ORIGINAL ARTICLE
Managementul oboselii în îngrijirile paliative
Management of fatigue in palliative cancer patients
Abstract
Background. Cancer-related fatigue is one of the most frequent symptoms reported by patients, in all stages of the disease. Fatigue is related to secondary causes, such as anemia, electrolytes disorders, malnutrition or to cancer specific therapy (chemotherapy, radiation or biologic treatment) or is related to the disease itself. Material and method. 120 patients admitted in our institution were evaluated regarding intensity of fatigue, using Edmonton Symptoms Assessment Scale (ESAS), and treatment of fatigue. Results and discussion. 83.33% of patients evaluated in our study reported different grades of fatigue. Most of them had low and moderate fatigue (69.16%) and only 14.16% reported severe fatigue. Many researches are focused on fatigue therapy - most of them studied the effect of stimulants, corticoids and non-pharmacological interventions. Conclusions. The intensity of this symptom is reported differently by patient and by the physician, and this is a strong reason for assessing fatigue at every clinical evaluation of the patients in palliative settings. The treatment option with very strong recommendation is based on non-pharmacological intervention.Keywords
fatiguepalliative settingsnon-pharmacological interventionRezumat
Introducere. Oboseala în tumorile maligne solide este una dintre cele mai frecvente simptome raportate de pacienți în toate etapele bolii. Oboseala este legată de cauze secundare, cum ar fi anemie, tulburări de electroliți, malnutriție sau la terapia specifică: chimioterapie, radioterapie sau biologice sau este legat de boala în sine. Material și metodă. 120 de pacienți internați în instituția noastră au fost evaluați în privința intensității oboselii; s-a folosit Scala Edmonton (ESAS) pentru evaluarea simptomelor înainte și după tratament. Rezultate și discuții. 83,33% din pacienții evaluați în studiul nostru au raportat diferite grade de oboseală. Cei mai mulți dintre ei au avut oboseală scăzută și moderată (69,16%) și numai 14,16% au raportat oboseală severă. Multe cercetări sunt concentrate pe terapia oboselii - cele mai multe dintre ele au studiat diverse stimulente, corticoizi și intervenții non-farmacologice. Concluzii. Intensitatea acestui simptom este raportată în mod diferit de pacient și de medic, iar acest lucru este un motiv întemeiat pentru a măsura oboseala la fiecare evaluare clinică a pacienților în îngrijirile paliative. Opțiunea de tratament se bazează pe intervenții non-farmacologice.Cuvinte Cheie
obosealăîngrijiri paliativeintervenții non-farmacologiceBackground
Cancer-related fatigue is defined as a persistent symptom, a subjective feeling of physical, emotional or cognitive tiredness or exhaustion related to cancer or its treatment that is not proportional to the recently performed activity, and which can interfere with the usual patient’s functional capacity; this is the strong recommendation of the National Comprehensive Cancer Network(1,2).Cancer-related fatigue is one of the most prevalent symptoms in cancer patients and it has been recognized by physicians, patients, caregivers, and researchers that fatigue needs clinical attention and strong intervention(3). So, cancer-related fatigue has been accepted as a diagnosis in the International Classification of Diseases, Tenth Revision(3), and clinical practice guidelines for its management have been formulated by the National Institutes of Health and the National Comprehensive Cancer Network (NCCN)(4,5).
Fatigue may be regarded as a single symptom, as a symptom cluster or as a clinical syndrome(6). Fatigue is a subjective symptom and must be assessed at initial clinical evaluation of cancer patients, by self-evaluation and, only in isolated cases (cognitive impairments) can be substituted by estimations of caregivers or medical staff(6). For the single-symptom approach, single item scales (analog-visual scale) have been proposed. For the symptom cluster approach, checklists and questionnaires with multiple dimensions have been validated: Functional Assessment of Cancer Therapy - Fatigue (FACT-F), The brief fatigue inventory (BFI), The EORTC QLQ-C30, The Multidimensional Fatigue Symptom Inventory (MFSI)(6,7,8).
Initially, in the management of fatigue should be considered the secondary causes of fatigue and these must be correctly treated. So, the patient should be evaluated for anemia, depression, thyroid disorders, hypercalcaemia, magnesium imbalance, malnutrition, too. Most of the patients with cancer-related fatigue will benefit from the non-pharmacological treatment, such as exercises, cognitive behavioral therapy, and sleep intervention. Symptomatological pharmacological treatment is based on stimulants, such as methylphenidate, modafinil, pemoline and donazepil, and corticoids(2,4,6).
