Adenopatia metastatică primitivă cervicală din perspectiva medicului ORL
ENT private eye for unknown primary metastatic lymph nodes
Abstract
Primitive metastatic cervical lymph nodes are defined in the context of an unknown primary tumor at the level of the superior respiratory tract. Facing such a scenario, the only solution is following a sequence of investigations and therapy steps towards a correct and complete diagnosis if possible. We review the current literature data and present a personal case. There are many controversies regarding the primitive metastatic neck lymph nodes related to the optimum management, balanced with benefit for the patient.Keywords
unknownprimarymetastaticlymphnodesRezumat
Metastazele primare de la nivelul ganglionilor cervicali sunt definite în contextul unei tumori primare necunoscute de la nivelul tractului respirator superior. În faţa unui asemenea scenariu, singura soluţie este urmarea unei secvenţe de investigaţii şi de paşi terapeutici pentru un diagnostic corect şi complet, dacă este posibil. În acest articol, trecem în revistă datele actuale din literatură şi prezentăm un caz din experienţa proprie. Există numeroase controverse privind metastazele primare de la nivelul ganglionilor gâtului, în legătură cu managementul optim, benefic şi pentru pacient.Cuvinte Cheie
necunoscutprimarmetastaticlimfaticganglionIntroduction
The major aspect influencing the prognosis of patients with carcinomas of superior airways is the status of neck lymph nodes on admission. Metastasis at this level reduces the survival with almost 50%(1).
Regional lymph nodes drainage at the level of head and neck is sequential and predictable. Understanding the metastasis pattern for every primary site is necessary for establishing the surgical management. Recording the lymph nodes metastasis was standardized by Head and Neck service at Sloan-Kettering Memorial Cancer Center for groups I to V. Afterwards, the system was improved by the American Academy of Otolaryngology – Head and Neck Surgery (AAOHNS) with groups VI and VII and A and B subgroups for levels I, II and V(2).
The distribution of neck lymph nodes metastasis could be summarized as following: oral cavity tumors will drain to groups I to III; masses from pharynx and larynx will go to groups II to IV on the same side; midline tumors present a risk for metastasizing bilaterally(3).
This pathology is defined as a lymph neck node metastasis with an occult primary tumor. Approximately 10% of the cases with neck cancer have an unknown primary site. Most frequently involved lymph nodes are in more than 70% of the cases in group II(4).
Taking into consideration the site of the lymph nodes metastasis, the primary tumor has an increased probability of situation as follows: group I in the lower lip and tip of the tongue; group IIA in the palatine tonsils, tongue border; group IIB in the rinopharynx; group III in the pharynx and larynx; group IV in the thyroid, esophagus and lungs; group V in the cavum, lungs, breast and stomach(5).
Usually, the sites for unknown primary tumors are nasopharynx, tongue base and palatine tonsils. Cystic metastasis is encountered in cases with primary tumor at the level of the palatine tonsils and thyroid carcinomas. It may be mistaken for brachial cysts(6).
Diagnosis principles(7)
-
Complete general exam and head and neck clinical exam.
-
Endoscopy of the nasal, pharynx and larynx cavities, superior digestive endoscopy and bronchoscopies.
-
CT and MRI scans.
-
Thorax CT scan.
-
Fine needle aspiration or core biopsy.
-
Targeted serial biopsies from subject regions.
-
Exploratory neck biopsy with pathology exam and supplementary immunohistochemistry studies.
Management of primary metastatic lymph nodes
Current management guidelines rely on fine needle aspiration biopsy of the cervical mass. Unfortunately, this approach is prone to error due to the level of expertise of the pathology laboratory regarding the cytology diagnosis of malignancy. Therefore, frequently there is used the excision of lymph node for diagnosis(8).
In case of confirmation of a tumor, it is necessary to perform CT and PET scans. Contrast CT scan reveals the dimensions, number and extent of lymph nodes metastasis. PET scan may show the primary occult site in a small number of cases. Due to the decreased accessibility to PET scans alternatively, the case should benefit from whole body CT scan in search for the primary tumor(9).
Further investigations are endoscopy under general anesthesia for increased comfort of the patient and the specialist. Any firm or easily bleeding surface should raise the suspicion of a primary site and these areas should be biopsied. Serial blind biopsies are not recommended due to little probability of identifying the primary site(10).
Another supplementary step is the same side tonsillectomy, because the primary tumor may be hidden in tonsil crypts(11).
Pathology exam of primitive metastatic lymph nodes
Most of the primitive metastatic lymph nodes are manifestations of squamous cell carcinoma with reduced levels of differentiation. The primary tumor may reside in a salivary gland of the upper half of the neck. Inferiorly it may come from thyroid gland. If cytology reveals melanoma, a thorough analysis of the entire skin is necessary. In case of a lymphoma, open biopsy is necessary for diagnosis certainty(12).
