowe K. Communication in palliative care: talking about the end of life, before the end of life. Postgrad Med J. 2016; 92:466–470.
- Hudson P, Hall C, Boughey A, Roulston A. Bereavement support standards and bereavement care pathway for quality palliative care. Palliative and Supportive Care. 2018 Aug; Volume 16, Special Issue 4 (Topics in Bereavement), pp. 375-387.

Particularităţile diagnosticului în limfoamele primare ale sistemului nervos central (PCNSL)
Anca Nicolescu, Ana Maria Vlădăreanu, Horia Bumbea, Diana Cisleanu, Raluca Nistor, Ion Dumitru, Tiberiu Sultan
Limfomul primar al sistemului nervos central este o formă rară de limfom extranodal care poate afecta creierul, leptomeningele şi ochiul sau măduva spinării, fără a exista dovezi ale unei boli sist...
Modificările funcţionale ale celulelor canceroase în raport cu celulele normale
Mariana Saulea, Maria Iuliana Gruia
Scopul acestui articol este de a explica ce modificări funcţionale apar atunci când celulele normale se transformă în celule canceroase. Organismul uman este alcătuit din trilioane de celule care cresc, se divid şi mor....
Imagistica multiparametrică de rezonanţă magnetică în diagnosticul cancerului de prostată: o necesitate
Ioana G. Lupescu
Cancerul de prostată reprezintă o importantă problemă de sănătate publică. Imagistica prin rezonanţă magnetică (IRM) este cea mai bună modalitate de evaluare a prostatei şi de a diagnostica cancerul d...
Modificările funcţionale ale celulelor canceroase în raport cu celulele normale
Mariana Saulea, Maria Iuliana Gruia
Scopul acestui articol este de a explica ce modificări funcţionale apar atunci când celulele normale se transformă în celule canceroase. Organismul uman este alcătuit din trilioane de celule care cresc, se divid şi mor....
Managementul cancerului de prostată rezistent la castrare
Lucian MIRON, Teodora Alexa
Cancerul de prostată rezistent la castrare (CRPC) este un aspect important al practicii noastre clinice în fiecare zi. Pentru o perioadă foarte lungă de timp, singura optiune de tratament disponibilă pentru pacienţi a fost chimioterapia cu docetaxel asociat cu prednison. Recenta aprobare în ţara noastră de no...