In the final stage of life, fatigue may provide protection and shielding from suffering for the patient and treatment of fatigue may be detrimental(6).
Materials and method
120 patients diagnosed with advanced loco-regional or metastatic cancer were admitted in the Department of Oncology, Palliative Care for Chronic Patients of “St. Luca” Chronic Diseases Hospital, in Bucharest, Romania, over a period of two weeks. In May 2016, they were evaluated regarding intensity of fatigue, using Edmonton Symptoms Assessment Scale (ESAS), and treatment of fatigue. The severity of fatigue at the time of assessment is rated from 0 to 10 on a numerical scale, with 0 meaning that the symptom is absent, 1-3 meaning low intensity of fatigue, 4-6 meaning moderate intensity of fatigue, and 7-10 representing severe level of fatigue.The participants were explained the purpose and the importance of the study and the patients signed a written informed consent, in which they freely agreed to join the study. The approval from the Medical Ethical Commission of “Sf. Luca” Chronic Diseases Hospital has been previously obtained.
Data obtained were analyzed using Microsoft Office Excell 2013.
Results
According to the usual age groups (30-45, 46-60 and over 60 years old), the patients’ distribution was the following: 8 (6.67%) in the 35-45 years old group, 32 (26.67%) in the 46-60 years old group, and 80 (66.67%) in the over 60 years old group.The patients’ distribution according to gender was: males 73 (60.83%) and females 47 (39.17%).
The patients’ distribution according to life environment was the following: urban 100 (83.33%) and rural 20 (16.67%).
Moreover, the patients’ distribution according to the disease diagnosis was the following: Lung - 46 (38.33%), Breast - 16 (13.33%), Colorectal - 15 (12.50%), Prostate - 11 (9.17%), Ovary - 4 (3.33%), Bladder - 3 (2.50%), Gastric - 3 (2.50%), Head and neck - 3 (2.50%), Pancreatic - 3 (2.50%), Renal - 3 (2.50%), Hepatobilliary - 3 (2.50%), Cervix - 2 (1.67), Endometrium - 1 (0.83%), Mediastinum - 1 (0.83%), Sarcoma of bones - 1 (0.83%), Small Intestine - 1 (0.83%), Pelvioabdominal - 1 (0.83%), Penis - 1 (0.83%), Unspecified - 1 (0.83%), Ureter - 1 (0.83%).
Patients’ distribution regarding local advanced or metastatic disease was the following: 69 (57.50%) presented local advanced disease and 51 (42.50%) presented metastatic disease.
Discussion
According to our study, patients reported no fatigue (visual analogue scale = 0), or low intensity of fatigue corresponding to grade 1 fatigue on National Cancer Institute Common Toxicity Criteria, ECOG, Eastern Cooperative Oncology Group; NCI CTC (increased fatigue in relation to the baseline situation, but without interfering with normal activities), moderate intensity of fatigue corresponding to grade 2 fatigue (worsening of performance status by 20% for the Karnofsky score or by one point in the ECOG scale or difficulty in carrying out some activities) and severe fatigue corresponding to grade 3 and 4 fatigue (worsening of the performance status by 40% for the Karnofsky score or by two points in the ECOG scale or loss of capacity to carry out some activities and bed bound or severe disability).In a study of 1000 patients in palliative care from an American Palliative Care Program, three of the five most reported symptoms were fatigue (in 84% patients), weakness (in 66% patients) and lack of energy (61% patients)(9). Fatigue has been reported in 65-100% of patients following radiotherapy and up to 82-96% of those receiving chemotherapy(10,11) during their treatment. 83.33% of patients evaluated in our study reported different grades of fatigue, most of them having low and moderate fatigue (69.16%) and only 14.16% of patients reported severe fatigue.