Therapeutic management
In these cases, with unknown primary site, the therapy decision is based on the site and extension of neck lymph nodes involvement. Radical neck dissection is the gold standard, in spite of esthetic or functional sequels. The preservation of the 11th nerve reduces the morbidity of the surgery. On the other hand, the conservation of internal jugular vein or of the sternocleidomastoid muscle has a high rate of failure. In N1 cases it is recommended the Functional Neck Dissection, and in 90% of the cases the surgical treatment is sufficient(13,14).
Radiation therapy is required in cases with at least one positive lymph node larger than 3 cm. There must be irradiated both neck sides and the areas with an increased potential risk for primary site. Associating chemotherapy is required by rupture of the lymph node capsule. Recurring lymph nodes benefit from salvage surgery or additional radiation therapy if possible(15).
Clinical case presentation
We present the clinical case of a 47-year-old patient, chronic smoker and drinker, with a high right lymph node, associating pain, with a progressive evolution for the last three months. The initial exam reveals the lymph node pertaining to Va group, associating recurrent right nerve palsy and right hypoglossal palsy. We cannot visualize a primary tumor at this stage. The patient underwent tonsillectomy in childhood, and has minimal hypertrophy of the lingual tonsils and no mass in the tongue base.
Neck CT scan with contrast i.v. underlines the malignant aspect of the lymph node with central necrosis, adherence to the right internal jugular vein, and without other primary lesions (Figure 1).

The surgical management of this case consisted in an exploratory right cervicotomy with the dissection of a right lymph node situated behind the jugular vein and infiltrating the vein (Figure 2).

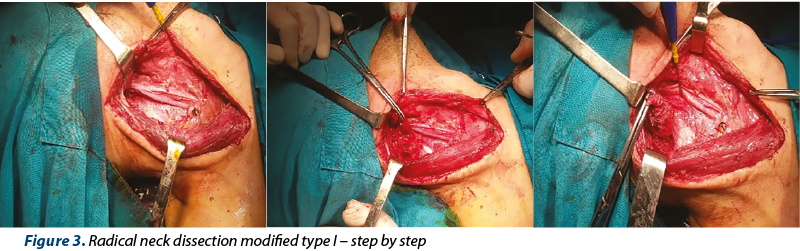
We observed the lymph node necrosis and engulfment of the cranial nerves 11 to 12 and cervical plexus. We performed radical neck dissection modified type I, with the preservation of the 11th cranial nerve (Figure 3).
The pathological exam suggests the diagnosis of invasive squamous carcinoma metastasis, sustained also by immunohistochemistry exam.
After surgery, the cervical MRI and 4-week PET scan underlined a lesion in the right tongue base, but without clinical correspondence on serial endoscopic exams. Chronic local pain was controlled with mild antiinflammatory compounds.
The oncology committee decided in favor for radiation therapy with associated chemotherapy with percutaneous endoscopic gastrostomy feeding during the treatment. The case was monitored for 16 months, without the apparition of the primary tumor on serial subsequent endoscopic investigations.
Discussion
In the case of an unknown primary neck lymph node metastasis, it is necessary to perform a complete thorough screening for the primary tumor. This endeavor is both complex and costly, as the surgeon leaves the comfort of established treatment protocols towards entering the realm of individualized therapy. All the aforementioned steps should be followed. These cases should never be abandoned during oncology treatment as the primary site may become evident even after a number of years from the moment of initial presentation. Our opinion is that these cases are either insufficiently investigated in the initial steps of diagnosis, or the primary tumor is under the current level of diagnostic accuracy of our imaging modalities.
Conclusions
Unknown primary neck lymph nodes metastasis represents a fight under time control with a partially invisible enemy. The correct management of such complex cases should reunite a team of ENT surgeon, radiation therapist, oncology specialist and the patient himself for an optimum result. The success is measured in survival and quality of life, although the ENT surgeon may remain a “private eye investigator” for a number of years even after the surgical removal of the lymph node.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Shah JP. Patterns of cervical lymph node metastasis from squamous carcinoma of the upper aerodigestive tract. Am J Surg. 1990; 160: 405-9.
- Shah JP. Head and Neck Surgery and Oncology, Fourth Edition, 2012.
- Medina JE, Lore JM Jr. Cervical Lymph Node Metastatic Guide. Lore & Medina. An Atlas of Head and Neck Surgery, Fourth edition, 2005, Elsevier Inc., 781-6.
- Müller von der Grün J, Tahtali A, Ghanaati S, Rödel C, Balermpas P. Diagnostic and treatment modalities for patients with cervical lymph node metastases of unknown primary site – current status and challenges. Radiat Oncol. 2017 May 10; 12(1):82.
- López F, Rodrigo JP, Silver CE, Haigentz M Jr, Bishop JA, Strojan P, Hartl DM, Bradley PJ, Mendenhall WM, Suárez C, Takes RP, Hamoir M, Robbins KT, Shaha AR, Werner JA, Rinaldo A, Ferlito A. Cervical lymph node metastases from remote primary tumor sites. Head Neck. 2016 Apr; 38 Suppl 1:E2374-85.
- Katabi N, Lewis JS. Update from the 4th Edition of the World Health Organization Classification of Head and NeckTumours: What Is New in the 2017. WHO Blue Book for Tumors and Tumor-Like Lesions of theNeck and Lymph Nodes. Head Neck Pathol. 2017 Mar; 11(1):48-54.
- Du C, Ying H, Zhang Y, Huang Y, Zhai R, Hu C. Treatment for retropharyngeal metastatic undifferentiated squamous cell carcinoma from an unknown primary site: results of a prospective study with irradiation to nasopharyngeal mucosa plus bilateral neck. Oncotarget. 2017 Jun 27; 8(26):42372-42381.
- Seol YM, Choi YJ, Lee BJ, Wang SG. Induction chemotherapy followed by radiotherapy in patients with cervical lymph node metastases from unknown primary carcinoma. Indian J Otolaryngol Head Neck Surg. 2015 Mar; 67(Suppl 1):74-8.
- Gődény M, Lengyel Z, Polony G, Nagy ZT, Léránt G, Zámbó O, Remenár É, Tamás L, Kásler M. Impact of 3T multiparametric MRI and FDG-PET-CT in the evaluation of occult primary cancer with cervical node metastasis. Cancer Imaging. 2016 Nov 4; 16(1):38.
- Lou J, Wang S, Wang K, Chen C, Zhao J, Guo L. Squamous cell carcinoma of cervical lymph nodes from an unknown primary site: The impact of neck dissection. J Cancer Res Ther. 2015 Oct; 11 Suppl 2:C161-7.
- Yasui T, Morii E, Yamamoto Y, Yoshii T, Takenaka Y, Nakahara S, Todo T, Inohara H. Human papillomavirus and cystic node metastasis in oropharyngeal cancer and cancer of unknown primary origin. PLoS One. 2014 Apr 21; 9(4):e95364.
- Chernock RD, Lewis JS. Approach to metastatic carcinoma of unknown primary in the head and neck: squamous cell carcinoma and beyond. Head Neck Pathol. 2015 Mar; 9(1):6-15.
- Hemminki K, Bevier M, Sundquist J, Hemminki A. Site-specific cancer deaths in cancer of unknown primary diagnosed with lymph node metastasis may reveal hidden primaries. Int J Cancer. 2013 Feb 15; 132(4):944-50.
- Takes RP, Kaanders JH, van Herpen CM, Merkx MA, Slootweg PJ, Melchers WJ. Human papillomavirus detection in fine needle aspiration cytology of lymph node metastasis of head and neck squamous cell cancer. J Clin Virol. 2016 Dec; 85:22-26.
- Mistry RC, Qureshi SS, Talole SD, Deshmukh S. Cervical lymph node metastases of squamous cell carcinoma from an unknown primary: outcomes and patterns of failure. Indian J Cancer. 2008 Apr-Jun; 45(2):54-8.

Abstracte Forum ORL.ro 2019
Lista rezumatelor lucrărilor susţinute in cadul celei de-a XI-a ediţii a Forumului ORL.ro 2019...
Aspectul endoscopic al procesului uncinat
Vlad Andrei Budu
Apofiza unciformă (procesul uncinat) reprezintă lamela anterioară a etmoidului (first lamella), fiind primul reper abordabil chirurgical endoscopic în timpul etmoidectomiei. În mod obişnuit, procesul uncinat se vizualizează prin medializarea cornetului mijlociu, dimensiunea sa permiţând ventilaţia meatului me...
Anomaliile neevolutive de structură ale smalţului dentar
Andrei Kozma, Ioana Monica Teodorescu, Cristian Teodorescu
Prin această lucrare ne propunem prezentarea succintă a anomaliilor neevolutive de structură ale smalţului din punct de vedere clinic şi a etiologiei acestora, precum şi conştientizarea medicului dentist şi a pacienţilor.../32 - Maxillomandibular skeletal repositioning and the upper airways.webp)
Repoziționarea scheletală maxilomandibulară și căile respiratorii superioare: rezultate funcționale în cazurile de chirurgie ortognatică
Remus Chirciu, Matei Dumitru, Bogdan Bănică, Mircea Laslău, Rareş Oancă, Lorena Păun, Ionuț Costin, Daniela Vrînceanu
Repoziționarea scheletală maxilomandibulară (MSR) modifică relațiile spațiale ale limbii, palatului moale și pereților faringieni ...
Septoplastia endoscopică – indicaţii, avantaje și dezavantaje
Bianca Buleandra, Simona Georgescu, Remus Chirciu, Rareș Oanca, Lorena Păun, Ionuț Costin, Miruna Bratiloveanu, Ioana Eftime, Mihai Dumitru, Daniela Vrînceanu
Septoplastia endoscopică este o tehnică modernă, minim invazivă, utilizată pentru corectarea deviațiilor septale, oferind o vizua...