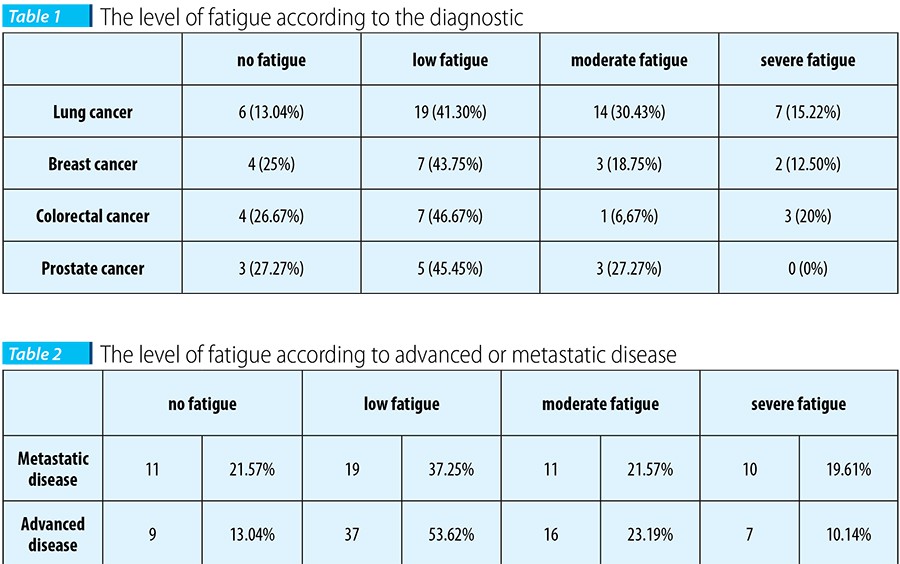
From an analysis of the published data, it emerged that low grade fatigue is present in approximately 30% (on average) of treated patients, while only approximately 10% reported severe grade fatigue, according to the type of patient, cancer type, the treatment and the dose intensity of the chemotherapy(12). However, cancer site does not seem to influence significantly the degree of fatigue(12).
86.96% of patients with lung cancer had different levels of fatigue, most of them reporting low and moderate levels of fatigue (71.73%). The same description of this symptom was found in patients with breast cancer - 75% of patients had different levels of fatigue and 62.50% had low and moderate levels of fatigue - and in patients with prostate cancer (72.72% with low and moderate levels of fatigue). There were differences between the results of the study and the expectancy of the investigators, especially in prostate cancer patients, who seemed to have a very good performance status and a very good tolerance of the specific treatment.
It is known that the prevalence and the impact of fatigue often have not been recognized by physicians(13). In a US survey, more than half of the patients reported that they had never talked about fatigue with their physician and the two most frequent reasons for this were the doctors’ failure to offer interventions and the patients’ lack of awareness of effective treatments(14).
In the last years, the studies focused on fatigue treatment to increase the quality of life. Pharmacological treatments include central nervous system stimulants and erythropoietin-stimulating agents in patients with chemotherapy and hemoglobin levels <10 mg/dL and corticosteroids in patients with terminal disease and severe fatigue(2,6). Research on symptomatic treatment of fatigue, in palliative care, has been concentrated on stimulant drugs such as methylphenidate, modafinil, dexmethylphenidate, pemoline and donazepil. The routine use of these drugs in palliative care patients was considered controversial in the expert group because the available evidences are being too poor(6).
The potentially useful interventions in cancer-related fatigue are: the correction of metabolic disorders, anemia, depression, insomnia, modifications in periods of activity and rest (diary), cognitive therapy, behavioral therapy to modify sleep (sleep hygiene) and nutritional support(12). In women with breast cancer receiving chemotherapy, exercise can significantly reduce the level of fatigue, and as the duration of exercise increases, the intensity of fatigue declines(15). In patients with melanoma receiving interferon-α, the combination of exercise and methylphenidate showed a positive effect on interferon-induced fatigue(16).
The management of fatigue in our patients included corticosteroids and light physical exercise program.
Conclusions
Fatigue is one of the most frequent symptom in cancer patients with advanced and metastatic disease and seems to be more pronounced in lung cancer in association, probably, with dyspnea. The intensity of this symptom is reported differently by patient and by the physician and this is a strong reason for assessing fatigue at every clinical evaluation of the patients in palliative settings.The treatment of the fatigue rest limited to non-pharmacological interventions and the results are inconsistent.
Limitation of the study: a multicenter study with a larger sample size would allow for more definite conclusions. n
Bibliografie
1. Mock V, Atkinson A, Barsevick AM, Berger AM, Cimprich B, Eisenberger MA et al. Cancer-related fatigue. Clinical Practice Guidelines in Oncology. J NatlComprCancNetw. 2007; 5(10):1054-78. Review.
2. Campos, MairaPaschoin de Oliveira, Hassan, Benjamin Joseph, Riechelmann, Rachel, & del Giglio, Auro. (2011). Cancer-related fatigue: a review. Revista da Associação Médica Brasileira, 57(2), 211-219.
3. Maarten H., Julie R., Colmar F.M, Pascal J.P., GaryM., Cancer-Related Fatigue: The Scale of the Probleme, TheOncologist, May 2007, Vol.12-Supllement1 4-10.
4. Mock V, Atkinson A, Barsevick AMet al. NCCN Practice Guidelines for Cancer-Related Fatigue. Oncology (Williston Park) 2000;14:151–161.
5. National Institutes of Health Consensus Development Panel. Symptom Management in Cancer: Pain, Depression, and Fatigue. Available at http://www.guideline.gov/summary/summary.aspx?doc_id=6108. Accessed April 27, 2006.
6. Radbruch L, Strasser F., Elsner F., Gonçalves J.F.,Løge J., Kaasa S.,Nauck F., Stone P., and the Research Steering Committee of the European Association for Palliative Care (EAPC), Fatigue in palliative care patients - an EAPC approach, Palliat Med January 2008 22: 13-32.
7. Mendoza TR, Wang XS, Cleeland CS et al. The rapid assessment of fatigue severity in cancer patients: use of the Brief Fatigue Inventory, Cancer 1999; 85: 1186–1196.
8. Stein KD, Martin SC, Hann DM et al. A multidimensional measure of fatigue for use with cancer patients. Cancer Pract 1998; 6: 143–152.
9. Walsh D, Donnelly S, Rybicki L. The symptoms of advanced cancer: relationship to age, gender, and performance status in 1,000 patients. Support Care Cancer 2000; 8:175–9.
10. Stasi R, Abriani L, Beccaglia P, Terzoli E, Amadori S. Cancer-related fatigue: evolving concepts in evaluation and treatment. Cancer 2003; 98: 1786–801.
11. Escalante CP. Treatment of cancer-related fatigue: an update. Support Care Cancer 2003; 11: 79–83.
12. Iop A., Manfredi A. M., Bonura S., Fatigue in cancer patients receiving chemotherapy: an analysis of published studies, Ann Oncol (2004) 15 (5): 712-720.
13. Vogelzang NJ, Breitbart W, Cella D et al. Patient, caregiver, and oncologist perceptions of cancer-related fatigue: results of a tripart assessment survey. The fatigue coalition. SeminHematol 1997; 34: 4–12.
14. Passik SD, Kirsh KL, Donaghy K et al. Patient-related barriers to fatigue communication. Initial validation of the fatigue management barriers questionnaire. J Pain Symptom Manage 2002; 24: 481–93.
15. Schwartz AL, Mori M, Gao R et al. Exercise reduces daily fatigue inwomen with breast cancer receiving chemotherapy. Med Sci Sports Exerc, 2001; 33: 718–723.
16. Schwartz AL, Thompson JA, Masood N. Interferon-induced fatigue inpatients with melanoma: a pilot study of exercise and methylphenidate, Oncol Nurs Forum 2002; 29: E85–E90.
Articole din ediția curentă

EDITORIAL
News from ASCO
Alexandru Grigorescu
An experimental monoclonal antibody has demonstrated promising results in neuroblastoma, according to new findings....
REVIEW
Tiolii albuminici - potențiali markeri ai statusului oxidativ în cancer
Maria Iuliana Gruia, Andreea Mirica
Stresul oxidativ a fost asociat, pentru o lungă perioadă de timp, cu fiziopatologia cancerului și a altor boli. Speciile reactive generate în exces duc la creșterea instabilității genomului care cauzează distrugeri ale A...
REVIEW
Radioterapia stereotactică - principii şi aspecte practice
Ciprian Enăchescu, Sena Yossi
Radioterapia stereotactică este o formă de iradiere externă care distribuie într-o şedinţă unică sau în câteva şedinţe doze mari de iradiere în volume-ţintă mici, tratament ce necesită o distribuţie a dozei extrem de precisă, astfel încât doza maximă să fie distribuită în volumul tumoral şi să scadă rapid per...Articole din edițiile anterioare
PALLIATIVE AND SUPPORTIVE CARE
Tratamentul antitrombotic la pacienţii cu cancer
Anda Natalia Ciuhu, Mihaela Popescu, Roxana-Andreea Rahnea-Niţă, Loredana Antuanela Tuinea, Gabriela Rahnea-Niţă
Complicaţiile tromboembolice în cancer sunt cauza principală de morbiditate şi mortalitate. Prin urmare, prevenirea şi tratamentul acestei complicaţii contribuie la creşterea supravieţuirii şi calitatea vieţii la pacienţ...